

Abstract
Historically, invasive, large incisions were necessary to perform “open” abdominal surgical procedures. While effective, this method increased the possibility of multiple complications, including post-operative pain, wound infection, incisional hernia and prolonged hospitalization. Concerns over the rate of complications and morbidities led surgeons to develop laparoscopic surgical techniques, in which operations in the abdomen are performed through small incisions as opposed to larger, open incisions across the surgical site. There was a continuous effort to minimize the number of ports, and finally single incision laparoscopic surgery (SILS) came into practice. Sils without frills is a concept where multiple ports are made in a curved 2.5 cm incision in a triangle. The chopstick method is used to minimize instrument and telescope clash during the procedure. Standard laparoscopic instruments are introduced along with a 30 ° telescope. Instrument clashes are avoided by chop stick technique of crossing them at a proximal point so that ends are away from each other. Dissection takes place in forward backward movement after making lateral retraction by the other instrument. With experience the operative time is expected to become comparable with conventional laparoscopic cholecystectomy. But benefits regarding post operative pain in SILS has not been confirmed. It is felt that expertise and reduction of operative time may reduce post operative pain. No special telescopes, ports or hand instruments are needed for this procedure but may have a role in advanced laparoscopic procedures.
Keywords: Sils, Spa, Single, Incision, Laparoscopy
Historically, invasive, large incisions were necessary to perform “open” abdominal surgical procedures. While effective, this method increased the possibility of multiple complications, including post-operative pain, wound infection, incisional hernia and prolonged hospitalization. Concerns over the rate of complications and morbidities led surgeons to develop laparoscopic surgical techniques, in which operations in the abdomen are performed through small incisions as opposed to larger, open incisions across the surgical site.
Laparoscopic cholecystectomy has replaced open cholecystectomy as the gold standard surgical procedure for majority of patients of gall stone disease [1]. Conventional laparoscopic Cholecystectomy is being performed using 4 ports. There was a continuous effort to minimize the number of ports, and finally single incision laparoscopic surgery (SILS) came into practice [2].
Single incision laparoscopic surgery is a rapidly evolving method that is complementing traditional laparoscopy in selected fields and patients [2–4]. It has also been suggested as a bridge between traditional laparoscopy and natural orifice transluminal endoscopic surgery [5].
It was started by the gynaecologists with the procedure of tubal ligation done by a single incision through the umbilicus in 1969 by Wheeles and this led to SILS tubal ligation becoming the gold standard with a nearly scarless abdomen [6, 7]. Appendecectomy in 1992 was the first general surgical procedure by Pelosi and D’Alessio [2]. Navarra et al. [3] reported early experiences with SILS cholecystectomy in 1997 in a letter to the editor in BJS. Navarra reported 30 patients who had two 10 mm cannulas placed next to each other and the skin cut was joined at the time of delivery of the gall bladder. Piskun and Rajpal [4] reported a different approach in 1999.
Since then various reports have come with various names like Single Port Surgery (SPA), Embryonic Natural Orifice Transumbilical Endoscopic Surgery (E-Notes), Laparo-Endoscopic Single Site Surgery (LESS), Single-Port Access (SPA), Single-Access Surgery (SAS), Single Site Surgery (S3), Trans Umbilical Endoscopic Surgery (TUES), Natural Orifice Trans-Umbilical Surgery (NOTUS), Single-Access Video Endoscopic Surgery (SAVES), Single-incision, multiport laparoscopy (SIMPL), Single-incision laparoscopic surgery (SILS).
