

Abstract
Objectives:
Mental disorders such as depression, anxiety and dementia are common in elderly. However, physical activity is suggested to be effective in preventing such aging-related disorders. The aim of this study was to investigate the role of physical activity on mental health in later life.
Methods:
Four hundred elderly people were randomly divided into the intervention and control groups. The intervention consisted of exercise twice a week for two months. Mental health status before, just after, and three months after the study was assessed with the 28-item General Health Questionnaire (GHQ-28).
Results:
The mean of the GHQ-28 total scale decreased in the case group and this change remained significant after three months (before: 8 ± 5.5, after three months: 5.6 ± 4.6, p < .001). GHQ subscales including somatization, anxiety, social dysfunction, and depression decreased significantly in the case group just after and three months after the intervention.
Conclusions:
Physical activity significantly prevents mental disorder in older adults. Although it has effects on anxiety, social dysfunction, and depression, the greatest influence is on improving the somatization symptoms.
Keywords: Aging, GHQ-28, mental health, physical activity
INTRODUCTION
Nowadays population aging is one of the most fundamental issues in the world. The elderly population has grown proportionally faster than other age group in many countries.[1,2] In Iran, although the elderly population (60 years and over) has small percentage of total population, it is rising rapidly compared to other age groups in recent decades.[3] As the population ages, a trend of health problems like chronic diseases and disabilities increases. About 84% of those aged 65 and older suffer from at least one chronic condition, compared to 38% of those aged 20 through 44.[4] The aging process is associated with an increased prevalence and number of both mental and physical health concerns and disabilities.[5] One of the consequences of chronic diseases is the dramatic increase in the old-age dependency ratio; therefore, these people cannot do their daily activities as they used to do. Some of them become dependent and incapable, which cause various problems such as mental disorders.[6] Mental health problems particularly depression and dementia are common in later life. For example, depression affects 3–5% of the over 65 s at any point in time, with milder forms of mood disorder being present in another 10–15%.[7] Studies on successful aging suggest that lifestyle habits like having physical activity has influence on physical and mental health in older people. Moreover the importance of physical activity in maintaining an independent living status in the elderly has been widely documented in several studies.[8,9] Doing regular exercises can increase the person's ability to perform daily chores without dependency. Additionally, these activities influence on different aspects of quality of life, such as reducing physical pain, general health, happiness, social and emotional function and mental health.[7] Despite this information, older adults remain mostly inactive and 65% of adults aged 75 and older report no leisure physical activity.[10,11] While a large number of studies have examined the effects of physical activity on mental health in adults, only a few interventions have been conducted in older people. In this study we investigated the effect of regular physical activities on mental health in the elderly in an Iranian setting.
METHODS
Subjects
Four hundred men and women aged 60 and over were recruited in this field trial study. The study was conducted in Shahrekord, which is a city in southwest of Iran. Participants were selected randomly from the list of population of 10 urban health centers, which were randomly selected from 35 centers. Then, subjects in the selected centers were stratified into two groups, intervention and control. Exclusion criteria were subjects with history of cardiovascular or respiratory diseases or any medical conditions that prevented them to exercise (before or during the study) and absentee in more than three consecutive sessions were excluded. All participants signed the informed consent forms.
Randomization
Participants were randomly assigned to either the intervention or the control group. Randomization took place at an individual level at the time of the first measurement. We used balanced block randomization. Participants agreed to take part before randomization without being informed about which group they were allocated to. The researchers and the participants had knowledge of participants’ group assignment after the randomization.
Intervention
The participants in the intervention group were visited by a general practitioner to rule out exclusion criteria. Then they took part in 45-minute-sessions, two times a week for 8 consecutive weeks. In each session an exercise instructor delivered a low intensity exercise program, adapted from a guideline provided by Iranian Ministry of Health.[12] The program consisted of the following parts: warming up in 20% of the session time, the main part that contained exercises for the upper body, lower body and movements for the whole body and cooling down phase, which took 10% of the session time. The exercises could be performed in sitting, as well as standing position. At the beginning of the session, the exercise instructor explained all the process. Moreover all participants were given a pamphlet explaining details of each session which also could be used for exercising at home. After finishing the exercise, the instructor explained the advantages of physical activity in later life.
