

Summary
This review analyzed the literature focused on Cone- Beam Computed Tomography (CBCT) diagnostic accuracy and efficacy in detecting impacted maxillary canines, and evaluated the possible advantages in using CBCT technique compared with traditional radiographs. PubMed and Embase searches were performed selecting papers since 1998 up to September 2011, moreover reference lists were hand searched. Two reviewers selected relevant publications on the basis of predetermined inclusion criteria. The literature search yielded 94 titles, of which 5 were included in the review. Three studies used CBCT technique to 3D localize maxillary impacted canines and assess root resorption of adjacent teeth. Other two publications compared traditional radiographs with CBCT images in the diagnosis of maxillary impacted canines. Only three studies presented the results using statistical analysis. The present review highlighted that the use of CBCT has a potential diagnostic effect and may influence the outcome of treatment when compared with traditional panoramic radiography for the assessment of impacted maxillary canines. Furthermore it underlines the need of future studies performed according with high level methodological standards, investigating diagnostic accuracy and effectiveness of CBCT in the diagnosis of maxillary impacted teeth.
Keywords: cone-beam computed tomography, volumetric computed tomography, maxillary impacted canine
Introduction
Maxillary canines have the highest frequency of impacted localization after the third molars, with a prevalence ranging from 1% to 3% (1–4), and with a 2:1 female to male ratio (5). Impacted maxillary canines lead to aesthetic and functional drawbacks: alteration in the aesthetic of the smile, resorption of lateral incisors, cystic degeneration (5). Moreover, their surgical and orthodontic management is not easy and time consuming to treat. Consequently, the accurate localization of impacted maxillary canines is essential, especially if surgical intervention is required.
In the daily practice the first radiographic image that is required to support the clinical examination is the panoramic radiography. The localization of impacted teeth can be improved radiographically using a combination of other bi-dimensional images: occlusal and periapical, which allow the localization of impacted canines, treatment planning, and evaluation of the treatment result. However the diagnostic accuracy of these bi-dimensional radiographic techniques presents many limitations such as distortion projection errors, blurred images and overlapping of structures, thus increasing the risk of the lack of some important information. In the modern practice the localization of impacted maxillary canines and the assessment of lateral root resorption can be drastically improved using information obtained from 3D investigations. Several previous studies used Computed Tomography (CT) (6–9). However, the high effective dose and the relatively high costs limit the use of this technique in the daily practice. With the introduction of low dose volumetric CT system, Cone Beam Computed Tomography (CBCT), clinicians can take advantages from 3D information provided by a low radiation dose and with relatively low costs.
The aim of this study was to evaluate the evidence for the diagnostic accuracy of CBCT in detecting impacted maxillary canines and to analyze the literature focused on the comparison between the diagnostic effectiveness of CBCT with that of conventional radiography in the localization of impacted maxillary canines and the assessment of adjacent roots resorption.
Materials and methods
The PRISMA 2009 Checklist (10) was used to conduct this review. Only Studies that matched (at least) one of the following inclusion criteria were selected: (1) studies that detected impacted maxillary canines with CBCT; (2) studies that described diagnostic and/or therapeutic accuracy and efficacy of CBCT technique in the diagnosis of maxillary impacted canines and incisors roots resorption; (3) studies that compared the efficacy of CBCT with that of conventional radiographic images in diagnosis of impacted maxillary canines.
The in vitro studies were excluded. No language limitations were applied.
The following electronic data bases were searched from 1998 up to September 2011: PubMed and Embase. The choice of that time period was justified by the introduction in the late 1990s of CBCT in the clinical practice. The searches were not limited to particular types of study design so as to include all human clinical studies (i.e. randomized controlled trials). The following keywords were used: CBCT, volumetric computed tomography, impacted teeth. To determine whether the keywords covered all articles on the diagnostic accuracy of CBCT for maxillary impacted canines, the following journals were manually screened: The American Journal of Orthodontics and Dentofacial Orthopedics; The Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology and Endodontology; The European Journal of Orthodontics. Finally, all relevant abstracts were read, and the full texts of all relevant articles were collected and reviewed. Ambiguous articles were also read to avoid inappropriate exclusion. All procedures were performed independently by two authors (GR, CC), and controversies were solved by reading again the articles and discussing them until consensus was reached.
