

Abstract
TThis paper reports two rare cases of patients with synchronous gastrointestinal stromal tumour (GIST) and colorectal adenocarcinoma (CRC) where adjuvant FOLFOX chemotherapy was administered concurrently with imatinib mesylate. The first case is a 67-year-old woman with a large gastrointestinal stromal tumour with metastasis masking a co-existing primary colon cancer, which was diagnosed after tumour response to imatinib mesylate. The second case presents a 61-year-old male with a primary colon cancer and a suspected metastatic lymph node, later confirmed to be a co-existing primary gastric GIST during colon surgery. While colorectal cancer is the third most common cause of cancer-related death in North America, the prevalence of GISTs remains rare. To date, very few cases of synchronous GIST and CRC adenocarcinoma have been reported in the literature. Although the coexistence of these two tumour types is rare, it is important to be aware of their disease patterns.
Keywords: Scolonic neoplasms, gastrointestinal stromal tumors, neoplasms, multiple primary
Case 1
In the fall of 2008, a previously well 67-year-old Caucasian woman, presented with progressive fatigue over three months accompanied by left lower abdominal pain. She reported passage of “darker stools”; however, there was no complaint of bright red blood per rectum or change in stool shape. On physical examination, a minimally tender palpable mass in the left lower quadrant was noted.
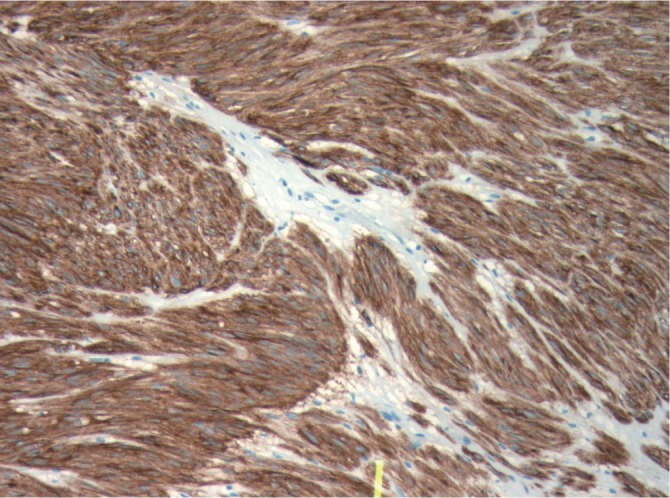
Computed tomography (CT) scan imaging revealed a large abdominal mass (Fig 1) with multiple hypervascular masses in the liver (Fig 2). The abdominal mass, with a large area of internal necrosis, was intimately related to the jejunum with minimal small bowel dilatation. One of the liver lesions in segment 4b was biopsied under ultrasound guidance. Pathology revealed a spindle cell tumour, which was strongly positive for CD117 and CD34 by immunohistochemistry (Fig 3). There were no mitotic figures noted. The pathologic diagnosis was consistent with metastatic gastrointestinal stromal tumour and in December 2008, she was started on 400 mg of imatinib mesylate per day.
Figure 1. CT of the abdomen revealing a large GIST.

Figure 2. CT scan revealing concomitant liver metastasis.

Figure 3. Strongly positive immunochemical CD117 immunostaining (x100) (Dako at a dilution of 1/400).
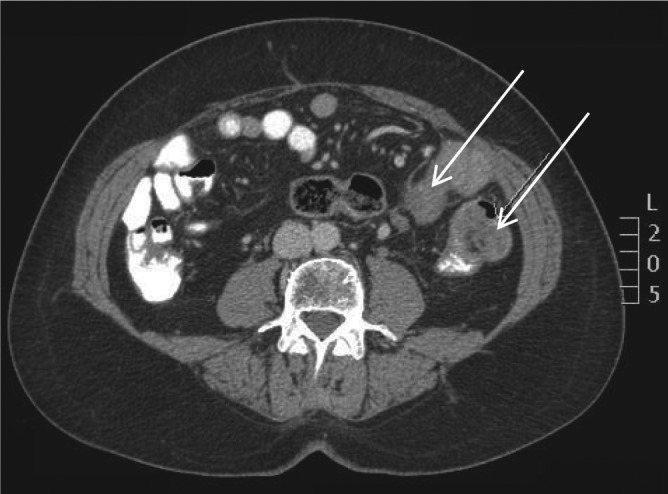
Subsequently, follow-up CT imaging revealed significant reduction of her primary GIST (Fig 4) as well as in the hepatic metastases. The GIST decreased from its initial size of 13.5 x 8.7 cm in November 2008 to 9.0 x 6.0 cm in January 2009. The primary tumour continued to decrease in size from 6.3 x 3.7 cm in June 2009 to 5.2 x 3.5 cm in November 2009.
