

Abstract
Benign chest wall tumours are very uncommon and chest wall lipomas are rarely reported in literature. We report herein a case of a 68-year old man who developed a giant, symptomless mass of the chest wall. A chest computed tomography scan evidenced a solid neoplasm measuring 27 cm in its major axis. A radical excision was performed and the histology was consistent with lipoma. To our knowledge, this is the first case reporting a giant lipoma of the chest wall with a thirty-year history.
Keywords: Lipoma, Chest wall tumour, Liposarcoma
INTRODUCTION
Benign chest wall tumours (BCWT) are very uncommon and chest wall lipomas are rarely reported in literature. We herein report a case of a giant, symptomless lipoma of the chest wall developed over a period of thirty years.
CASE REPORT
A 68-year-old caucasian man developed, in over thirty years of progressive enlargement, a giant, symptomless mass of the chest wall [Fig. 1(A)]. His medical history included coronary artery disease treated by percutaneous transluminal coronary angioplasty in 2006. Laboratory data and tumoral biomarkers were within normal limits. A computed tomography (CT) scan of the chest evidenced a solid neoplasm measuring 27 cm in its major axis, apparently originating from the left serratus anterior muscle. The mass showed a homogeneous fat density with spotted areas of calcification. No direct signs of chest wall invasion were detected [Fig. 1(B) and (C)]. Based upon the radiological findings, the possible diagnoses were those of a lipoma or liposarcoma. Given the foreseeable resectability of the mass, no biopsy was undertaken and a radical excision was indicated and performed. Intraoperatively, the mass was confirmed not to be infiltrating the chest wall, nor was any regional involvement evident. At final pathology, the tumour measured approximately 26 × 16 × 21 cm and weighed 4,570 g [Fig. 2(A)]. The histology was consistent with lipoma (well-encapsulated adipose tissue with fat necrosis areas, fibrosis and calcification) [Fig. 2(B)]. The patient's postoperative course was good; he was discharged in the third postoperative day and, one year after surgery, as expected, there is no evidence of recurrence.
Figure 1:
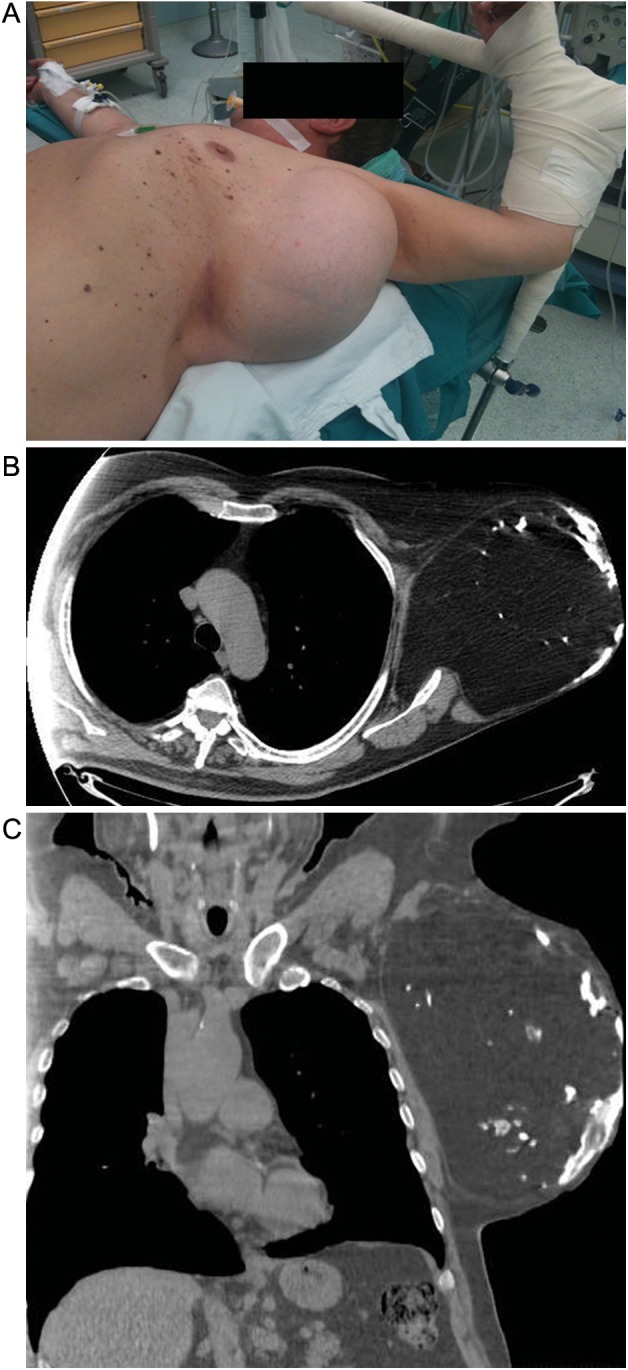
(A) Preoperative appearance of the chest wall mass. (B–C) Chest CT scan evidenced a solid neoplasm measuring 27 cm in its major axis, apparently originating from the left serratus anterior muscle. The mass showed a homogeneous fat density with spotted areas of calcification. No direct signs of chest wall invasion were detected.