Results
A total of 94 abstracts were found using the search methods described. Seven abstracts were judged to meet the inclusion criteria and were read in full (4,10–16). Two of the collected studies were excluded for methodological limits: the first one (11) compared different radiographic exams for the localization of impacted maxillary canines of four different subjects; the other one (13) compared the efficacy of CBCT images in diagnosis of maxillary impacted canines with traditional radiographs (panoramic and maxillary occlusal) not generated using traditional systems but obtained from CBCT data. Finally, only five papers met the inclusion criteria and resulted relevant for the review (Fig. 1).
Figure 1.
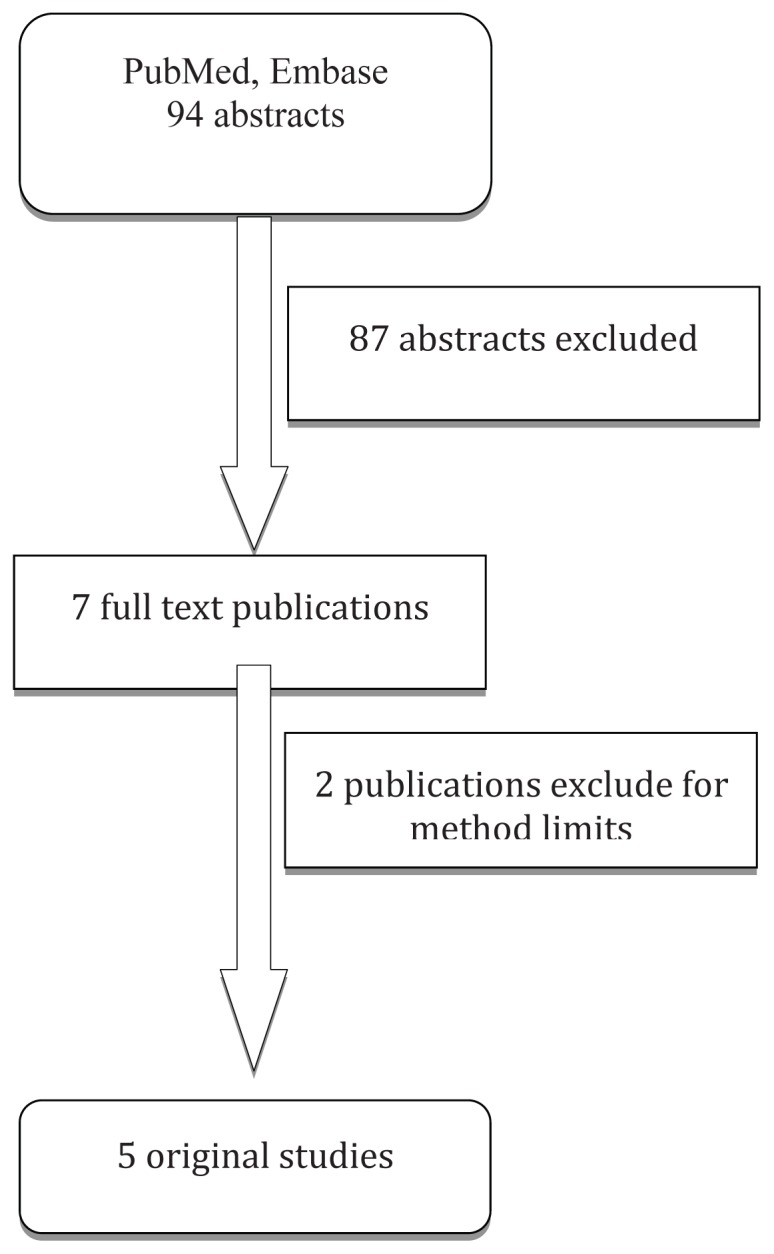
Flowchart of the selection strategy used in the review.