Figure 4. CT scan of the abdomen following treatment with imatinib mesylate revealing a reduction of GIST (top arrow). The colon mass is now visible (bottom arrow).
The CT scan in November 2009 revealed the presence of a colonic mass with mesenteric lymphadenopathy. The presence of the newly identified mass was confirmed on colonoscopy, which revealed the presence of an intraluminal mass at 80 cm from the anal verge. Biopsy of this lesion revealed an invasive, moderately differentiated adenocarcinoma of colonic origin.
After discussion at tumor board, a decision was made to resect the primary colonic mass as well as the primary GIST. In December 2009, the patient underwent a left hemicolectomy in addition to resection of the primary GIST, which originated in the small bowel. The pathology of the colonic mass revealed a moderately differentiated adenocarcinoma with 7 out 12 lymph nodes involved. The small bowel pathology revealed a spindle cell lesion consistent with a GIST, which was positive for CD117 and CD34. The Ki67 stain showed positivity in less than 1% of tumour cells. The mitotic count was less than 1 per 50 High Power Fields (HPF). The tumour showed large hypocellular areas of hyalinization, an area of necrosis, and several areas of hemorrhage as well as a focal hemangiopericytoma-like pattern, consistent with treatment (imatinib mesylate) effect. Of note, the laboratory findings did not include a preoperative CEA, however, a CEA level was drawn shortly after the surgery, measuring 2.5 ug/L.
She subsequently received 12 cycles of modified FOLFOX-6 chemotherapy while remaining on imatinib for her metastatic GIST. She did not experience any unexpected toxicity from either the imatinib or chemotherapy and remains well with continued regression of her liver metastasis (GIST).
Case 2
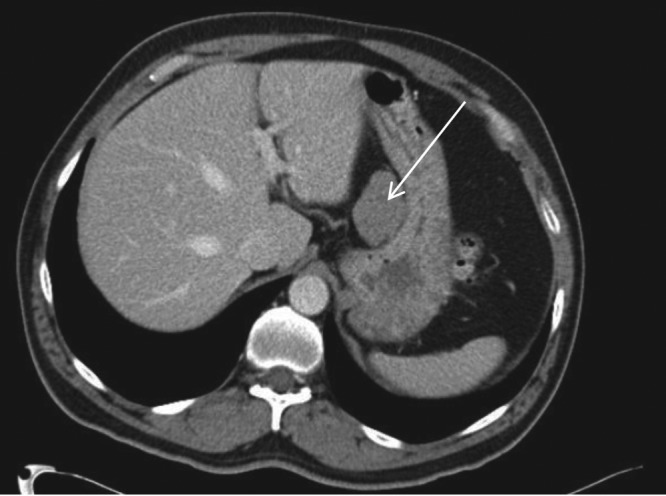
A 61-year-old Caucasian gentleman presented with a change in bowel habits and rectal bleeding in March 2009. He reported no associated anorexia or weight loss. Colonoscopy and biopsy revealed an adenocarcinoma at the splenic flexure. A staging CT scan also revealed a few subcentimeter lymph nodes and a 5 cm mass at the gastrohepatic ligament also suspected to be an enlarged metastatic lymph node (Fig 5).
Figure 5. CT scan demonstrating a mass later confirmed to be a primary gastric GIST.