Control Condition
Participants in the control group also received all the pamphlets[13] about exercise programs during 16 sessions when an exercise instructor explained about those pamphlets and also benefits of physical activity for elderly people in a two-hour session.
Data Collection
Since the percentage of illiteracy in Iranian elderly is high (about 71.6%),[14] self-response questionnaire could not be an appropriate way to collect information. Therefore, we all participants were interviewed. All interviewers were trained by the researchers. They were also handed in interview guidelines. The interviews were conducted three times: Before the intervention, just after and 3 months after the study.
Measures
In this study to measure the mental health we used the GHQ, which was designed by Goldberg and colleagues.[15] This instrument is widely used in the general population to measure mental health and screening in primary care. The main version of the questionnaire contains 60 questions; shorter versions are derived from the main one, GHQ-12 and GHQ-28. 28-Items that include a total score and four 7-item scales Somatization, Anxiety, Social dysfunction and Depression. The participants evaluate changes in his/her behaviors, mood and feelings in the recent four weeks. It has 4-point response scale. According to the standard scoring method, recommended by Goldberg, scores for the first two types of answers are “0” (positive) and for the two others “1” (negative).[16] This questionnaire was translated into the official language of Iran (Persian), which is comprehensible to almost every Iranian, and its validity and reliability were approved in an independent study.[13] Reliability and validity of this questionnaire is also indicated for the Iranians elderly.[17] The best cutoff point for this questionnaire was 6: i.e., those scoring 6 and above were designated as possible cases of mental disorder. Sensitivity, specificity and overall misclassification rate for a GHQ-28 cut-off score of 6 were 84.7%, 93.8% and 8.2%, respectively. The estimated intra-class correlation between the test–retest for assessing reliability of the GHQ – 28 was 0.85.[13]
Another questionnaire was used to measure demographic variables (age, gender, education, marital status, living arrangement, participate in social activity and doing exercises) and included 10 questions.
Statistical Analysis
Data relating to the survey were analyzed with the Statistical Package for the Social Sciences, version 11.5 for Windows. We use Chi-square to compare the background variables and dependent variable in the control and intervention group before intervention. Paired-t test was used to compare the mental status before and after intervention. Independent-t test was used to identify significant variables. Sex, age, marital status, living with family and having social activity were considered as background variables. The mental health score measured as dependent variable and physical activity was an independent variable.
RESULTS
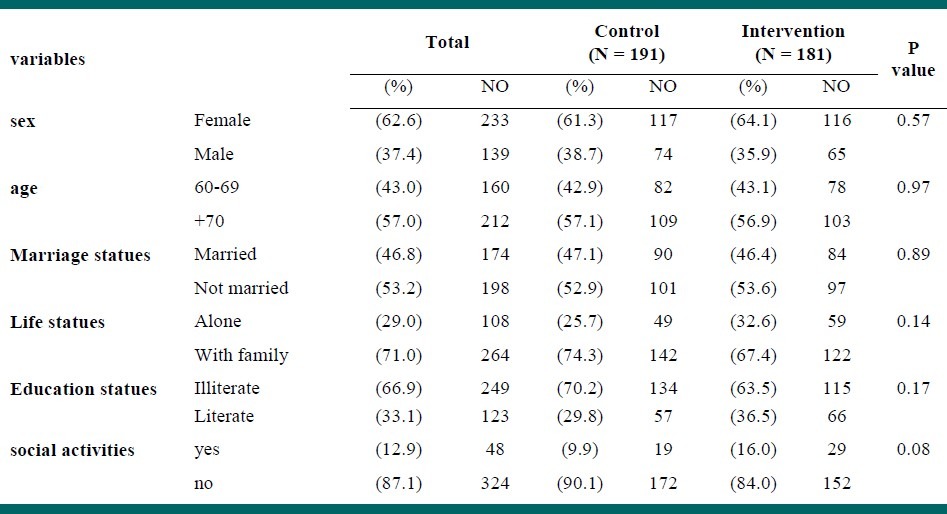
During the study, 19 persons in the case group were absent in more than three consecutive sessions and were excluded accordingly. In the control group, nine subjects were excluded due to lack of access (one person died and eight participants changed their place of living). Therefore, 372 participants (181 in the intervention group and 191 controls) finished the study (as shown in figure 1). There were 139 men (37.4%) and 233 women (62.6%). Their mean age was 71.71 ± 8.22 years. One hundred and seventy four subjects (46.8%) were married, 108 persons (29%) were living alone, 249 participants (66.9%) were illiterate and 48 participants (12.9%) had participated in social activities. There was no significant difference between background in the intervention and control groups before the study [Table 1].
