

Abstract
Introduction
In Ethiopia, lack of reliable data on causes of death prevents full understanding of the double mortality burden of communicable and noncommunicable diseases. Our objective was to help bridge this research gap by analyzing surveillance data on causes of death in Addis Ababa.
Methods
Burial surveillance identified 58,010 deaths in Addis Ababa from 2006 through 2009, of which 49,309 were eligible for verbal autopsies, a method of interviewing caregivers of the deceased about the circumstances, signs, and symptoms preceding death. We randomly selected 10% from the eligible sample, of whom 91% were defined as adults (aged ≥15 y). Verbal autopsies were completed and causes of death were assigned for 3,709 adults.
Results
Overall, 51% (95% confidence interval [CI], 49.7%-52.9%) of deaths were attributed to noncommunicable diseases, 42% (95% CI, 40.6%-43.8%) to communicable diseases, and 6% (95% CI, 5.5%-7.0%) to injuries. Similar proportions of male and female deaths were caused by noncommunicable and communicable diseases. Adults aged 55 to 84 were more likely, and those aged 15 to 44 were less likely, to die from noncommunicable diseases compared with the age group 85 or older. Premature deaths (defined as earlier than age 65) from noncommunicable diseases were mainly due to certain cancers, type 1 and type 2 diabetes, hypertension, stroke, and genitourinary disease.
Conclusion
Noncommunicable diseases are the leading cause of death among adults in Addis Ababa, where the health care system is still geared toward addressing communicable diseases. Health policy attention is needed to remedy this situation. This observed double mortality burden is unlikely to be unique to Addis Ababa and provides new insight into the epidemiological transition in urban Ethiopia. Nationwide studies should be conducted in Ethiopia to examine the pattern of epidemiological transition and the magnitude of double mortality burden.
Introduction
For 1,500 years, epidemics of communicable diseases such as plague, cholera, smallpox, typhus, and dysentery were documented as major causes of death in Ethiopia. In the early 20th century, one-fifth of the Addis Ababa population died of influenza (1). In the late 20th century, meningitis, malaria, cholera, and AIDS ravaged the country (2). Analogous data for noncommunicable diseases, however, are scarce (3). Thus, it is difficult to assess the double mortality burden, that is, the increasing threat of noncommunicable diseases as a cause of death while deaths from infectious diseases remain highly prevalent. The health system continues to rely heavily on the conventional infectious disease paradigm and is unresponsive to the emerging epidemiological shift.
Evidence on the causes and patterns of death is required to understand the overall epidemiological profile of diseases in Ethiopia and to help planners and decision makers prioritize the public health agenda. The objective of this study was to examine the proportion of deaths in Addis Ababa caused by communicable diseases, noncommunicable diseases, and injuries using verbal autopsy, a method of interviewing relatives or caregivers of the deceased about their signs, symptoms, lifestyle behaviors, and other characteristics before death and the circumstances surrounding their death.
Methods
We conducted verbal autopsies of a sample of deceased Addis Ababa residents for whom data were collected by the Addis Ababa Mortality Surveillance Program from September 2006 through December 2009. Our sampling frame was all burials recorded by burial surveillance, which has been conducted since 2001 in all cemeteries within the city limits. Cemetery clerks submitted forms for all deaths (approximately 20,000 per year). In principle, burial surveillance records data for all deceased residents of Addis Ababa, although biases exist because residents may die or be buried outside the capital, just as nonresidents may be buried inside city limits. Some of these biases are identified and corrected, but others inevitably go unnoticed (4-6). However, the 2007 Ethiopian census showed that Addis Ababa had 18,686 deaths of adults (defined for our study as aged ≥15) in the year before the census, a death rate of 9.2 per 1,000 (7). This is similar to the number identified by burial surveillance, 18,013, an age-specific death rate of 8.9 per 1,000. Similarly, adult deaths identified in 2008 and 2009 were 17,984 and 18,154, respectively.
The study population was all adults buried in Addis Ababa cemeteries. Addis Ababa has 89 cemeteries; 64 are Ethiopian Orthodox Church-based, 10 are municipal, 9 are mosque-based, and the rest are associated with the Catholic Church, Greek Orthodox Church, and synagogues. Because cremation is not practiced in Addis Ababa, virtually all deaths result in burials conducted at religious or municipal sites (8).
The burial surveillance identified 58,010 deaths during the study period. Of these, 49,309 (85%) deaths were eligible for verbal autopsy; the rest were not because they had been buried without close relatives or friends who could provide information for verbal autopsy interviews. The verbal autopsy questionnaire was adapted from a standardized verbal autopsy questionnaire from the World Health Organization (WHO) and International Network for the Demographic Evaluation of Populations and Their Health in Developing Countries Network. Three pairs of trained data collectors administered the surveys. They underwent frequent refresher training with strict supervision.