Three studies (4,12,16) used CBCT imaging as the standard method with the purpose to localize maxillary impacted canines in 3D and assess root resorption of adjacent teeth. Two of these studies (4,16) described the exact position of impacted maxillary canines and their spatial relationship with neighboring anatomical structures using CBCT images. Only the third publication (12) compared the differences between the variations of impaction with a control group (30 normally erupted canines). While Oberoi et al.(16) described the localization of the maxillary impacted canines in 3D (“mesial”, “distal”, “facial”, “palatal” and “gingival” impactions) and assessed root resorption of lateral incisors (“no root resorption”, “slight”, “moderate”, “severe” root resorption), Walker et al. (4) and Liu et al. (12) focused their attention also to the type of impaction, the proximity of the impacted canine to the lateral and central incisors, the follicle size, the existence of deciduous canines and the alveolar width in the canine area. No diagnostic accuracy was described in these three studies and the study sample was different among the mentioned articles.
The other two publications (14,15) performed a comparative analysis between traditional radiographs and CBCT images in the diagnosis of maxillary impacted canines. Haney et al. (14) evaluated also the diagnostic accuracy of CBCT in detecting impacted maxillary canines. These Authors used as 2D traditional radiographic methods the panoramic radiographs to evaluate the vertical position and the occlusal x-rays to evaluate the proximity to adjacent teeth; two periapical radiographs were used to determine the labio-palatal position. The clinicians’ confidence of the accuracy of diagnosis and treatment plan was statistically higher for CBCT images (P <0.001). No root resorption of adjacent teeth was assessed. Alqerban et al.(15) compared traditional panoramic radiograph with two different CBCT systems: 3D Accuitomo-XYZ Slice View Tomograph® (J. Morita, Kyoto, Japan) and Scanora® 3D CBCT (Soredex, Tuusula, Finland).
The Authors describe the diagnostic accuracy for the localization of maxillary impacted canines and the detection of root resorption of maxillary incisors of these three different radiographic systems. They found that a greater agreement between observers for all variables was achieved when using CBCT. No statistically significant differences among the different CBCT devices were found.
A summary of the results from the 5 articles is presented in Tables 1 and 2.
Table 1.
Search results. CBCT localization of maxillary impacted canines and incisors root resorption.
| Authors | Sample size | CBCT machine | Records collected | Results |
|---|---|---|---|---|
| Walker et al. 2005 | 19 patients: 16 bilateral impacted canines, 5 left unilateral impacted canines, 6 right unilateral impacted canines | NewTom QR-DVT 9000, Verona, Italy |
|
92.6% palatal impactions. Resorption: 66.7% lateral incisors, 11.1% central incisors. Impacted canine side vs erupted canine side: the alveolus was narrower. No common location where eruption was arrested. Great variation in the inclination of the impacted canine. |
| Liu et al. 2008 | 175 patients: 210 impacted canines | NewTom QR-DVT 9000, Verona, Italy |
|
Impaction: 45.2% buccallabially, 40.5% palatally, 14.3% in the midalveolus. Locations: 67 mesial-labial, 74 mesialpalatal, 31 in situ, 12 distal, 18 horizontal, 8 inverted. Root resorption: 27.2% of lateral incisors, 23.4% of central incisors, 94.3% of these occurred where the impacted canines were in close contact with the incisors. |
| Oberoi et al. 2012 | 29 patients: 26 bilateral impacted canines, 16 unilateral impacted canines | Hitachi MercuRay CBCT (Hitachi Medical Corporation, Tokyo, Japan) |
|
Average degree of impaction: mesial 10.1mm, distal 4.2mm, facial 4.16mm, palatal 1.8mm, gingival 10mm. Root resorption of lateral incisors: 40.4% no, 35.7% slight, 14.2% moderate, 4% severe. |
Table 2.