Figure 1.
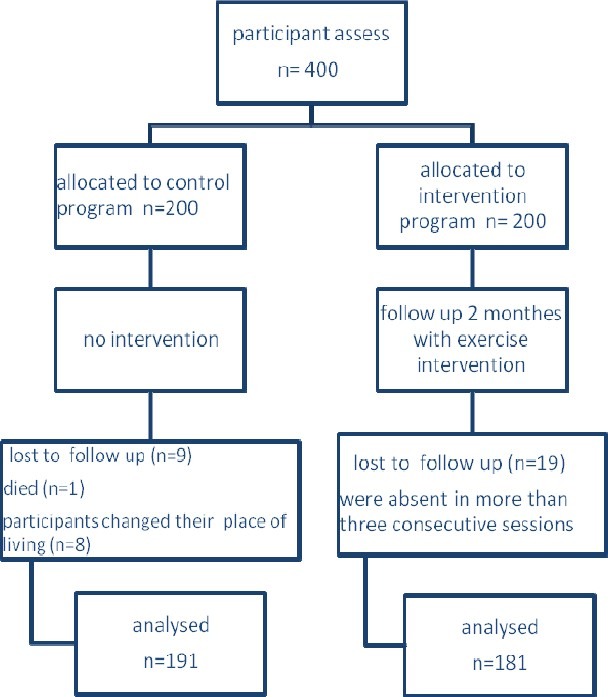
Participant flow and follow up
Table 1.
Baseline characteristics of control and intervention groups
Effect of the Intervention on Mental Health
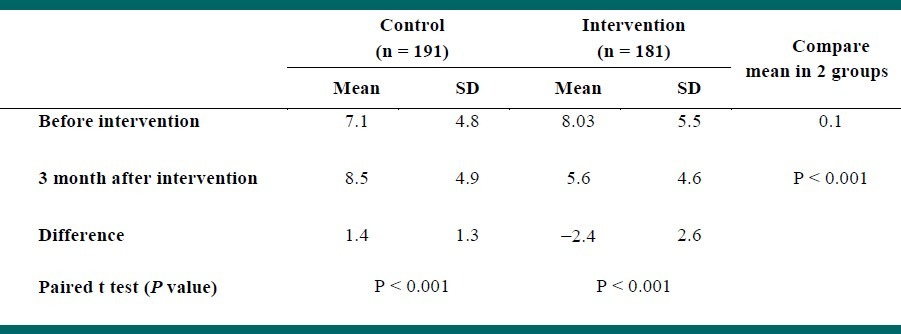
Table 2 shows changes in total mental health scores of the participants in both groups. After the intervention, the mental health status in intervention group became better and the mean score of GHQ decreased significantly (–2.4 ± 2.6), but in control group this score increased during the same period (1.4 ± 1.3).
Table 2.
