

Abstract
Malignant tumors in the tonsils are usually primary. Metastases to the tonsils are extremely rare, with nearly one hundred cases reported. Herein we present an unusual case of palatine tonsillar metastasis of non-small cell lung cancer during chemotherapy. The patient was a 39-year-old man who was diagnosed as non-small lung cancer with IIIA4 staging and poor differentiated histology. After two cycles of vinorelbine and cisplatin based chemotherapy, a big mass was developed in the right palatine tonsil which was pathologically confirmed as the metastasis from the lung. There was no hemorrhage and complains except moderate foreign body sensations. No cervical lymphadenopathy and distal metastases to other organs such as brain and liver was found. Because of poor overall performance status, no radiotherapy was given. The disease progressed after docetaxel treatment. To the best of our knowledge, this is the first case with palatine tonsillar metastasis from non-small lung cancer during induction chemotherapy.
Keywords: Tonsil neoplasm, metastasis, lung neoplasm, computed tomography, histopathology
Introduction
Tonsil is a quite rare site of metastatic disease. Metastatic palatine tonsil tumor generally occurs from the tumors in kidney [1], skin [2] (melanoma), Lung [3] and occasionally colon [4], rectum [5], cecum [6], liver [7], stomach [8]. The prognosis of metastatic palatine tonsil cancer is poor and the mean time of survival following the development of tonsillar metastasis was nine months [3].
It is often difficult to distinguish a metastatic tumor at unusual sites from the secondary cancer. We present a case of a 39-year-old male patient with lung cancer who developed a big metastasis in the right palatine tonsil after two cycles of chemotherapy, highlighting the importance of systemic physical examination to evaluate chemotherapy effects.
Case report
A 39-year-old man was admitted to our hospital because of severe persistent dry cough for 7 moths. He did not have a history of fever, weight loss, headache or bloody phlegm. He did not complain any pharyngeal foreign body sensations. He had smoked 40 cigarettes a day for more than 20 years but was otherwise fit and well. There was no history of ear, nose and throat problems.
The physical examination did not reveal any enlargement of bilateral palatine tonsil or cervical lymphadenopathy. There were no positive findings in the physical examination except that breathing sounds especially on the right side were increased moderately.
The chest X-Ray showed opacity in the right lung and a subsequent CT scan revealed a mass of 4.2 × 4.8 cm (T2a) in the right upper lobe, and fixed multistation N2 disease. A lesion was further identified in the upper lobe of the right lung by bronchofibroscopy. A punch biopsy was taken and histological examination confirmed as poorly differentiated carcinoma (Figure 1A). Immunohistochemistry was positive for cytokeratin (CK), epithelial membrane antigen (EMA), but negative for chromogranin A (CgA), synaptophysin (Syn), neurone specific enolase (NSE), leukocyte common antigen (LCA) and neuronal cell adhesion molecules (CD56). Serum levels of squamous cell carcinoma (SCC) and NSE were all in normal range. No lesions in the bone, brain, liver and adrenal glands were found according to the results of CT-scan, ECT-scan or magnetic Resonance Imaging.
Figure 1.
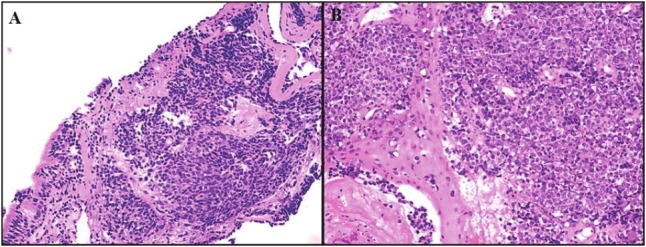
Microscopic findings of the tumor in the lung (HE, x100) (A), and palatine tonsil (HE, x100) (B). These lesions revealed poorly differentiated carcinoma.