We randomly selected 10% (4,931) of deaths from the eligible burial surveillance sample for verbal autopsy; we used a sample for financial and logistical reasons. Of these, 91% (4,494) were aged 15 or older. We completed verbal autopsies for 3,709 (83%) deaths. All underwent physician review, and underlying causes of death were assigned. Verbal autopsy was not conducted for the rest, 785 (17%) of the sample because some caregivers were unwilling to participate and others were not available, despite repeated visits to their residences.
The age group 15 or older was selected for this study because the prevalence of noncommunicable diseases is rapidly increasing for this age category in developing countries and because the age group 15 to 64 is considered the most economically productive. In addition, adult death rates are an indicator for overall death rates (9). Furthermore, burial surveillance tends to underreport infant deaths (10,11).
We adapted the 2006 Global Burden of Diseases and Risk Factors to classify causes of death in our study as follows: Group I (communicable diseases, maternal conditions, and nutritional deficiencies), Group II (noncommunicable causes), and Group III (injuries) (12).
We calculated percentages and proportional death rates using Stata software (StataCorp LP, College Station, Texas). We used a binary logistic regression model to assess associations and significant differences; adjusted odds ratios and 95% confidence intervals were calculated to assess strength of associations.
Results
Of the 3,709 adults for whom verbal autopsies were completed, approximately half were women and 60% were aged 15 to 64 (Table 1). The median age at death was 55 (range, 15-105).
Table 1.
Sociodemographic Characteristics in a Sample of Deceased Adults (N = 3,709), Addis Ababa, Ethiopia, 2006-2009
| Characteristic | Women, n (%) | Men, n (%) |
|---|---|---|
| Age, y | ||
| 15-24 | 123 (3.3) | 94 (2.5) |
| 25-34 | 270 (7.3) | 261 (7.0) |
| 35-44 | 241 (6.5) | 286 (7.7) |
| 45-54 | 237 (6.4) | 250 (6.7) |
| 55-64 | 234 (6.3) | 229 (6.2) |
| 65-74 | 262 (7.1) | 337 (9.1) |
| 75-84 | 221 (6.0) | 248 (6.7) |
| ≥85 | 257 (6.9) | 159 (4.3) |
| Religion | ||
| Orthodox | 1,629 (43.9) | 1,629(43.5) |
| Muslim | 166 (4.5) | 170 (4.6) |
| Other | 50 (1.3) | 50 (1.3) |
| Ethnicity | ||
| Amhara | 1,001 (27.0) | 933 (25.2) |
| Oromo | 453 (12.2) | 456 (12.3) |
| Guraghe | 212 (5.7) | 248 (6.7) |
| Other | 179 (4.8) | 227 (6.1) |
| Education status | ||
| No education | 971 (26.2) | 484 (13.0) |
| Elementary school | 405 (10.9) | 486 (13.1) |
| Secondary school | 276 (7.4) | 465 (12.5) |
| College/university | 74 (2.0) | 222 (6.0) |
| Other (church education) | 119 (3.2) | 207 (5.6) |
| Occupation | ||
| Professional/technical/managerial/sales and services | 209 (5.6) | 663 (17.9) |
| Skilled/unskilled manual labor | 216 (5.8) | 319 (8.6) |
| Housewives | 1,090 (29.4) | 8 (0.2) |
| Retired | 79 (2.1) | 465 (12.5) |
| Other (unemployed, students, farmers) | 251 (6.8) | 409 (11.0) |
| Marital status | ||
| Single | 289 (7.8) | 515 (13.9) |
| Married | 446 (12.0) | 1,032 (27.8) |
| Separated | 133 (3.6) | 48 (1.3) |
| Divorced | 139 (3.7) | 58 (1.6) |
| Widowed | 838 (22.6) | 211 (5.7) |
Overall, 51% of deaths were attributed to noncommunicable diseases, 42% to communicable diseases (of which a negligible percentage were due to maternal and nutritional conditions), and 6% to injuries. The cause of death was ill-defined for 7% of deaths (Table 2). These percentages exceeded 100% because multiple causes could be recorded for 1 death. Proportions of male and female deaths due to noncommunicable and communicable diseases were similar, but more women than men died of both. In contrast, injuries were responsible for 10% of male and 3% of female deaths.
Table 2.