Distribution of mean and standard deviation scores from the total General Health Questionnaire (GHQ-28) in intervention and control group, before and 3 months after intervention
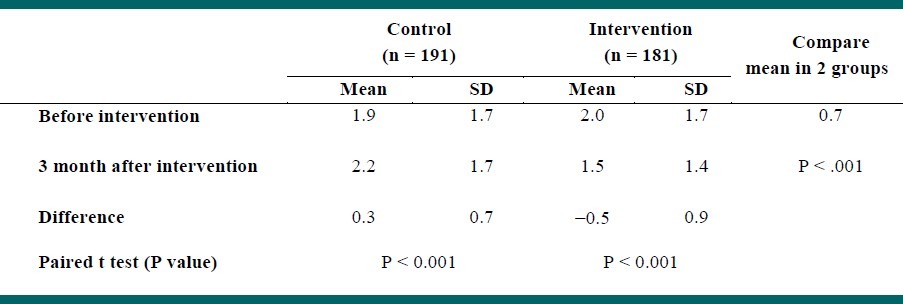
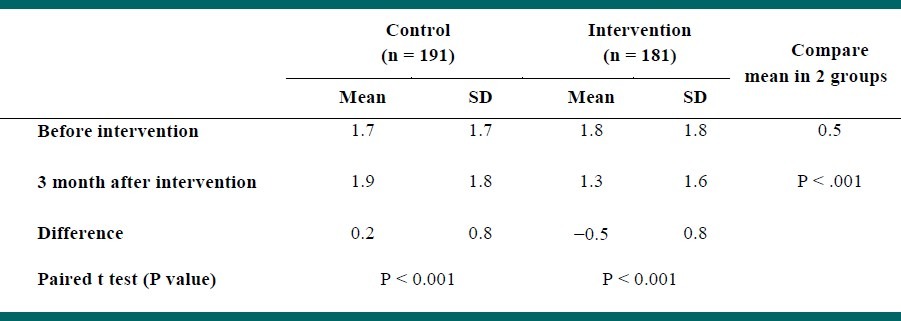
GHQ subscales improved the intervention group after doing physical activity. Moreover, there was a significant difference between intervention and control group in all these subscales. The mean score of somatization in intervention group was 2.2 ± 1.9 at the beginning of the study, which reduced to 1.5 ± 1.5 three months later (P < 0.001). Furthermore, the most significant improvement was seen in this subscale. In contrast, it increased significantly in the control group [Table 3]. Participants in physical activity group also had better score in anxiety than those in the control one after the intervention. The mean score of anxiety increased significantly in the control group three months after the study [Table 4].
Table 3.
Distribution of mean and standard deviation scores of the somatization in intervention and control group, before and 3 months after intervention
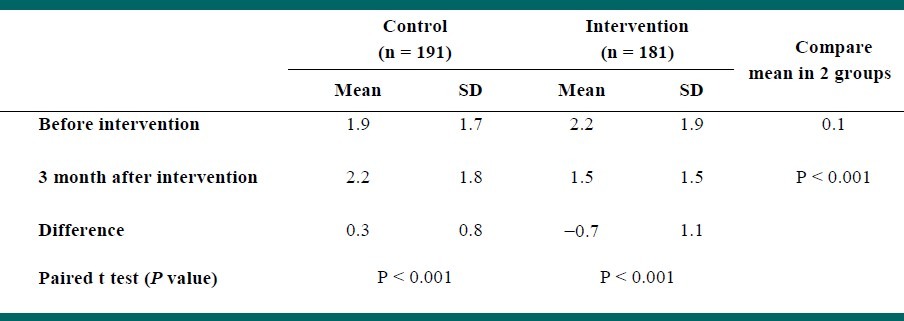
Table 4.