In May 2009, at the time of surgery, the gastrohepatic mass was resected. Once confirmed on a frozen section to be a spindle cell tumour consistent with a GIST, a partial gastrectomy was performed.
During the same operation, the patient also underwent a left hemicolectomy. Final pathology revealed a 4 x 3.5 x 1.1 cm moderately differentiated adenocarcinoma with 4/22 lymph nodes being positive.
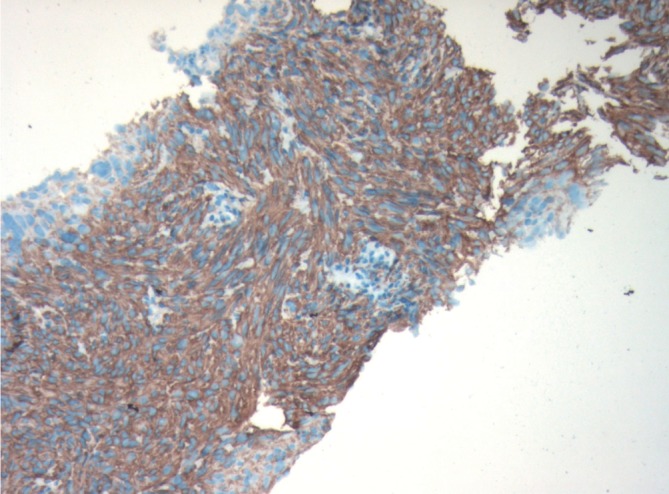
The gastric-based mass was a primary GIST measuring 5.5 cm. Histopathological examination revealed a spindle cell lesion with a high mitotic index of 7 mitoses per 50 high power fields (HPF) with negative resection margins. The immunohistochemistry was positive for CD34 and CD117 (Fig 6) and negative for S100 and desmin. Ki67 stained 10% of tumor cell nuclei. A pre-operative CEA level was normal at 1.3 ug/L.
Figure 6. Patient 2: Positive CD117 staining (x100) (Dako at a dilution of 1/400).
Post-operatively, he received 10 cycles of adjuvant FOLFOX chemotherapy for his stage III colon cancer as well as one year of adjuvant imatinib therapy for the GIST. Imatinib (400 mg per day) was started after he had received two cycles of modified FOLFOX-6.
Discussion
Defined as cellular spindle cell, epithelioid, or pleomorphic mesenchymal tumour of the gastrointestinal (GI) tract, the term gastrointestinal stromal tumour (GIST) was introduced by Mazur and Clark in 1983 to differentiate GISTs from leiomyomas (1),(2). The putative origin of these tumours is believed to be the interstitial cells of Cajal, the GI pacemaker cells (2)-(4). Approximately 95% of GISTs are positive for expression of the KIT (CD117, stem cell factor receptor) protein and as well as 70-80% of GISTs expressing CD34, the human progenitor cell antigen (2),(5).
Although GISTs are the most common mesenchymal tumours of the digestive tract, they remain rare. They represent 0.1-3% of all GI cancers and have an incidence of 10-20 cases/million (2),(4). Conversely, colorectal cancer is the third most common cause of cancer-related death in North America (6). While the incidence of synchronous occurrence of other tumours with GISTs is on the rise, there is no evidence of a common etiology (4),(7). Based on the prevalence of both tumours, an incidental occurrence is more likely. What remains important, however, is the need to be aware of their coexistence.
The first case outlines the presentation of a metastatic small bowel GIST masking a colonic adenocarcinoma. As the primary GIST decreased in size in response to treatment with imatinib mesylate, the colonic mass and enlarged mesenteric lymph node was unmasked. As lymph node involvement with GIST is rare, the lymphadenopathy was consistent with metastasis from a second primary tumour. It also highlights that metastatic GIST should not preclude the potential curative treatment of other secondary cancers. The second case details a man with a primary colonic neoplasm and an unidentified gastrohepatic mass that was initially suspected to be a metastatic node but later confirmed to be a GIST. Given the atypical location of the suspected lymph node, the patient underwent primary surgery rather than systemic therapy. These cases highlight the importance of being aware of second primary cancers throughout the course of treatment for both colon cancer and GISTs.