Causes of Death, by Sex, in a Sample of Deceased Adults (N = 3,709), Addis Ababa, Ethiopia, 2006-2009
| Cause of Death | na | % (95% CI)b | ||
|---|---|---|---|---|
|
| ||||
| Men | Women | Total | ||
| Communicable diseases, maternal conditions, and nutritional deficiencies | ||||
| All | 1,565 | 40 (37.8-42.2) | 44 (41.7-46.3) | 42 (40.6-43.8 ) |
| HIV/AIDS | 707 | 17 (15.3-18.7) | 21 (19.1-22.9) | 19 (17.8-20.3) |
| Tuberculosis | 460 | 14 (12.4-15.6) | 11 (9.6-12.3) | 12 (11.3-13.5) |
| Respiratory tract infections | 102 | 3 (2.2-3.8) | 3 (2.2-3.8) | 3 (2.2-3.3) |
| Diarrheal disease | 115 | 3 (2.2-3.8) | 4 (3.1-4.9) | 3 (2.5-3.7) |
| Meningitis | 47 | 1 (0.5-1.5) | 2 (1.4-2.6) | 1 (0.7-1.3) |
| Noncommunicable diseases | ||||
| All | 1,904 | 50 (47.7-52.3) | 53 (50.7-55.3) | 51 (49.7-52.9) |
| Malignant neoplasm | 386 | 8 (6.8-9.2) | 13 (11.5-14.5) | 10 (9.4-11.3) |
| Stomach cancer | 73 | 2 (1.4-2.6) | 2 (1.4-2.6) | 2 (1.6-2.5) |
| Breast cancer | 43 | 0 | 2 (1.4-2.6) | 1 (0.7-1.3) |
| Uterine cancer | 47 | 0 | 2 (1.4-2.6) | 1 (0.7-1.3) |
| Liver cancer | 37 | 1 (0.5-1.5) | 1 (0.6-1.6) | 1 (0.7-1.3) |
| Cancer of cervix | 19 | 0 | 1 (0.6-1.6) | 1 (0.7-1.3) |
| Colon and rectal cancer | 27 | 1 (0.5-1.5) | 1 (0.6-1.6) | 1 (0.7-1.3) |
| Other neoplasm | 145 | 4 (3.1-4.9) | 4 (3.1-4.9) | 4 (3.3-4.5) |
| Diabetesc | 183 | 6 (4.9-7.1) | 4 (3.1-4.9) | 5 (4.2-5.6) |
| Neuropsychiatric conditions | 76 | 2 (1.4-2.6) | 2 (1.4-2.6) | 2 (1.6-2.5) |
| Cardiovascular diseases | 885 | 24 (22.1-25.9) | 24 (22.1-26.0) | 24 (22.5-25.2) |
| Hypertension | 426 | 11 (9.4-12.4) | 12 (10.5-13.5) | 12 (10.5-12.5) |
| Stroke | 404 | 11 (9.4-12.4) | 11 (9.6-12.4) | 11 (9.9-11.9) |
| Congestive heart failure | 239 | 6 (4.9-7.1) | 7 (5.8-8.2) | 6 (5.7-7.2) |
| Myocardial infarction | 84 | 3 (2.2-3.8) | 1 (0.6-1.5) | 2 (1.6-2.5) |
| Respiratory diseases | 93 | 2 (1.4-2.6) | 3 (2.2-3.8) | 3 (2.5-3.7) |
| Asthma | 73 | 2 (1.4-2.6) | 2 (1.4-2.6) | 2 (1.6-2.5) |
| Digestive diseases | 327 | 10 (8.6-11.4) | 8 (6.8-9.2) | 9 (7.9-9.7) |
| Chronic liver disease | 165 | 5 (4.0-6.0) | 4 (3.1-4.9) | 4 (3.8-5.1) |
| Peptic ulcer disease | 31 | 1 (0.5-1.5) | 1 (0.6-1.5) | 1 (0.7-1.3) |
| Genitourinary disease | 137 | 4 (3.1-4.9) | 4 (3.1-4.9) | 4 (3.1-4.3) |
| Chronic renal failure | 112 | 3 (2.2-3.8) | 3 (2.2-3.8) | 3 (2.5-3.6) |
| Injuries | ||||
| All | 233 | 10 (8.6-11.4) | 3 (2.2-3.8) | 6 (5.5-7.0) |
| Unintentional | 102 | 4 (3.1-4.9) | 1 (0.6-1.5) | 3 (2.2-3.3) |
| Road traffic accidents | 83 | 3 (2.2-3.8) | 1 (0.6-1.5) | 2 (1.6-2.5) |
| Intentional | 79 | 3 (2.2-3.8) | 1 (0.6-1.5) | 2 (1.6-2.5) |
| Poisoning | 28 | 1 (0.5-1.5) | 0 | 1 (0.7-1.3) |
| Ill-defined causes | ||||
| All | 254 | 6 (4.9-7.1) | 8 (6.8-9.2) | 7 (6.0-7.7) |
Values exceeded total deaths because multiple causes could be recorded for 1 death.
Values above 1 were rounded to nearest whole number and values less than 1 were reported as 0.
Type 1 and type 2 combined.