Distribution of mean and standard deviation scores of anxiety in intervention and control group, before and 3 months after intervention
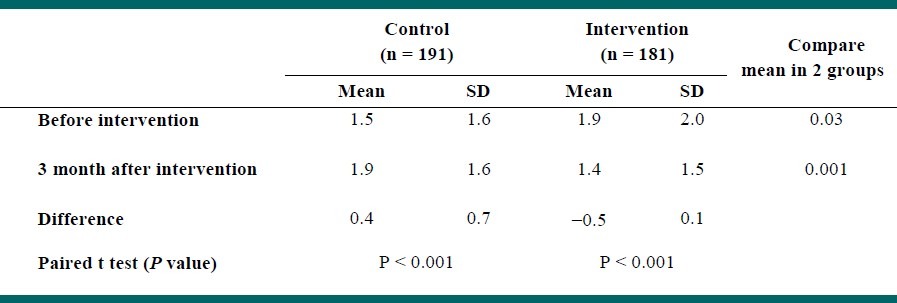
At the beginning of this study, subjects in the physical activity group had higher score of social dysfunction than those in the control group. However, three months after the study subjects in the intervention group had lower scores of social dysfunction than participants in the control group [Table 5].
Table 5.
Distribution of mean and standard deviation scores of social dysfunction in intervention and control group, before and 3 months after intervention
We also found a significant decline in the mean scores of depression in intervention group after intervention [Table 6].
Table 6.
Distribution of mean and standard deviation scores of depression in intervention and control group, before and 3 months after intervention
DISCUSSION
These research findings indicate that physical activity has positive effects on elders’ mental health. This result support Dunn Andrea et al., who suggest that physical activity improves disorders such as anxiety and depression.[18] Sandy Whitelaw et al. explained that physical activity has an effect on mental health promotion, prevention of mental disorders and treatment of these illnesses.[19] Andreas Strohle in his review showed that although the evidence for positive effects of exercise and exercise training on depression and anxiety is growing, the clinical use, at least as an adjunct to established treatment approaches like psychotherapy or pharmacothe-rapy, is still at the beginning.[20]
In addition, the results showed that physical activity can reduce somatization and the most changes are related to this scale. Mousavi Gilani and his colleagues in the study showed, there are significant differences ListRead phonetically between athletes and non-athletes in somatization scores.[21] This finding is supported by Ahmadi et al. study, which indicates a positive impact of exercise in this subscale of mental health,[22] while Hosseini et al. in their study showed the difference between athletes and non-athlete group was not significant.[23]
The results suggest that the efficacy of physical activity in reducing anxiety symptoms. This finding is confirmed by the Andreas Strohle's study that showed physical activity is associated with decrease anxiety.[20] Robert F et al.,[24] Matthew P. Herring et al.[25] and Monika Guszkowska[26] studies also confirm this results. Palleschi demonstrated that physical activity for 3 months has a greater role in reducing anxiety score in the elderly.[27]
Since social dysfunction score was different between two groups before intervention,we used difference in mean score before and after the study to evaluate the effect of our intervention. Similar to previous studies[21,22,28] we showed an improvement in social dysfunction following the intervention. Although, physical exercise was effective on reducing depression symptoms, which is confirmed in many studies,[29–32] it has the lowest effect compared with other subscales. On the other hand, Hale et al. reported that physical activity by clinical psychologists and psychiatrists as an effective intervention strategy has not been accepted.[33] Nevertheless, Dimeo and his colleagues showed that aerobic exercise or strength training significantly reduced the symptoms of depression.[34] There were some limitations for this study. First of all, selection bias and information bias might have influenced our findings. Selection bias might occur because our participants were willing to take part and we missed those who were not eager to follow the program. In the present study, interviewers were not blinded to participants’ allocation in the two groups, which might be a source of information bias. However, we tried to minimize this problem by working with trained interviewers.
CONCLUSION
According to findings of this study, doing physical activity 2 times a week for 2 months has a positive impact on mental health in general and on the four subscales somatization, anxiety, social dysfunction and depression in elder people.