GISTs are most commonly found in the stomach and small intestine. The coexistence of GISTs and adenocarcinoma at two separate locations in the GI tract is uncommon (7). Both colon cancer and GISTs are infrequently associated with a genetic disposition and in this report, neither patient reported a family history of any malignancies.
Surgery is the primary treatment modality for both nonmetastatic GISTs and colon cancer (3). For metastatic GIST, imatinib mesylate is the standard first-line treatment (8). Imatinib mesylate, a selective tyrosine kinase inhibitor, has been shown to have a tumor response rate of greater than 50% (3),(9). Continuous treatment with imatinib in the metastatic setting is the standard treatment as interruptions have been shown to result in rapid disease progression (10). Although surgery for patients with metastatic disease is considered investigational, if the patient has disease responsive to imatinib, surgical excision of a primary tumor or an isolated metastasis that has progressed can be associated with a good outcome (11).
Treatment with imatinib in the adjuvant setting, however, is now established as the standard of care for those with resected primary GISTs (8). A phase III trial, ACOSOG Z9001, was the first to demonstrate that one year of imatinib as compared to placebo in the adjuvant setting, is effective in decreasing recurrences. The trial included 713 patients with a resected GIST measuring at least 3 cm in maximal diameter. Mitotic count was not an inclusion criterion for this study. In this report, patient two had a tumour greater than 3 cm and received adjuvant imatinib therapy for one year consistent with the recommendations of the major cancer societies (12),(13). Although adjuvant imatinib is recommended for a minimum of one year, the optimal duration of administration remains unknown. The Intergroup EORTC 62024 trial is a randomized study comparing two years of imatinib versus observation alone. The Scandinavian Sarcoma Group (SSG) trial XVIII is investigating three years versus one year of adjuvant imatinib. Although both studies have completed accrual, the results have not yet been presented. Hence, until the results of these two studies are known, the recommended duration of adjuvant treatment remains one year.
A unique feature common to the two cases presented is the concurrent treatment of adjuvant FOLFOX chemotherapy with imatinib mesylate. Dexamethasone is a steroid that is commonly included as part of the antiemetic regimen with a serotonin 5HT-3 antagonist in the FOLFOX regimen. Both imatinib and dexamethasone are metabolized by the cytochrome P450 (CYP450) isoenzyme CYP3A4. Imatinib is a potent competitive inhibitor of the CYP450 isoenzyme CYP3A4 while dexamethasone is an inducer (14). There is a high possibility of a drug interaction as the plasma concentration of imatinib may decrease when administered with dexamethasone. While case two presents a patient who received concurrent treatment for ten cycles of FOLFOX, the patient in case one was administered concurrent treatment for all twelve cycles. Although there were no ill effects noted in either case, perhaps due to the brief exposure of both dexamethasone and imatinib, a more prolonged exposure of the two medications may benefit from possible monitoring of plasma imatinib levels especially in the setting of metastatic GIST (case one). Modifications to the treatment could include increasing the dosage of imatinib, decreasing the dosage of dexamethasone, or administering another anti-emetic in lieu of dexamethasone.
Conclusion
There have been very few incidences of synchronous colorectal cancer and GISTs reported in literature. Most of the cases described were found due to other malignancies or discovered incidentally during surgery (3),(5),(15). The two cases presented above underline the importance of being aware of this particular coexistence as well as the unlikely metastatic spread of GIST to lymph nodes, development of other primary tumours during treatment of metastatic GIST, and the importance of a multidisciplinary approach to cancer treatment.
Footnotes
No potential conflict of interest.
