

Non-traumatic spontaneous rupture of the kidney in subjects on chronic hemodialysis is a rare event. In most cases it is associated with acquired cystic kidney disease (ACKD)[1] or the presence of kidney cancer.[2] There are few reports on this topic. Until 2009 Goto identified in the Japanese literature only five reports of renal cell carcinoma in patients with end-stage renal disease (ESRD) manifesting with spontaneous rupture.[3] In the general population primary neoplasms of the renal pelvis are uncommon and most are malignant. The majority of these cases consist of transitional cell carcinoma. Squamous cell carcinoma (SCC) and adenocarcinoma (AC) of the renal pelvis are highly uncommon tumors and constitute less than 1% of upper urinary tract neoplasms.[4] SCC and AC are known to be associated with chronic renal calculi and infection. The incidence of coexisting urinary stone disease varies from 18% in the United States to 100% in Hong Kong.[5,6] The pathogenesis of SCC and AC associated with renal calculi is well documented. The process is assumed to begin with urothelial metaplasia due to chronic irritation and this leads to dedifferentiation and finally SCC or AC.[7]
A 62-year-old woman, suffering from diabetes mellitus and coronary artery disease presented with acute and sudden flank pain on the left side. She had received right nephrectomy 10 years ago because of bilateral nephrolitiasis. For last 2 years she was on maintenance hemodialysis three times a week. She was totally anuric. She was not receiving oral anticoagulant therapy. CT scan abdomen on arrival showed left kidney significantly increased in volume with inhomogeneous structure, presence of large staghorn calculus in the left renal pelvis, other lower calyceal calculi, and massive hematoma in the lower third of the kidney [Figure 1]. Laboratory tests showed severe anemia (Hb: 6.3 g/dl); coagulation and liver function tests were within the normal range. An emergency left nephrectomy was performed. Macroscopic finding was a kidney with a size of 16 cm in length, covered by coagula with ruptured renal capsule. On the cross-section analysis, we observed thinning of the cortex, cystic dilatation of the collecting system, with several calculi and a copious amount of brownish liquid, large hemorrhagic collection extended to perirenal adipose tissue. Pathological examination revealed a well-differentiated squamous cell carcinoma of the renal pelvis, infiltrating the adipose tissue and the parenchyma. Histological grading UICC: G1-pT3 [Figures 2 and 3].
Figure 1.

Renal CT scan: Right side empty. Left kidney significantly increased in volume; staghorn calculus in renal pelvis and other calyceal stones; huge perirenal hematoma
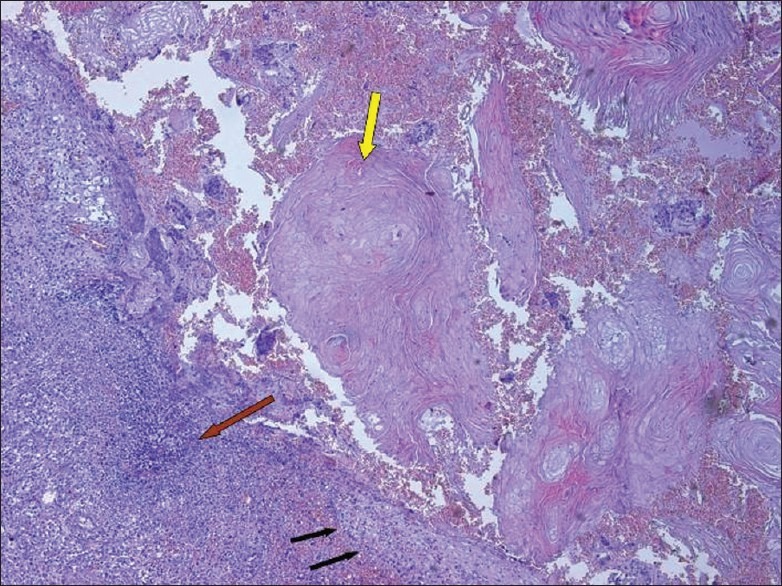
Figure 2.