ACKNOWLEDGMENT
This study was funded by Tehran University of Medical Sciences under the project number 88-02-27-8996.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Drewnowski A, Evans WJ. Nutrition, Physical Activity, and Quality of Life in Older Adults: Summary. J Gerontol. 2001;56:89–94. doi: 10.1093/gerona/56.suppl_2.89. [DOI] [PubMed] [Google Scholar]
- 2.Bastone AdC, Filho WJ. Effect of an exercise program on functional performance of institutionalized elderly. J Rehabil Res Dev. 2004;41:659–68. doi: 10.1682/jrrd.2003.01.0014. [DOI] [PubMed] [Google Scholar]
- 3.Mirzai M, Shams M. Demograghy of elder population in Iran over the period 1956 to 2006. Iran J Aging Res. 2007;5:226–31. [Google Scholar]
- 4.Center for Health Workforce Studies School of Public Health. The impact of aging population on the health workforce in the United States. University at Albany. National Center for Health Workforce Analysis. 2006. [Last cited on 2011 Apr 09]. Available from: http://www.albany.edu/news/pdf_files/impact_of_aging_full.pdf .
- 5.Sherina M, Rampal LS, Aini M, Norhidayati HM. The prevalence of depression among elderly in an urban area of Selangor, Malaysia. Int Med J. 2005;4:57–63. [Google Scholar]
- 6.WHO. Library Cataloguing-in-Publication Data. Keep fit for life: Meeting the nutritional needs of older persons. 2002 [Google Scholar]
- 7.BHF National Centre for Physical Activity and Health .Active for Later Life Promoting physical activity with older people. A resource for agencies and organizations. 2007. [[Last cited on 2011 April 09]. In: Health BNCfPAa, editor. Available from: http://www.healthscotland.com/uploads/documents/4448-ActiveForLaterLife .
- 8.Fried LP, Freedman M, Endres TE, Wasik B. Building communities that promote successful aging. West J Med. 1997;167:216–9. [PMC free article] [PubMed] [Google Scholar]
- 9.Fahlman M, Boardley D, Flynn MG, Braun WA, Lambert CP, Bouillon LE. Effects of endurance training on selected parameters of immune function in elderly women. Gerontology. 2000;46:97–104. doi: 10.1159/000022142. [DOI] [PubMed] [Google Scholar]
- 10.2nd ed. Washington DC: Government Printing Office; 2000. Healthy People 2010: Understanding and Improving Health. In: Services USDoHaH, editor. [Google Scholar]
- 11.US Department of Health & Human services. Physical Activity Fundamental To Preventing Disease. 2002. [Last cited on 2011 April 09]. Available from: http://aspe.hhs.gov/health/reports/physicalactivity/
- 12.Khoshbin S, Ghosi A, Farahani A, Motlagh ME. Tehran: Kebria; 2007. Guideline to improve healthy lifestyles during aging,Nutrition and Physical activity; p. 140. 1, editor. [Google Scholar]
- 13.Noorbala AA, Yazdi SAB, Mohammad K, et al. Validation of GHQ – 28 in Iran. Hakim Mag. 1999;5:101–10. [Google Scholar]
- 14.Khoshbin S, Eshrati B, Farahani AA, Ghosi A, Mot-lagh ME. Report of Elderly Health Survey. Ministry of Health. 2002 [Google Scholar]
- 15.Goldberg D, Hillier VF. A scaled version of the General Health Questionnaire. Psychol Med. 1979;9:131–45. doi: 10.1017/s0033291700021644. [DOI] [PubMed] [Google Scholar]
- 16.Makowska Z, Merecz D, Moscicka A, Kolasa W. The Validity of General Health Questionnairs GHQ-12 and GHQ-28, in mental health studise of working people. Int J Occup Med Environ Health. 2002;15:353–62. [PubMed] [Google Scholar]
- 17.Malakuti K, Arash M, Paridokht FE, Mogde S, Shamsodin K, Azize AE. Validity, reliability and Factor analysis of General Health Questionnaire-28 (GHQ – 28) in Iranians elderly. Iranian Journal of Aging. 2006;1:11–21. [Google Scholar]