The leading cause of death was cardiovascular disease (CVD) (24%); proportions for hypertension (12%) and stroke (11%) were similar and constituted most of the CVD deaths. The second and third most common causes of death were HIV/AIDS (19%) and tuberculosis (12%). Malignant neoplasm (10%) was the fourth leading cause of death; stomach cancer (2%) and other neoplasms (4%) were the most common neoplasms. Digestive tract diseases caused 9% of all deaths; chronic liver disease accounted for 4%. These 5 leading causes of death accounted for three-fourths of all deaths. The other main causes of death were injury (6%) and type 1 and type 2 diabetes (5%) (Table 2).
Stratification by sex
The proportions of deaths from cardiovascular causes were comparable by sex, although the pattern varied slightly for the 2 major causes (hypertension and stroke) (Table 2). HIV/AIDS was responsible for a higher proportion of deaths among women, and the tuberculosis was higher for men. Similarly, women more often died of malignant neoplasm than did men. In contrast, digestive tract diseases, injuries, and diabetes caused larger numbers of deaths among men than women. Overall, communicable and noncommunicable diseases caused more deaths among women, and injuries caused more deaths among men.
Stratification by age
HIV/AIDS and tuberculosis were the leading causes of death for the age group 15 to 54, and CVD and neoplasm were the leading causes of death for people aged 55 or older (Table 3). The third, fourth, and fifth leading causes of death in most age groups were noncommunicable diseases.
Table 3.
Causes of Death, by Age, in a Sample of Deceased Adults (N = 3,709), Addis Ababa, Ethiopia, 2006-2009
| Cause of Death | na | % (95% CI)b | |||
|---|---|---|---|---|---|
|
| |||||
| 15-34 y | 35-54 y | 55-74 y | ≥75 y | ||
| Communicable diseases, maternal conditions, and nutritional deficiencies | |||||
| All | 1,565 | 59 (55.5-62.5) | 53 (49.9-56.1) | 29 (26.3-31.7) | 33 (30.0-36.1) |
| HIV/AIDS | 707 | 41 (37.5-44.5) | 34 (31.1-36-9) | 6 (4.6-7.4) | 0 |
| Tuberculosis | 460 | 19 (16.2-21.8) | 18 (15.6-20.4) | 9 (7.3-10.7) | 4 (2.7-5.3) |
| Respiratory tract infections | 102 | 2 (1.0-3.0) | 2 (1.1-2.9) | 2 (1.2-2.8) | 5 (3.6-6.4) |
| Diarrheal disease | 115 | 2 (1.0-3.0) | 2 (1.1-2.9) | 3 (3.0-4.0) | 7 (5.3-8.9) |
| Meningitis | 47 | 3 (1.8-4.2) | 2 (1.1-2.9) | 0 | 1 (0.3-1.7) |
| Noncommunicable diseases | |||||
| All | 1,904 | 25 (21.9-28.1 | 42 (40.0-45) | 70 (67.2-72.8) | 63 (59.8-66.2) |
| Malignant neoplasm | 386 | 7 (5.2-8.8) | 11 (9.1-12.9) | 15 (12.9-17.2) | 7 (5.3-8.9) |
| Stomach cancer | 73 | 1 (0.3-1.7) | 1 (0.4-1.6) | 3 (3.0-4.0) | 2 (1.2-2.9) |
| Breast cancer | 43 | 0 | 2 (1.1-2.9) | 1 (0.4-1.6) | 0 |
| Uterine cancer | 47 | 1 (0.3-1.7) | 2 (1.1-2.9) | 2 (1.2-2.8) | 1 (0.3-1.7) |
| Liver cancer | 37 | 0 | 1 (0.4-1.6) | 2 (1.2-2.8) | 1 (0.3-1.7) |
| Cancer of cervix | 19 | 0 | 1 (0.4-1.6) | 1 (0.4-1.6) | 0 |
| Colon and rectal cancer | 27 | 1 (0.3-1.7) | 0 | 1 (0.4-1.6) | 1 (0.3-1.7) |
| Other neoplasm | 145 | 3 (1.8-4.2) | 3 (2.0-4.1) | 6 (4.6-7.4) | 3 (1.9-4.1) |
| Diabetesc | 183 | 1 (0.3-1.7) | 4 (2.3-5.2) | 8 (6.4-9.6) | 6 (4.4-7.6) |