Not much interest was shown by surgeons around the world for SILS till the time natural orifice transluminal endoscopic surgery (NOTES) came up. This led to a renewed interest in SILS procedures. Many surgeons have reported their experience of SILS and almost all operations have been done by this technique if we go through the various reports. There are very few studies that have compared it with standard laparoscopic surgery and little evidence that anything extra has been achieved apart from the cosmetic result.
The hot question today is whether this procedure is going to add anything to the existing laparoscopic surgery. The answer to this question is important for the patient, surgeon and health care industry.
Single incision laparoscopic surgery utilizes three ports through the single skin incision at umbilicus [8]. It is being considered as no scar surgery, because the incision is placed within the umbilical scar that is not visible [9, 10]. SILS has also decreased postoperative pain in some studies [9]. Many special instruments [8] and ports [11–13] are available now for SILS. Technical modifications like puppeteering of the gall bladder with a suture have been done [14].
Surgeon’s interest and industry interest can become a vicious cycle. So quickly came various devices like flexible tip telescopes that could avoid clash between instrument and camera. Roticulating and forward bending hand instruments that could go around the structures and give a somewhat triangulation experience. Pre-bent instruments that are longer lasting. Finally a plethora of ports through which multiple trocars and cannulas could be inserted without air leaks and minimal clashes.
All the above meant an increase of cost of surgery, which in the Indian context meant a doubling of the total cost in procedures, like cholecystectomy, ovarian cystectomy and appendicectomy (three of the commonest laparoscopic procedures done in our country by the laparoscopic method).
Also the above fancy and expensive equipment that looked good in animations were found to be very clumsy in the operating scenario. For example rotating the forward bent roticulating instrument led to not a tip rotation but an arc movement of the forward 5 cm of the grasper taking it out of the field in a circular movement. Having 2 bent instruments created havoc.
The real challenge of SILS is to avoid conflict between the operative instruments and the camera, to maintain the pneumoperitoneum and reduce operative stress. As a result of the limited space with using only a single incision, it is difficult for both the surgeon and the assistant to work in the area [14].
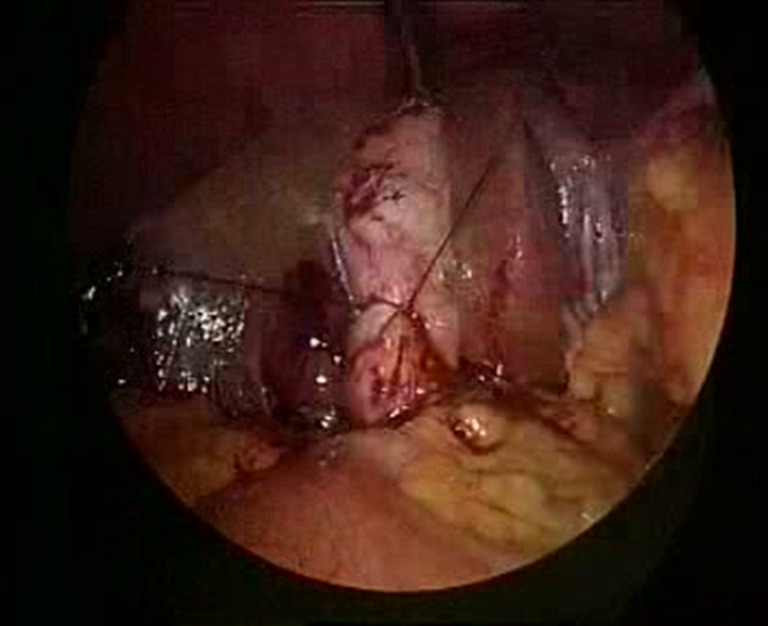
Sils without frills is a concept where multiple ports are made in a curved 2.5 cm incision in a triangle (Fig. 1). The chopstick method is used to minimize instrument and telescope clash during the procedure. Standard laparoscopic instruments are introduced along with a 30 ° telescope. Instrument clashes are avoided by chop stick technique of crossing them at a proximal point so that ends are away from each other (Fig. 2). Dissection takes place in forward backward movement after making lateral retraction by the other instrument (Fig. 3). For the SILS cholecystectomy, incision is made at the level of umbilicus. Upper skin flap is raised for a distance of 1 cm. After initial insufflation with Veress needle, a 10 mm cannula is inserted at the incision line and the two 5 mm cannulas half cm inferiorly and laterally on both sides through the same incision (Fig. 4). A grasper introduced through the right lateral cannula does the fundal traction. The left lateral cannula is used for introduction of the dissector to define Calot’s triangle (Fig. 5). The instrument cannulas and telescope cannula are crossed by a chop stick method (Fig. 2) to avoid sword fighting and clashing of instruments in the abdomen. At the end of the procedure, the gall bladder is delivered from the central port site. Fascial defects are closed meticulously and skin apposed.
Fig. 1.