Although the tumor cells were poorly differentiated, we planned a treatment strategy according to non-small cell lung cancer after the communication with two experienced pathologist. Because he had a relatively poor performance status of 2, sequential chemoradiotherapy was ordered. The patient received vinorelbine (25 mg/m2) on days 1, 8 plus cisplatin (80 mg/m2) on day 1 for every 21 days. After two cycles of chemotherapy, CT-scan evaluation of the abdomen and chest was done and the chemotherapy effect was evaluated initially as stable disease (according to RECIST Criteria). The patient coughed much less. He was planned to receive subsequent thoracic radiotherapy. However, a mass of 3.5cm from the right Palatine tonsil was found (Figure 2A and 2B). Also he felt with foreign body sensation in the oral cavity that he had never found. The biopsy confirmed it as the poorly differentiated metastatic carcinoma (Figure 1B).
Figure 2.
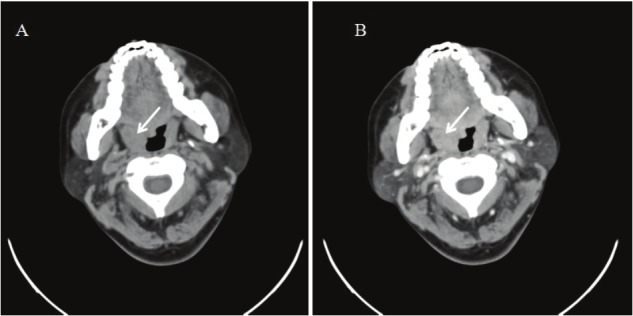
CT scan of the oropharynx showing a mass at the level of the right palatine tonsil (A) (arrow), and slightly enhanced tumor tissue after injection of a contrast medium (B) (arrow). There was no cervical lymph node swelling.
Immunohistochemical analysis showed positive staining for CK, EMA, and negative for CgA, Syn, NSE, LCA and CD56. So the effect of chemotherapy was revised from stable disease (SD) to progression disease (PD) and the second-line chemotherapy with single agent docetaxel was therefore offered. However, the mass in the tonsil was still not shrunk after 2 cycles of chemotherapy.
Discussion
Malignant tumors in the tonsils are usually primary and the incidence of tonsillar metastasis is very rare. In a series of 1535 malignant tonsillar neoplasms collected at the Armed Forces Institute of Pathology between 1945 and 1976, only 12 (0.8 per cent) were metastatic [9]. Joseph was probably the first to report the palatine tonsil metastasis of human cancers [10]. Since then, around 100 cases of metastatic tonsil cancers have been reported.
Palatine tonsils have only efferent lymphatics. The metastatic pathway to the tonsil from primary tumors remains controversial. The hematogenous route probably account for the majority of metastases to the palatine tonsil. Retrograde lymphatic spread of tumors to the tonsil has also been suggested although it seems less likely especially when the cervical lymph nodes are uninvolved. The possibility of direct implantation of cancer cells from instrumentation during bronchoscopy has been suggested in patients with lung cancer [3].
Liver, bone, adrenal glands and brain are the common sites for the metastases of lung cancer. Up to now, 19 cases of lung cancers mainly small cell carcinoma were found to have tonsillar metastases and 17 of them involved the palatine tonsils while only 2 cases metastasize to the lingual tonsil [11]. Although the tumor cells were poorly differentiated in the case reported here, CK and EMA but not CgA, Syn, NSE, LCA and CD56 were expressed, strongly indicating the nature of non-small cell lung cancer.
The prognoses of patients with tonsillar metastases are poor due to the lack of effective treatments. However, recent reports indicate that epidermal growth factor receptor (EGFR) inhibitors significantly improved prognosis of a lung cancer patient with tonsillar metastasis by achieving a mean progression-free survival (PFS) of 4.7 months with first- and second-line treatments, a PFS of 58.8 months with gefitinib and an overall survival (OS) of 82.4 months [12]. Unfortunately, the patient refused to receive EGFR inhibitor treatment due to the potential heavy economic burden. To the best of our knowledge, this patient is the first reported case of palatine tonsillar metastasis from non-small cell lung cancer after chemotherapy.