| Neuropsychiatric conditions | 76 | 3 (1.8-4.2) | 2 (1.1-2.9) | 2 (1.2-2.8) | 2 (1.2-2.9) |
| Cardiovascular diseases | 885 | 6 (4.3-7.7) | 15 (12.8-17.2) | 35 (32.1-37.9) | 37 (33.8-40.2) |
| Hypertension | 426 | 1 (0.3-1.7) | 6 (4.5-7.5) | 20 (17.6-22.4) | 16 (13.6-18.4) |
| Stroke | 404 | 1 (0.3-1.7) | 7 (5.4-8.6) | 16 (13.8-18.2) | 18 (15.5-20.5) |
| Congestive heart failure | 239 | 3 (1.8-4.2) | 4 (2.3-5.2) | 8 (6.4-9.6) | 10 (8.0-12.0) |
| Myocardial infarction | 84 | 0 | 2 (1.1-2.9) | 3 (3.0-4.0) | 3 (1.9-4.1) |
| Respiratory diseases | 93 | 1 (0.3-1.7) | 2 (1.1-2.9) | 4 (2.8-5.2) | 3 (1.9-4.1) |
| Asthma | 73 | 1 (0.3-1.7) | 2 (1.1-2.9) | 3 (3.0-4.0) | 2 (1.2-2.9) |
| Digestive diseases | 327 | 5 (3.4-6.6) | 9 (7.2-10.8) | 11 (9.1-12.9) | 9 (7.1-10.9) |
| Chronic liver disease | 165 | 2 (1.0-3.0) | 5 (3.7-6.3) | 7 (5.5-8.5) | 3 (1.9-4.1) |
| Peptic ulcer diseases | 31 | 1 (0.3-1.7) | 1 (0.4-1.6) | 1 (0.4-1.6) | 1 (0.3-1.7) |
| Genitourinary diseases | 137 | 2 (1.0-3.0) | 3 (2.0-4.1) | 5 (3.7-6.3) | 4 (2.7-5.3) |
| Chronic renal failure | 112 | 2 (1.0-3.0) | 3 (2.0-4.1) | 4 (2.8-5.2) | 3 (1.9-4.1) |
| Injuries | |||||
| All | 233 | 15 (12.4-17.6) | 7 (5.4-8.6) | 4 (2.8-5.2) | 2 (1.2-2.9) |
| Unintentional | 102 | 6 (4.3-7.7) | 3 (2.0-4.1) | 2 (1.2-2.8) | 1 (0.3-1.7) |
| Road traffic accidents | 83 | 4 (2.6-5.4) | 3 (2.0-4.1) | 2 (1.2-2.8) | 0 |
| Intentional | 79 | 7 (5.2-8.8) | 2 (1.1-2.9) | 1 (0.4-1.6) | 0 |
| Poisoning | 28 | 1 (0.3-1.7) | 1 (0.4-1.6) | 1 (0.4-1.6) | 0 |
| Ill-defined causes | |||||
| All | 254 | 6 (4.3-7.7) | 5 (3.7-6.3) | 6 (4.6-7.4) | 11 (8.9-13.1) |
Values exceeded total deaths because multiple causes could be recorded for 1 death.
Values above 1 were rounded to nearest whole number, and values less than 1 were reported as 0.
Type 1 and type 2 combined.
The proportion of deaths caused by communicable diseases increased with age among people aged 15 to 34 and decreased after that until age 74. In contrast, the proportion of deaths caused by noncommunicable diseases was lower among people aged 15 to 44 but increased gradually until age 74. Proportions of deaths from injuries were higher among people aged 15 to 34 and decreased gradually after that. In general, deaths from noncommunicable diseases increased with age, and injuries decreased with age (Figure).
Figure.
Causes of death in a sample of deceased adults (N = 3,455) in Addis Ababa, by age, 2006-2009. Causes of death may not total 100% because multiple causes could be recorded for 1 death. The cause of death was ill-defined for 254 adults.
| Cause of Death | Age, y | |||||||
|---|---|---|---|---|---|---|---|---|
|
| ||||||||
| 15-24 | 25-34 | 35-44 | 45-54 | 55-64 | 65-74 | 75-84 | ≥85 | |
| Noncommunicable diseases, % | 30 | 22 | 33 | 52 | 68 | 72 | 71 | 54 |
| Communicable diseases, % | 45 | 65 | 60 | 44 | 34 | 25 | 31 | 35 |
| Injuries, % | 19 | 13 | 7 | 7 | 3 | 4 | 2 | 2 |
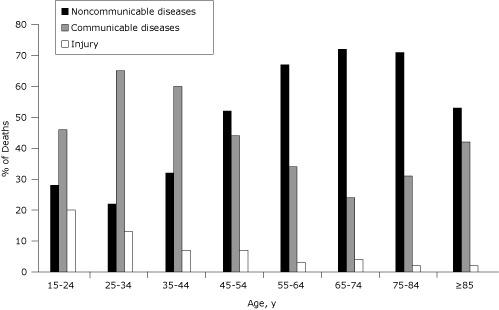
People aged 55 to 84 were more likely, and people who were aged 15 to 44 were less likely, to die from noncommunicable diseases compared with people aged 85 or older (Table 4).
Table 4.