Incision and port placement
Fig. 2.

Instrument crossing by ‘chop stick’ method
Fig. 3.

Instrument movements
Fig. 4.

Cannula positioning
Fig. 5.

Calot’s triangle in SILS Cholecystectomy
After struggling in the initial learning curve and also ‘converting’ a few cases to 4 port, many surgeons have adopted the technique for cholecystectomy. Method is quite successful for appendicectomy and ovarian cystectomy and hence covering the lower cost laparoscopic procedures and proving an alternative to the surgeons and patients without any increase in the cost of the procedure. Patients are delighted with the cosmetic results achieved (Fig. 6).
Fig. 6.

Cosmetic result
Difficult cases can be converted to ‘reduced’ port technique by adding innovating techniques like passing a suture to lasso (also called puppeteering technique) the Hartmann’s pouch of the gall bladder (Fig. 7). Also popular is a needle grasper that can be introduced through a ‘scarless’ needle puncture to hold the gall bladder fundus/appendicular tip/fallopian tube etc. (Fig. 8). Finally a ‘rescue’ port can be added in some case to make it a 2 port procedure. Last option of conversion to standard laparoscopic or open surgery is always there.
Fig. 7.
Lasso/Puppet technique
Fig. 8.
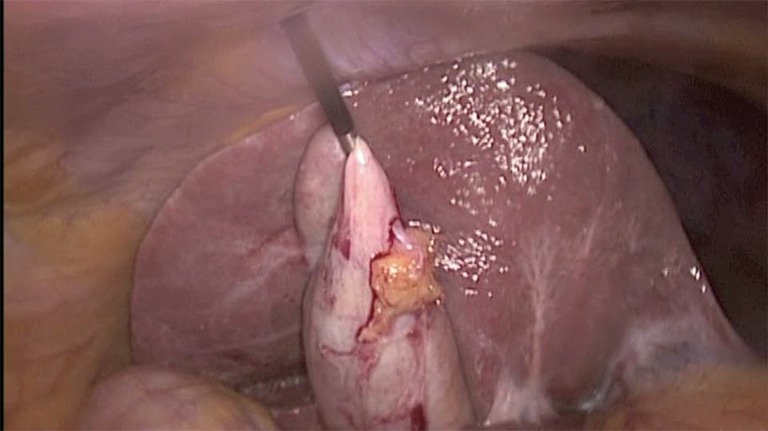
Needle grasper
So what is the Downside ?
The larger fascial incisions and excessive manipulation around small muscular space may lead to more pain and increased incidence of incisional hernias has also been an area of concern. It is tiring for the surgeon and will always take more time than if the procedure is done with multiple ports. Over enthusiasm may also potentially lead to a higher incidence of injuries.
A recent study presented at the Society of American Gastrointestinal and Endoscopic Surgeons found no difference in total operating room cost, charges to the patient, and hospital charges when comparing SILS cholecystectomy to standard cholecystectomy [15]. Further randomized studies are needed to determine if SILS is any better than conventional laparoscopic surgery.
The review of literature shows that there is a paucity of quality data comparing SILS to its counterpart. The studies we have do not reveal any significant advantage to SILS over standard laparoscopic techniques thus far, except with respect to cosmesis.
Conclusion
In recent years, SILS has been focused upon as a bridge between Natural orifice transluminal endoscopic surgery (NOTES) and traditional laparoscopic surgery [5]. NOTES is a technically challenging procedure and current instruments need to be further improved [16]. SILS, on the other hand, enables the application of a wide range of already existing instruments. The main point for reducing the number of incisions has not only been the cosmetic advantage but also lowered incision risks, morbidity of bleeding, incisional hernia, and organ damage [17, 18]. Single-incision laparoscopic surgery for gall bladder removal is a feasible and promising method for the treatment of symptomatic cholelithiasis [19, 20]. This surgery can be performed with traditional re-usable laparoscopic instruments [21]. With experience the operative time is expected to become comparable with conventional laparoscopic cholecystectomy. But benefits regarding post operative pain in SILS has not been confirmed [22]. There were some studies that indicate reduction in post operative pain [23] but those are small and not sufficient to come to a conclusion. It is felt that expertise and reduction of operative time may reduce post operative pain. No special telescopes, ports or hand instruments are needed for this procedure but may have a role in advanced laparoscopic procedures.
References
- 1.Johnson CD. ABC of the upper gastrointestinal tract upper abdominal pain: gall bladder. Br Med J. 2001;323:1170–1173. doi: 10.1136/bmj.323.7322.1170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Pelosi MA, Pelosi MA. Laparoscopic appendectomy using a single umbilical puncture (minilaparoscopy) J Reprod Med. 1992;37:588–594. [PubMed] [Google Scholar]
- 3.Navarra G, Pozza E, Occhionorelli S, Carcoforo P, Donini I. One-wound laparoscopic cholecystectomy. Br J Surg. 1997;84:695. doi: 10.1002/bjs.1800840536. [DOI] [PubMed] [Google Scholar]