Search results. Conventional radiographs vs CBCT in diagnosis of maxillary impacted canines and incisors root resorption.
| Authors | Sample size | CBCT machine | Records collected | Results |
|---|---|---|---|---|
| Haney et al. 2010 | 18 patients: 25 impacted canines | Hitachi MercuRay CBCT (Hitachi Medical Corporation, Tokyo, Japan) |
|
21% disagreement in the perceived mesiodistal cusp tip position. 16% difference in the perceived labiopalatal position. Perception of root resorption of adjacent teeth: 36% lack of congruence. The clinicians’ confidence of the accuracy of diagnosis and treatment plan: statistically higher for CBCT images (P<0.001). |
| Alqerban et al. 2011 | 60 patients: 89 impacted or ectopically erupting maxillary canines |
|
|
Highly significant difference between the 2D and 3D images in all variables calculated. |
Discussion
The advantages of 3D medical computed tomography (CT) imaging are already well established in different dental specialties: management of trauma to the maxillofacial skeleton, surgical facial reconstruction, orthognathic surgery, dental implants, complicated extractions and endodontic treatments (17–20). Nevertheless, its use has been limited in orthodontics due to high-radiation dose, high cost, lack of availability, poor resolution and difficulty in interpretation. These issues may be addressed by recent CBCT innovations in CT technology and the use of CBCT systems could substantially modify the management of patients with potentially complex orthodontic problems.
The aim of this review was to analyze the literature focused on the CBCT accuracy in giving information about the localization of impacted maxillary canines, and to evaluate the advantages of CBCT images compared with those of conventional radiographs. Only few studies matched the inclusion criteria of this review, differing for the sample size and the methods used. Walker et al. (4), Oberoi et al. (16) and Liu et al.(12) evaluated, using CBCT data, the localization of impacted maxillary canines and assessed lateral root resorption lesions. Walker et al.(4) collected 19 patients, ranged from 8 to 20 years (average, 13.3; SD, 2.98), with a total of 27 impacted maxillary canines. The Authors focused their attention on the type of impaction, the resorption of incisors, the proximity of the impacted canine to the lateral and central incisors, the follicle size, the existence of deciduous canines, the alveolar width in the area of the canine, and the location of the impacted canines (coronal or frontal, sagittal, axial or horizontal). The study sample of Liu et al.(12) comprised 175 patients with 210 impacted maxillary canines. The age range was not specified. The Authors evaluated the 3D variations of impaction (vertical inclination, mesio-distal migration, bucco-lingual crown location), linear and angular measurements of the inclination and location of the impacted canines related to maxillary anatomical structures made on axial and transaxial views, based upon the methods used by Walker et al. (4). The Authors also evaluated follicle size, contact of impacted canine to the incisors and resorption of the incisors (assessed by axial and transaxial views and graded in 4 categories based on the grading system suggested by Ericson and Kurol (21): no resorption: intact root surface; mild resorption: resorption midway to the pulp or more, the pulp lining being unbroken; moderate resorption: the pulp is exposed by the resorption, the involved length of the root is less than one third of the entire root; severe resorption: the pulp is exposed by the resorption, and the involved length is more than one third of the root). Oberoi et al.(16) analyzed 29 CBCT of orthodontic patients with a total of 42 impacted maxillary canines. Age range was 10.6 to 28.0 years with a mean age of 16.6 years. The objective of this study was to localize the impacted canines in 3D and determine the most common location of impaction. The Authors also assessed lateral root resorption, but they did not focuse their attention on the follicle size, the existence of deciduous canines and the alveolar width in the area of the canine.
All the papers selected agreed on the following conclusions: 3D volumetric imaging of impacted maxillary canines can determine with extreme precision the presence and absence of the canine, the size of the follicle, the inclination of the long axis of the teeth, the relative buccal and palatal positions, the amount of bone covering the teeth, the anatomical bone structures, the 3D proximity and resorption of roots of adjacent teeth, the condition of adjacent teeth, the local anatomic considerations, and finally the overall stage of dental development. Therefore, all Authors agreed on the reliably assessment of the 3D position and on the improved localization and surgical-orthodontic management of maxillary impacted canines using CBCT technique.