Odds of Causes of Death in a Sample of Deceased Adults (N = 3,455a), Addis Ababa, Ethiopia, 2006-2009
| Category | n (%) | Crude OR (95% CI) | P Valueb | Adjusted OR (95% CI)c | P Valueb |
|---|---|---|---|---|---|
| Communicable diseases, maternal conditions, and nutritional deficiencies | |||||
| Age, y | |||||
| 15-34 | 442 (12) | 2.70 (2.11-3.46) | <.001 | 3.63 (2.70-4.88) | <.001 |
| 35-44 | 318 (9) | 2.84 (2.18-3.71) | <.001 | 3.59 (2.66-4.84) | <.001 |
| 45-54 | 214 (6) | 1.47 (1.12-1.92) | .006 | 1.73 (1.30-2.32) | <.001 |
| 55-64 | 156 (4) | 0.95 (0.72-1.23) | .72 | 1.06 (0.80-1.42) | .68 |
| 65-74 | 147 (4) | 0.61 (0.46-0.80) | <.001 | 0.68 (0.51-0.90) | .006 |
| 75-84 | 144 (4) | 0.83 (0.63-1.10) | .19 | 0.90 (0.67-1.19) | .44 |
| ≥85 | 145 (4) | 1 [Reference] | NA | 1 [Reference] | NA |
| Noncommunicable diseases | |||||
| Age, y | |||||
| 15-34 | 183 (5) | 0.28 (0.22-0.36) | <.001 | 0.20 (0.15-0.27) | <.001 |
| 35-44 | 176 (5) | 0.43 (0.33-0.57) | <.001 | 0.35 (0.26-0.47) | <.001 |
| 45-54 | 253 (7) | 0.94 (0.72-1.22) | .62 | 0.81 (0.61-1.07) | .14 |
| 55-64 | 313 (8) | 1.81 (1.37-2.38) | <.001 | 1.66 (1.25-2.21) | <.001 |
| 65-74 | 433 (12) | 2.26 (1.74-2.94) | <.001 | 2.11 (1.61-2.77) | <.001 |
| 75-84 | 334 (9) | 2.14 (1.62-2.83) | <.001 | 2.07 (1.56-2.74) | <.001 |
| ≥85 | 223 (6) | 1 [Reference] | NA | 1 [Reference] | NA |
Abbreviations: OR, odds ratio; CI, confidence interval; NA, not applicable.
Ill-defined causes of death (n = 254) were not analyzed.
Calculated by using χ2 test.
Adjusted for sex, religion, marital status, ethnicity, educational status, and occupation.
Discussion
Most of the deaths in this study were among the young and middle age groups (aged 30-64), reflecting a typical mortality burden for low- and middle-income countries (12). Noncommunicable diseases were the leading cause of death by a considerable margin. Few mortality studies are available for Africa, but this finding is in line with the 2001 estimate for low- and middle-income countries by the Global Burden of Diseases analysis, in which 36% of the deaths were due to Group I, 54% to Group II, and 10% to Group III (12). This finding also supports World Bank estimates for Madagascar in 2006, where the percentage of deaths among adults aged 15 to 44 due to Group I and Group II diseases was equivalent (40%) but for adults aged 45 or older was 18% and 63%, respectively (13). Our findings also support those of a study from Banjul, Gambia, where noncommunicable diseases were reported as the leading causes of death among adults (14). These similarities may be due to similar lifestyle and sociodemographic characteristics of urban settings in Africa.
On the other hand, our finding is different from a 2004 WHO estimate for deaths of African adults aged 15 to 59, in which 62% of the deaths were due to Group I diseases, 25% to Group II, and 13% to Group III (15). The World Bank estimate for Kenya in 2006 is also different; 75% of deaths among people aged 15 to 44 were due to Group I, and 11% were due to Group II; 57% of deaths among people aged 45 or older were from Group I, and 27% were from Group II (13).
Moreover, our findings are different from the estimates by the 2002 WHO analysis for Ethiopia (16). In that analysis, noncommunicable diseases accounted for 23% of deaths, and the corresponding estimate for communicable, maternal, perinatal, and nutritional causes was 71%. The possible explanation for these differences could be that cause-of-death analysis by WHO used cause-of-death models because of lack of information on death rates at the country level (17,18). Our results are not directly comparable to a study conducted in rural Ethiopia (19), where leading causes of death are Group I. Our study is from an urban setting dominated by a sedentary, Western lifestyle (eg, cigarette smoking, obesity, stress, and consumption of refined foods).
In our analysis, cardiovascular diseases, HIV/AIDS, tuberculosis, malignant neoplasm, and digestive tract diseases were the leading causes of death and accounted for three-fourths of all adult deaths. This finding supports the indication that an epidemiological transition is occurring, especially in the urban population, while people are also hard hit by HIV/AIDS and tuberculosis (20). An earlier community-based study in Addis Ababa also showed that high blood pressure and physical inactivity were highly prevalent among adults (21). In addition, a study from Zimbabwe, an urban blood pressure follow-up survey, and data from a central registry confirmed high prevalence of hypertension (22).