Figure 2:
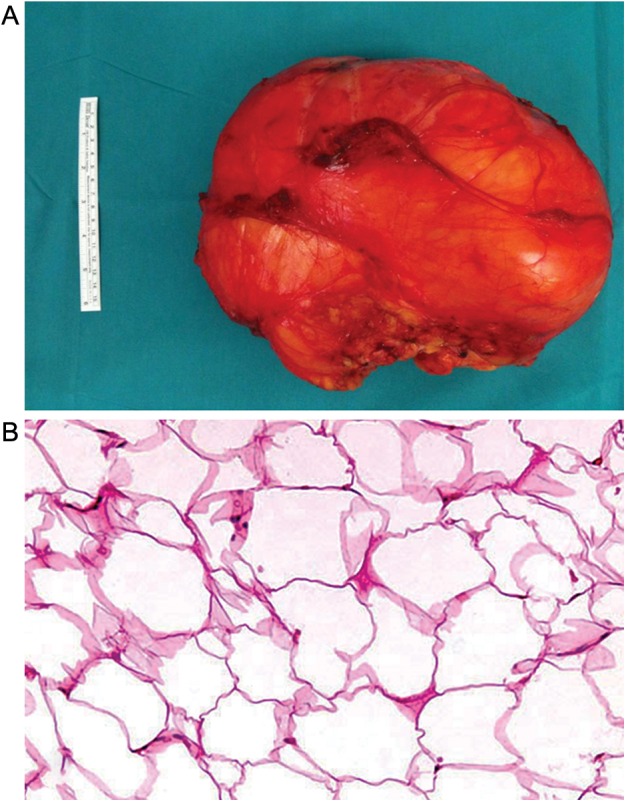
(A) Macroscopic aspect of giant lipoma. The tumour measured approximately 26 × 16 × 21 cm and weighed 4,570 g. (B) Final pathology confirmed a lipoma (well-encapsulated adipose tissue with fat necrosis areas, fibrosis and calcification).
DISCUSSION
BCWT may originate from vascular, peripheral nerve, osseous, cartilaginous, or adipose tissue and are very rare lesions. In the literature, few research studies of this group of tumours have been reported. In particular, the imaging features of BCWT are non-specific: only combination of imaging appearance, location and clinical information may suggest a diagnosis [1].
Chest radiography can be used to determine the location, size, and growth rate of the mass. However, CT enables a more accurate assessment of tumour morphology, composition, location and extent [1].
In the case we report, CT scan evidenced a solid neoplasm with homogeneous fat density with spotted areas of calcification. According to these radiological features and the absence of signs of chest wall invasion, we did not perform a fine needle aspiration biopsy preoperatively and a radical excision was indicated and performed.
Generally, chest wall lipomas occur in obese patients who are 50–70 years of age and, in most cases, are deep lesions, larger and less well circumscribed than subcutaneous ones [2]. In our case, the patient was 68 years old and the tumour (an extremely large mass measuring 27 cm in its major axis) apparently originated from the left serratus anterior muscle. Moreover, the capsule was difficult to see clearly on CT scans.
In conclusion, chest wall giant lipomas are rarely reported in the literature [3]. To our knowledge, this is the first case reporting a giant, symptomless lipoma of the chest wall developed over a thirty-year period.
Conflict of interest: none declared.
REFERENCES
- 1.Tateishi U, Gladish GW, Kusumoto M, Hasegawa T, Yokoyama R, Tsuchiya R, et al. Chest wall tumours: radiologic findings and pathologic correlation: part 1. Benign tumours. Radiographics. 2003;23:1477–90. doi: 10.1148/rg.236015526. [DOI] [PubMed] [Google Scholar]
- 2.Haas AF, Fromer ES, Bricca GM. Spindle cell lipoma of the scalp: a case report and review. Dermatol Surg. 1999;25:68–71. doi: 10.1046/j.1524-4725.1999.08038.x. [DOI] [PubMed] [Google Scholar]
- 3.Ozpolat B, Ozeren M, Akkaya T, Yucel E. Giant lipoma of chest wall. Eur J Cardiothorac Surg. 2004;26:437. doi: 10.1016/j.ejcts.2004.04.042. [DOI] [PubMed] [Google Scholar]