Considering studies that compared traditional radiographic analysis and CBCT images (14–15), CBCT was found more sensitive than conventional radiography for maxillary impacted canines localization and identification of root resorption in adjacent teeth. Haney et al.(14) concluded that the orthodontic treatment plans were significantly influenced by the radiographic modality (P <0.0001). Alqerban et al. found greater agreement between observers for all the variables studied when using CBCT. In addition, this two Authors confirmed the literature data (21–23): panoramic radiography is not a reliable method for localization of impacted canines, and conventional radiographic imaging is inadequate for the detection of root resorption and the characterization of resorptive lesions.
Based on the results of this review, the following conclusions can be made:
the studies on 3D localization of impacted maxillary canines and assessment of lateral root resorption showed that CBCT system is a reliable method for detecting canine impaction;
the studies on comparison between traditional radiographs and CBCT, demonstrated that CBCT is superior to other radiographic methods for visualizing the maxillofacial region and it is a useful aid for the diagnosis and visualization of the position and complications of impacted maxillary canines;
methodological differences among selected studies (i.e. study sample, materials and methods) revealed the lack of studies performed using methodological standards for diagnostic accuracy and effectiveness of CBCT in the diagnosis of maxillary impacted teeth.
References
- 1.Mason C, Papadakou P, Roberts GJ. The radiographic localization of impacted maxillary canines: a comparison of methods. Eur J Orthod. 2001;23:25–34. doi: 10.1093/ejo/23.1.25. [DOI] [PubMed] [Google Scholar]
- 2.Preda L, La Fianza A, Di Maggio EM, Dore R, Schifino MR, Campani R, et al. The use of spiral computed tomography in the localization of impacted maxillary canines. Dentomaxillofacial Radiol. 1997;26:236–41. doi: 10.1038/sj.dmfr.4600258. [DOI] [PubMed] [Google Scholar]
- 3.Stewart JA, Heo G, Glover KE, Williamson PC, Lam EW, Major PW. Factors that relate to treatment duration for patients with palatally imapcted maxillary canines. Am J Orthod Dentofac Orthop. 2001;119:216–25. doi: 10.1067/mod.2001.110989. [DOI] [PubMed] [Google Scholar]
- 4.Walker L, Enciso R, Mah J. Three-dimansional localization of maxillary canines with cone-beam computed tomography. Am J Orthod Dentofac Orthop. 2005;128:418–23. doi: 10.1016/j.ajodo.2004.04.033. [DOI] [PubMed] [Google Scholar]
- 5.Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod. 1994;64:249–56. doi: 10.1043/0003-3219(1994)064<0249:WNID>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 6.Ericson S, Kurol J. CT diagnosis of ectopically erupting maxillary canines – a case repost. European Juornal fo Orthodontics. 1988;10:115–21. doi: 10.1093/ejo/10.2.115. [DOI] [PubMed] [Google Scholar]
- 7.Ericson S, Kurol J. Incisor root resorption due to ectopic maxillary canines imaged by computerized tomography: a comparative study in entracte teeth. Angle Orthodontist. 2000;70:276–83. doi: 10.1043/0003-3219(2000)070<0276:IRRDTE>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 8.Ericosn S, Bjerklin K, Falahat B. Does the canine dental follicle cause resorption of permanent root? A computed tomography study of erupting maxillary canines. Angle Orthodontist. 2002;72:95–104. doi: 10.1043/0003-3219(2002)072<0095:DTCDFC>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 9.Schmuth GP, Freisfeld M, Koster O, Schuller H. The application of computerized tomography (CT) in cases of impacted maxillary canines. European Journal of Orthodontics. 1992;14:296–301. doi: 10.1093/ejo/14.4.296. [DOI] [PubMed] [Google Scholar]