Our finding that men were more affected by injury concurs with that of a cause-of-death analysis of sub-Saharan Africa (13). Even though our study found that both men and women were almost equally affected by CVD, HIV/AIDS and malignant neoplasm caused more deaths among women than men. Another study found that more women than men die of HIV/AIDS in Addis Ababa (23). The higher proportion of deaths from malignancies among women requires further epidemiological study.
Among young and middle-aged adults, HIV/AIDS, tuberculosis, and injuries were leading causes of death in our study, while CVD, malignancies, and digestive tract diseases were the leading causes among adults aged 45 or older. In general, the proportion of deaths from communicable diseases and injuries decreased with age, while that from noncommunicable diseases increased. This implies that the premature death rate from communicable diseases is higher than that from noncommunicable diseases, a finding that is in line with those of the World Bank's estimates for causes of death in sub-Saharan Africa that reported young adults (aged 15-44) had a high prevalence of HIV/AIDS and high incidence of injuries (13). The pattern of cause of death by age is also in line with the study from South Africa that reported that deaths from communicable diseases decreased with increasing age (24). The contribution of noncommunicable diseases to premature death increases with age starting at age 35. These premature deaths from noncommunicable diseases were mainly due to selected cancers, diabetes, hypertension and stroke.
This study had several limitations. Burial surveillance may not record data for all deceased residents of Addis Ababa, some of whom died outside the city. Verbal autopsies may be less accurate than physical autopsies, and causes of death were ill-defined in some cases.
In conclusion, this study closes some gaps in the estimates of causes of death for Addis Ababa residents that may be relevant to health policy. Noncommunicable diseases are the leading cause of death among adults in Addis Ababa. Together with the existing burden of communicable diseases, this double morality burden requires the attention of policy makers and planners. Leading causes of deaths such as CVD, HIV/AIDS, tuberculosis, malignancies, digestive tract diseases, injuries, and diabetes should be prioritized for attention.
Finally, the observed pattern of double mortality burden is unlikely to be unique to Addis Ababa and provides new insight into the progression of the epidemiological transition in urban Ethiopia. This study may therefore serve as a baseline for further assessments. Similar studies or surveys should be conducted with large cities and rural areas to examine the pattern of epidemiological transition and the factors associated with it.
Acknowledgments
The Addis Ababa Mortality Surveillance Program was made possible with financial support from the AIDS Foundation of Amsterdam (grant no. 7022), the World Health Organization (WHO/Second Generation Surveillance on HIV/AIDS, contract no. SANTE/2004/089-735), the Centers for Disease Control and Prevention (EPHA-CDC Cooperative Agreement no. 5U22/PS022179_05), a Mellon Foundation pilot project grant to the Population Studies Center of the University of Pennsylvania, and a Hewlett Foundation grant to the University of Colorado at Boulder for the African Population Studies Research and Training Program. The program receives institutional support from the Faculty of Medicine of Addis Ababa University and the Ethiopian Public Health Association. Religious leaders and the Addis Ababa Labour and Social Affairs Bureau facilitated our access to the burial sites.
Footnotes
The opinions expressed by authors contributing to this journal do not necessarily reflect the opinions of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions.
Suggested citation for this article: Misganaw A, Mariam DH, Araya T. The double mortality burden among adults in Addis Ababa, Ethiopia, 2006-2009. Prev Chronic Dis 2012;9:110142. DOI: http://dx.doi.org/10.5888/pcd9.110142.
Contributor Information
Awoke Misganaw, Addis Ababa Mortality Surveillance Program, College of Health Sciences, Addis Ababa University; Addis Ababa, Ethiopia, Phone: 251911867007, Email: asterawoke2007@gmail.com.
Damen Haile Mariam, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia.
Tekebash Araya, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia.