Acknowledgement
We are grateful to the hospital staff for their cooperation. This paper was supported by Medical Scientific Research Foundation of Zhejiang Province, China (Grant No.2007B025 and No.2010KYA036).
References
- 1.Brownson RJ, Jaques WE, LaMonte SE, Zollinger WK. Hypernephroma metastatic to the palatine tonsils. Ann Otol Rhinol Laryngol. 1979;88:235–240. doi: 10.1177/000348947908800215. [DOI] [PubMed] [Google Scholar]
- 2.Aydogan LB, Myers JN, Myers EN, Kirkwood J. Malignant melanoma metastatic to the tonsil. Laryngoscope. 1996;106:313–316. doi: 10.1097/00005537-199603000-00013. [DOI] [PubMed] [Google Scholar]
- 3.Seddon DJ. Tonsillar metastasis at presentation of small cell carcinoma of the lung. J R Soc Med. 1989;82:688. doi: 10.1177/014107688908201122. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sheng LM, Zhang LZ, Xu HM, Zhu Y. Ascending colon adenocarcinoma with tonsillar metastasis: a case report and review of the literature. World J Gastroenterol. 2008;14:7138–7140. doi: 10.3748/wjg.14.7138. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Goldenberg D, Golz A, Arie YB, Joachims HZ. Adenocarcinoma of the rectum with metastasis to the palatine tonsil. Otolaryngol Head Neck Surg. 1999;121:653–654. doi: 10.1016/S0194-5998(99)70076-8. [DOI] [PubMed] [Google Scholar]
- 6.Guvenc MG, Ada M, Acioglu E, Pamukcu M. Tonsillar metastasis of primary signet-ring cell carcinoma of the cecum. Auris Nasus Larynx. 2006;33:85–88. doi: 10.1016/j.anl.2005.07.009. [DOI] [PubMed] [Google Scholar]
- 7.Llanes F, Sanz-Ortega J, Suarez B, Sanz-Esponera J. Hepatocellular carcinomas diagnosed following metastasis to the oral cavity. Report of 2 cases. J Periodontol. 1996;67:717–719. doi: 10.1902/jop.1996.67.7.717. [DOI] [PubMed] [Google Scholar]
- 8.Benito I, Alvarez-Gago T, Morais D. Tonsillar metastasis from adenocarcinoma of the stomach. J Laryngol Otol. 1996;110:291–293. doi: 10.1017/s0022215100133468. [DOI] [PubMed] [Google Scholar]
- 9.Hyams VJ. Differential diagnosis of neoplasia of the palatine tonsil. Clin Otolaryngol Allied Sci. 1978;3:117–126. doi: 10.1111/j.1365-2273.1978.tb00674.x. [DOI] [PubMed] [Google Scholar]
- 10.Joseph G. Ein Fall von metastatischem Magencarcinom. Dtsch Med Wochenschr. 1907;33:460–461. [Google Scholar]
- 11.Mastronikolis NS, Tsiropoulos GE, Chorianopoulos D, Liava AC, Stathas T, Papadas TA. Palatine tonsillar metastasis from lung adenocarcinoma. Eur Rev Med Pharmacol Sci. 2007;11:279–282. [PubMed] [Google Scholar]
- 12.Gottschling S, Penzel R, Pelz T, Herpel E, Schnabel PA, Dyckhoff G, Thomas M, Kuhnt T. KRAS-mutation positive, metastatic tonsil carcinoma with cancer stem-like cell features and long-term response to gefitinib: a case report and review of the literature. J. Clin. Oncol. 2011;29:e616–619. doi: 10.1200/JCO.2011.34.5892. [DOI] [PubMed] [Google Scholar]