Renal biopsy: Fracture of the renal parenchyma with inflammatory infiltrate and squamous epithelium layer (H and E, ×10)
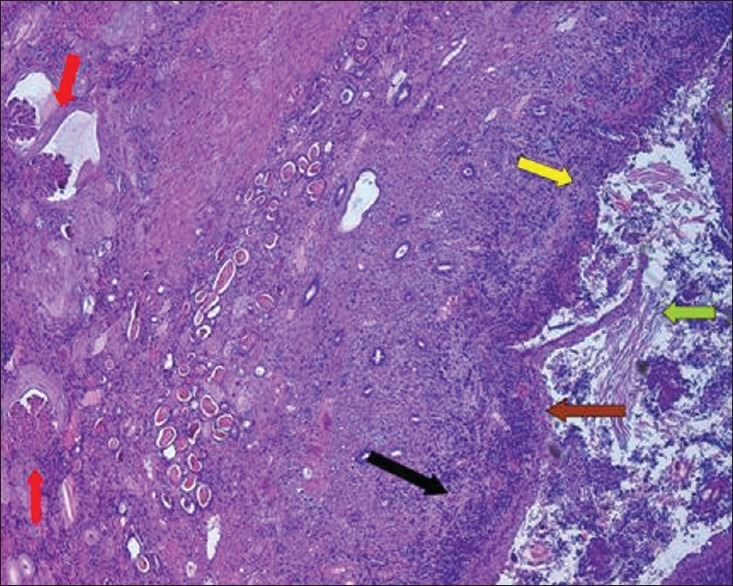
Figure 3.
Renal biopsy. Left kidney: Squamous metaplasia in renal pelvic epithelium layer (H and E, ×10)
There are a few studies regarding the urothelial carcinoma in patients with ESRD.[8] Renal calculi are a risk factor for the development of squamous cell carcinoma. The native kidneys, though no longer functioning, suffer from the chronic irritation from kidney stones. Therefore the patients on maintenance dialysis with long-standing nephrolithiasis should be monitored.
Footnotes
Source of Support: Nil
Conflict of Interest: No.
References
- 1.Borràs M, Valdivielso JM, Egido R, Vicente de Vera P, Bordalba JR, Fernández E. Haemoperitoneum caused by bilateral renal cyst rupture in an ACKD peritoneal dialysis patient. Nephrol Dial Transplant. 2006;21:789–91. doi: 10.1093/ndt/gfi298. [DOI] [PubMed] [Google Scholar]
- 2.Matsui F, Kobori Y, Amano T, Takemae K, Suzuki T. Renal cell carcinoma in acquired cystic disease of the kidney manifested by spontaneous renal rupture. Hinyokika Kiyo. 2003;49:239–41. [PubMed] [Google Scholar]
- 3.Goto T, Sengiku A, Sawada A, Shibasaki N, Ishitoya, Sokumura K. Bilateral renal cell carcinoma of dialysis patient manifesting as spontaneous renal rupture. Hinyokika Kiyo. 2009;55:707–10. [PubMed] [Google Scholar]
- 4.Papadopoulos I, Wirth B, Jacobsen KW, Loch T, Wacker HH. Primary squamous cell carcinoma of the ureter and adenocarcinoma of the renal pelvis: 2 case reports. J Urol. 1996;155:288–9. [PubMed] [Google Scholar]
- 5.Li MK, Cheung WL. Squamous cell carcinoma of the renal pelvis. J Urol. 1987;138:269. doi: 10.1016/s0022-5347(17)43116-8. [DOI] [PubMed] [Google Scholar]
- 6.Blacher EJ, Johnson DE, Karim FW, Ayala AG. Squamous cell carcinoma of renal pelvis. Urology. 1985;25:124–6. doi: 10.1016/0090-4295(85)90526-6. [DOI] [PubMed] [Google Scholar]
- 7.Raghavendran M, Rastogi A, Dubey D, Chaudhary H, Kumar A, Srivastava A, et al. Stones associated renal pelvic malignancies. Indian J Cancer. 2003;40:108–12. [PubMed] [Google Scholar]
- 8.Hung PH, Shen CH, Tsai HB, Hsiao CY, Chiang PC, Guo HR, et al. Urothelial carcinoma in patients with advanced kidney disease: A 12-year retrospective cohort survey. Am J Med Sci. 2011;342:148–52. doi: 10.1097/MAJ.0b013e318223e800. [DOI] [PubMed] [Google Scholar]