References
- 1.Mazur MT, Clark HB. Gastric stromal tumors. Reappraisal of histogenesis. Am J Surg Pathol. 1983;7:507–19. doi: 10.1097/00000478-198309000-00001. [DOI] [PubMed] [Google Scholar]
- 2.Miettinen M, Lasota J. Gastrointestinal stromal tumors--definition, clinical, histological, immunohistochemical, and molecular genetic features and differential diagnosis. Virchows Arch. 2001;438:1–12. doi: 10.1007/s004280000338. [DOI] [PubMed] [Google Scholar]
- 3.Melis M, Choi EA, Anders R, Christiansen P, Fichera A. Synchronous colorectal adenocarcinoma and gastrointestinal stromal tumor (GIST) Int J Colorectal Dis. 2007;22:109–14. doi: 10.1007/s00384-006-0089-6. [DOI] [PubMed] [Google Scholar]
- 4.Efstathios P, Athanasios P, Papaconstantinou I, Alexandros P, Frangisca S, Sotirios G, et al. Coexistence of gastrointestinal stromal tumor (GIST) and colorectal adenocarcinoma: A case report. World J Surg Oncol. 2007;5:96. doi: 10.1186/1477-7819-5-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Kosmidis C, Efthimiadis C, Levva S, Anthimidis G, Baka S, Grigoriou M, et al. Synchronous colorectal adenocarcinoma and gastrointestinal stromal tumor in meckel's diverticulum; an unusual association. World J Surg Oncol. 2009;7:33. doi: 10.1186/1477-7819-7-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010;60:277–300. doi: 10.3322/caac.20073. [DOI] [PubMed] [Google Scholar]
- 7.Gopal SV, Langcake ME, Johnston E, Salisbury EL. Synchronous association of small bowel stromal tumour with colonic adenocarcinoma. ANZ J Surg. 2008;78:827–8. doi: 10.1111/j.1445-2197.2008.04669.x. [DOI] [PubMed] [Google Scholar]
- 8.DeMatteo RP, Ballman KV, Antonescu CR, Maki RG, Pisters PW, Demetri GD, et al. Adjuvant imatinib mesylate after resection of localised, primary gastrointestinal stromal tumour: a randomised, double-blind, placebo-controlled trial. Lancet. 2009;373:1097–104. doi: 10.1016/S0140-6736(09)60500-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Spinelli GP, Miele E, Tomao F, Rossi L, Pasciuti G, Zullo A, et al. The synchronous occurrence of squamous cell carcinoma and gastrointestinal stromal tumor (GIST) at esophageal site. World J Surg Oncol. 2008;6:116. doi: 10.1186/1477-7819-6-116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Le Cesne A, Ray-Coquard I, Bin Bui N, Adenis A, Rios M, Duffaud F, et al. Time to onset of progression after imatinib interruption and outcome of patients with advanced GIST: Results of the BFR14 prospective french sarcoma group randomized phase III trial [abstract] J Clin Oncol. 2010;s28:10033. [Google Scholar]
- 11.Mussi C, Ronellenfitsch U, Jakob J, Tamborini E, Reichardt P, Casali PG, et al. Post-imatinib surgery in advanced/metastatic GIST: Is it worthwhile in all patients? Ann Oncol. 2010;21:403–8. doi: 10.1093/annonc/mdp310. [DOI] [PubMed] [Google Scholar]
- 12.Nccn.org [Internet] Washington: National Comprehensive Cancer Network. c2010 [cited 2010]. Available from: http://www.nccn.org/ [Google Scholar]
- 13.Casali PG, Jost L, Reichardt P, Schlemmer M, Blay JY, ESMO Guidelines Working Group Gastrointestinal stromal tumours: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009;20:s64–7. doi: 10.1093/annonc/mdp131. [DOI] [PubMed] [Google Scholar]
- 14.Scripture CD, Figg WD. Drug interactions in cancer therapy. Nat Rev Cancer. 2006;6:546–58. doi: 10.1038/nrc1887. [DOI] [PubMed] [Google Scholar]
- 15.Tzilves D, Moschos J, Paikos D, Tagarakis G, Pilpilidis I, Soufleris K, et al. Synchronous occurrence of a primary colon adenocarcinoma and a gastric stromal tumor. A case report. Minerva Gastroenterol Dietol. 2008;54:101–3. [PubMed] [Google Scholar]