References
- 1.Pankhurst R. An introduction to the medical history of Ethiopia. Trento (IT): Red Sea Press; 1990. [Google Scholar]
- 2.Tedla T. Meningococcal meningitis. In: Kloos H, Zein ZA, editors. The ecology of health and disease in Ethiopia. Boulder (CO): Westview Press, Inc; 1993. pp. 284–294. [Google Scholar]
- 3.Berhane Y, Haile Mariam D, Kloos H, editors. Epidemiology and ecology of health and disease in Ethiopia. Addis Ababa (ET): Shama Books; 2006. pp. 704–747. [Google Scholar]
- 4.Araya T, Reniers G, Schaap A, Kebede D, Kumie A, Nagelkerke N, et al. Lay diagnosis of causes of death for monitoring AIDS mortality in Addis Ababa, Ethiopia. Trop Med Int Health. 2004;9(1):178–186. doi: 10.1046/j.1365-3156.2003.01172.x. [DOI] [PubMed] [Google Scholar]
- 5.International statistics classification of diseases and related health problems (10th revision) Geneva (CH): World Health Organization; 1989. [Google Scholar]
- 6.Tensou B, Araya T, Telake DS, Byass P, Berhane Y, Kebebew T, et al. Evaluating the InterVA model for determining AIDS mortality from verbal autopsies in the adult population of Addis Ababa. Trop Med Int Health. 2010;15(5):547–553. doi: 10.1111/j.1365-3156.2010.02484.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.The population and housing census of Ethiopia. Statistical report for Addis Ababa City Administration. Addis Ababa (ET): Population Census Commission; 2007. pp. 175–193. [Google Scholar]
- 8.Sanders EJ, Araya T, Kebede D, Schaap AJ, Nagelkerke ND, Coutinho RA. Mortality impact of AIDS in Addis Ababa, Ethiopia. AIDS. 2003;17(8):1209–1216. doi: 10.1097/00002030-200305230-00013. [DOI] [PubMed] [Google Scholar]
- 9.Definition of indicators, world health statistics. Geneva (CH): World Health Organization; [Accessed January 25, 2012]. 2007. http://www.who.int/whosis/indicators/compendium/2007/en/index.html . [Google Scholar]
- 10.Measurement of overall and cause-specific mortality in infants and children: memorandum from a WHO/UNICEF meeting. Bull World Health Organ. 1994;72(5):707–713. [PMC free article] [PubMed] [Google Scholar]
- 11.Health and health related indicators. Addis Ababa (ET): Federal Democratic Republic of Ethiopia, Ministry of Health; 2000. [Google Scholar]
- 12.Lopez AD, Mathers CD, Ezzati M, Murray CJL, Jamison DT. Global burden of disease and risk factors. New York (NY): Oxford University Press; 2006. [PubMed] [Google Scholar]
- 13.Rao C, Lopez AD, Hemed Y. Causes of death. In: Jamison DT, Feachem RG, Makgoba MW, Bos ER, Baingana FK, Hofman KJ, Rogo KO, editors. Disease and mortality in sub-Saharan Africa. 2nd edition. Washington (DC): World Bank; 2006. pp. 43–58. [PubMed] [Google Scholar]
- 14.Van der Sande MA, Inskip HM, Jaiteh KO, Maine NP, Walraven GE, Hall AJ. Changing causes of death in the West African town of Banjul, 1942-97. Bull World Health Organ. 2001;79(2):133–141. [PMC free article] [PubMed] [Google Scholar]
- 15.The global burden of disease: 2004 update. World Health Organization; 2008. [Accessed January10, 2011]. http://www.who.int/healthinfo/global_burden_disease/2004_report_update/en/index.html . [Google Scholar]
- 16.Brundtland GH. From the World Health Organization. Reducing risks to health, promoting healthy life. JAMA. 2002;288(16):1974. doi: 10.1001/jama.288.16.1974. [DOI] [PubMed] [Google Scholar]
- 17.Mathers CD, Lopez AD, Murray CJL. The burden of disease and mortality by condition: data, methods and results for 2001. In: Lopez AD, Mathers CD, Ezzati M, Murray CJL, Jamison DT, editors. Global burden of disease and risk factors. New York (NY): Oxford University Press; 2006. pp. 45–240. [PubMed] [Google Scholar]
- 18.Global burden of deaths and DALYs. World Health Organization; [Accessed January 10, 2010]. 2004. http://www.who.int/healthinfo/statistics/bodgbddeathdalyestimates.xls . [Google Scholar]
- 19.Abdulahi H, Mariam DH, Kebede D. Burden of disease analysis in rural Ethiopia. Ethiop Med J. 2001;39(4):271–281. [PubMed] [Google Scholar]
- 20.Caselli G, Mesle F, Vallin J. Epidemiological transition theory exceptions. Citeseer 2002;58(1):1–34. [Google Scholar]
- 21.Tesfaye F. Epidemiology of cardiovascular disease risk factors in Ethiopia: the rural-urban gradient [dissertation] Umeå (SE): Umeå University; 2008. [Google Scholar]
- 22.Mufunda J, Chatora R, Ndambakuwa Y, Nyarango P, Kosia A, Sparks HV. Prevalence of noncommunicable disease in Zimbabwe: results from analysis of data from the National Central Registry and Urban Survey. Ethn Dis. 2006;16(3):718–722. [PubMed] [Google Scholar]
- 23.Single point HIV prevalence estimation. Addis Ababa (ET): Ethiopia Ministry of Health; 2007. [Google Scholar]
- 24.Kahn K, Tollman SM, Garenne M, Gear JS. Who dies from what? Determining cause of death in South Africa's rural north-east. Trop Med Int Health. 1999;4(6):433–441. doi: 10.1046/j.1365-3156.1999.00415.x. [DOI] [PubMed] [Google Scholar]