- 4.Piskun G, Rajpal S. Transumbilical laparoscopic cholecystectomy utilizes no incisions outside the umbilicus. J Laparoendosc Adv Surg Tech. 1999;9:361–364. doi: 10.1089/lap.1999.9.361. [DOI] [PubMed] [Google Scholar]
- 5.Bresadola F, Pasqualucci A, Donini A, et al. Elective transumbilical compared with standard laparoscopic cholecystectomy. Eur J Surg. 1999;165(1):29–34. doi: 10.1080/110241599750007478. [DOI] [PubMed] [Google Scholar]
- 6.Wheeless CR. A rapid, inexpensive and effective method of surgical sterilization by laparoscopy. J Reprod Med. 1969;3(5):65–69. [Google Scholar]
- 7.Thompson B, Wheeless RC. Outpatient sterilization by laparoscopy. A report of 666 patients. Obstet Gynecol. 1971;38(6):912–915. [PubMed] [Google Scholar]
- 8.Tacchino R, Greco F, Matera D. Single-incision laparoscopic cholecystectomy: surgery without a visible scar. Surg Endosc. 2009;23:896–899. doi: 10.1007/s00464-008-0147-y. [DOI] [PubMed] [Google Scholar]
- 9.Cuesta MA, Berends F, Veenhof AA. The “invisible cholecystectomy”: a transumbilical laparoscopic operation without a scar. Surg Endosc. 2008;22:1211–1213. doi: 10.1007/s00464-007-9588-y. [DOI] [PubMed] [Google Scholar]
- 10.Hong TH, You YK, Lee KH. Transumbilical single-port laparoscopic cholecystectomy : scarless cholecystectomy. Surg Endosc. 2009;23:1393–1397. doi: 10.1007/s00464-008-0252-y. [DOI] [PubMed] [Google Scholar]
- 11.Kurpiewski W, Pesta W, Kowalczyk M, Głowacki L, Juśkiewicz W. SILS cholecystectomy—our first experiences. Videosurg Minim Invasive Tech. 2009;4(3):91–94. [Google Scholar]
- 12.Romanelli JR, Mark L, Omotosho PA. Single port laparoscopic cholecystectomy with the TriPort system: a case report. Surg Innov. 2008;15:223–228. doi: 10.1177/1553350608322700. [DOI] [PubMed] [Google Scholar]
- 13.Merchant AM, Cook MW, White BC, Davis SS, Sweeney JF, Lin E. Transumbilical Gelport access technique for performing single incision laparoscopic surgery (SILS) J Gastrointest Surg. 2009;13:159–162. doi: 10.1007/s11605-008-0737-y. [DOI] [PubMed] [Google Scholar]
- 14.Chow A, Purkayastha S, Aziz O, Paraskeva P. Single-incision laparoscopic surgery for cholecystectomy: an evolving technique. Surg Endosc. 2010;24:709–714. doi: 10.1007/s00464-009-0655-4. [DOI] [PubMed] [Google Scholar]
- 15.Love KM, Durham CA, Meara MP, Mays AC, Bower CE. Single-incision laparoscopic cholecystectomy: a cost comparison. Surg Endosc. 2011;25(5):1553–1558. doi: 10.1007/s00464-010-1433-z. [DOI] [PubMed] [Google Scholar]
- 16.Marescaux J, Dallemagne B, Perretta S, Wattiez A, Mutter D, Coumaros D. Surgery without scars: report of transluminal cholecystectomy in a human being. Arch Surg. 2007;142:823–826. doi: 10.1001/archsurg.142.9.823. [DOI] [PubMed] [Google Scholar]
- 17.Ishikawa N, Arano Y, Shimizu S, Morishita M, Kawaguchi M, Matsunoki A, Adachi I, Shimizu J, Watanabe G. Single incision laparoscopic surgery (SILS) using cross hand technique. Minim Invasive Ther Allied Technol. 2009;18:322–324. doi: 10.3109/13645700903384492. [DOI] [PubMed] [Google Scholar]
- 18.Kuon Lee S, You YK, Park JH, Kim HJ, Lee KK, Kim DG. Single-port transumbilical laparoscopic cholecystectomy: a preliminary study in 37 patients with gallbladder disease. J Laparoendosc Adv Surg Tech A. 2009;19:495–499. doi: 10.1089/lap.2008.0424. [DOI] [PubMed] [Google Scholar]
- 19.Ersin S, Firat O, Sozbilen M. Single-incision laparoscopic cholecystectomy: is it more than a challenge? Surg Endosc. 2010;24:68–71. doi: 10.1007/s00464-009-0543-y. [DOI] [PubMed] [Google Scholar]
- 20.Cugura JF, Janković J, Kulis T, Kirac I, Beslin MB. Single incision laparoscopic surgery (SILS) cholecystectomy: where are we? Acta Clin Croat. 2008;47:245–248. [PubMed] [Google Scholar]
- 21.Prasad A. Single incision laparoscopic surgery. World J Gastroenterol. 2010;16:2705–2706. doi: 10.3748/wjg.v16.i21.2705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Prasad A, Kaul S, Mukherjee K, Kaur M. Post operative pain after cholecystectomy: conventional laparoscopy versus single incision laparoscopic surgery. J Min Access Surg. 2011;7:24–27. doi: 10.4103/0972-9941.72370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Tsimoyiannis EC, Tsimogiannis KE, Pappas-Gogos G, et al. Different pain scores in single transumbilical incision laparoscopic cholecystectomy versus classic laparoscopic cholecystectomy: a randomized controlled trial. Surg Endosc. 2010;24(8):1842–1848. doi: 10.1007/s00464-010-0887-3. [DOI] [PubMed] [Google Scholar]