- 18.Dunn AL, Trivedi MH, O’neal HA. Physical activity dose-response effects on outcomes of depression and anxiety. Med Sci Sports Exerc. 2001;33:S587–97. doi: 10.1097/00005768-200106001-00027. discussion 609-10. [DOI] [PubMed] [Google Scholar]
- 19.Whitelaw S, Swift J, Goodwin A, Clark D. Woodburn House, Canaan Lane, Edinburgh: NHS Scotland Health; 2008. Physical Activity and Mental Health: The role of physical activity in promoting mental wellbeing and preventing mental health problems. [Google Scholar]
- 20.Strohle A. Physical activity, fitness and anxiety disorders. J Neural Transm. 2009;116:777–84. doi: 10.1007/s00702-008-0092-x. [DOI] [PubMed] [Google Scholar]
- 21.Mousavi Gilani SR, Kianpour M, Sadeghi M. Comparison of mental health in athletes non-athlete male students. TABIB-E-SHARGH Spring. 2002;4(1):43–50. [Google Scholar]
- 22.Ahmadi E, Alizadeh SS, Shirmohamadzade M. Experimental effects of exercise on mental health in students. Motion Mag. 2005;28:19–29. [Google Scholar]
- 23.Hosseini S, Kazemi SH, Shahbaznejad L. Relationship between exercise and mental health in students. J Mazandaran Univ Med Sci. 2006;15:97–104. [Google Scholar]
- 24.Robert F, Zoeller J. Physical Activity: Depression, Anxiety, Physical Activity, and Cardiovascular Disease: What's the Connection? Am J Lifestyle Med. 2007;1:175–80. [Google Scholar]
- 25.Herring MP, O’Connor PJ, Dishman RK. The effect of exercise training on anxiety symptoms among patients: A systematic review. Arch Intern Med. 2010;170:321–31. doi: 10.1001/archinternmed.2009.530. [DOI] [PubMed] [Google Scholar]
- 26.Guszkowska M. Age and exercise duration as determinants of the efffect of single bout of exercise on state anxiety in women. Sport Medicine Journal. 2009;13:125–30. [Google Scholar]
- 27.Palleschi L, Gennaro E, Sottosanti G, Vetta F, Ronzoni S, Lato PF, et al. The role of exercise training in aged subjects with anxiety-depression syndrome. Gerontol Geriatr. 1998;26:381–4. [Google Scholar]
- 28.Esfahani N. Effect of exercise on mental health in somatization, anxiety, sleep disorders, social dysfunction and depression in Azahra University students. Motion Mag. 2002;12:75–87. [Google Scholar]
- 29.Motl RW, Birnbaum AS, Kubik MY, Dishman RK. Naturally Occurring Changes in Physical Activity Are Inversely Related to Depressive Symptoms During Early Adolescence. Psychosom Med. 2004;66:336–42. doi: 10.1097/01.psy.0000126205.35683.0a. [DOI] [PubMed] [Google Scholar]
- 30.Singh NA, Clements KM, Singh MA. The efficacy of exercise as a long-term antidepressant in elderly subjects: A randomized,controlled trial. J Gerontol A Biol Sci Med Sci. 2001;56:M497–504. doi: 10.1093/gerona/56.8.m497. [DOI] [PubMed] [Google Scholar]
- 31.Benedetti TR, Borges LJ, Petroski EL, Gonçalves LH. Physical activity and mental health status among elderly people. Rev saode poblica. 2008;42:1–6. [PubMed] [Google Scholar]
- 32.Antunes HK, Stella SG, Santos RF, Bueno OF, de Mello MT. Depression, anxiety and quality of life scores in seniors after an endurance exercise program. Rev Bras Psiquiatr. 2005;27:266–71. doi: 10.1590/s1516-44462005000400003. [DOI] [PubMed] [Google Scholar]
- 33.Hale A. S. ABC of mental health: Depression [database on the Internet] BMJ. 1997 Jul 5;315(7099):43–46. doi: 10.1136/bmj.315.7099.43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Dimeo F, Bauer M, Varahram I, Proest G, Halter U. Benefits from aerobic exercise in patients with major depression: A pilot study. Br J Sports Med. 2001;35:114–7. doi: 10.1136/bjsm.35.2.114. [DOI] [PMC free article] [PubMed] [Google Scholar]