- 10.Liberati A, Altman DG, Tetzlaff J, Murlow C, Gøtzsche PC, et al. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 6(7):e1000100. doi: 10.1371/journal.pmed.1000100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Maverna R, Gracco A. Different diagnostic tools for the localization of impacted maxillary canines: clinical considerations. Prog Orthod. 2007;81:28–44. [PubMed] [Google Scholar]
- 12.Liu D, Zhang W, Zhang Z, Wu Y, Ma Y. Localization of impacted maxillary canines and observation of adjacent incisor resorption with cone-beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:91–8. doi: 10.1016/j.tripleo.2007.01.030. [DOI] [PubMed] [Google Scholar]
- 13.Katheria BC, Kau CH, Tate R, Chen JW, English J, Bouquot J. Effectiveness of Impacted and Supernumerary Tooth Diagnosis from Traditional Radiography Versus Cone Beam Computed Tomography. Pediatr Dent. 2009;32(4):304–9. [PubMed] [Google Scholar]
- 14.Haney E, Gansky SA, Lee JS, Johnson E, Maki K, Miller AJ, Huang JC. Comparative analysis of traditional radiographs and cone-beam computed tomography volumetric images in the diagnosis and treatment planning of maxillary imparte canines. Am J Orthod Dentofacial Orthop. 2010;137:590–7. doi: 10.1016/j.ajodo.2008.06.035. [DOI] [PubMed] [Google Scholar]
- 15.Alqerban A, Jacobs R, Fieuws S, Willems G. Comparison of two cone beam computed tomographic system versus panoramic imaging for localization of imparte maxillary canines and detection of root resorption. Eur J Orthod. 2011;33:93–102. doi: 10.1093/ejo/cjq034. [DOI] [PubMed] [Google Scholar]
- 16.Oberoi S, Knueppel S. Three-dimensional assessment of impacted canines and root resorption using cone beam computed tomography. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2012;xx:xxx. doi: 10.1016/j.tripleo.2011.03.035. [DOI] [PubMed] [Google Scholar]
- 17.Scarfe WC, Farman AG, Sukovic P. Clinical applications of cone-beam computed tomography in dental practice. Journal of the Canadian Dental Association. 2006;72:75–80. [PubMed] [Google Scholar]
- 18.Nair MK, Nair UP. Digital and advanced imaging in endodontics: a review. J Endod. 2007 Jan;33(1):1–6. doi: 10.1016/j.joen.2006.08.013. [DOI] [PubMed] [Google Scholar]
- 19.Patel S, Dawood A, Mannocci F, Wilson R, Pitt Ford T. Detection of periapical bone defects in human jaws using cone beam computed tomography and intraoral radiography. Int Endod J. 2009 Jun;42(6):507–15. doi: 10.1111/j.1365-2591.2008.01538.x. Epub 2009 Mar 2. [DOI] [PubMed] [Google Scholar]
- 20.Quereshy FA, Savell TA, Palomo JM. Applications of cone beam computed tomography in the practice of oral and maxillofacial surgery. J Oral Maxillofacial Surg. 2008;66:791–6. doi: 10.1016/j.joms.2007.11.018. [DOI] [PubMed] [Google Scholar]
- 21.Eriscon S, Kurol J. Resorption of incisors after ectopic eruption of maxillary canines: a CT study. Angle Orthod. 2000;70:415–23. doi: 10.1043/0003-3219(2000)070<0415:ROIAEE>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 22.Nagpal A, Pai KM, Setty S, Sharma G. Localization of impacted maxillary canines using panoramic radiography. Journal of Oral Science. 2009;51:37–45. doi: 10.2334/josnusd.51.37. [DOI] [PubMed] [Google Scholar]
- 23.Heimisdottir K, Bosshardt D, Ruf S. Can the severity of root resorption be accuratle judged by means of radiographs? A case report with histology. Am J Orthod Dentofacial Orthop. 2005;128:106–9. doi: 10.1016/j.ajodo.2004.11.028. [DOI] [PubMed] [Google Scholar]