

Abstract
Objectives:
Infected hospital wastes are among hazardous wastes, and special treatment methods are needed for their disposal. Having information about present status of medical waste management systems is of great importance in finding weak, and for future planning. Such studies have not been done for most of the hospitals in Iran.
Methods:
This paper reports the results of a study on the present status of medical waste management in Isfahan hospitals. A ten page researcher made questionnaire was used to collect data in terms of collection, transportation, segregation, treatment and disposal. For assessment of autoclaves, standard tests including TST (Time, Steam, and Temperature) strip test and spore tests were used. Samples were made of stack gases of incinerators. Quantity and composition of hospital wastes in Isfahan were also measured manually.
Results:
Of all wastes in selected hospitals, 40% were infected wastes (1.59 kg/day/bed), which is 15 to 20% higher than World Health Organization (WHO) standards. TST and Spore test results were negative in all samples. Stack gases analysis showed high concentration of CO in some samples. Besides, the combustion efficiency in some samples is less than 99.5%, which is the standard criterion in Iran.
Conclusions:
This study may create awareness regarding the magnitude of the problem of waste management in hospitals of Isfahan and may stimulate interests for systematic control efforts for hospital waste disposal. Hospital waste management cannot succeed without documented plans, certain equipment, defined staff trainings, and periodic evaluations.
Keywords: Autoclave, Hospital, Incineration, Infected wastes, Isfahan, medical waste management
INTRODUCTION
Medical waste is an issue of growing concern since it is a source for contamination and pollution, capable of causing diseases and illness either through direct contact or indirectly by contamination of soil, ground water, surface water and air. The health care establishments are an integral part of the life support system. Improper disposal of waste generated from such establishments can have direct and indirect health impacts as well as posing a potential threat to the surrounding environment, people handling it and the public in general. There is an urgent need to improve upon the medical waste management practices in the country based on systematic and scientific planning of medical waste management.[1]
The medical wastes’ disposal has been a serious problem in urban areas. The appropriate disposal of these hazardous wastes requires the development of waste management systems to reduce their effects on the environment.
Applying an organized medical waste management system is necessary in any community to subdue environmental hazards from contamination by these wastes. Like any other waste management system, waste reduction is the first step in medical waste management. Thus, applying a source reduction system in hospitals through training personnel is very important. The amount of medical waste generated depends on the factors which may be different not only in various countries, but also between different cities of a country. Composition of medical wastes may also be different.[2] Medical wastes are composed of infected and non-infected ones. The non-infected wastes may be disposed like municipal solid wastes, but infected part needs special treatment before disposal. Thus, good separation of these two parts is very important in optimizing the treatment procedures and making the waste management practices cost effective.
Many case studies have been implemented in different foreign cities, investigating the quantity, composition and physiochemical characteristics of medical wastes. In Iran, such studies have been done in very few cases. More studies need to be implemented to make officials able to draw a realistic scheme of the present status of the medical waste management in Iran.
The amount, composition and physiochemical characteristics of the infected wastes are among the main factors in the selection of a treatment method. Two major treatment methods are being used in Iran. Incineration is the first and the most popular method in Iran to treat medical wastes, but it has recently faced many obligations due to toxic emissions. Autoclaves are newer devices used in Iran for this purpose.
The city of Isfahan is the capital of Isfahan province. According to the census in 2007, the population of the province was 4,559,256 of which approximately 83.3 percent were urban residents and 16.7 percent resided in the rural areas. The city of Isfahan has a population of 602110. Isfahan has 25 hospitals and 21 clinics, which totally have 5460 beds.
Previous Case Studies
Foreign Cities
In 2009, Birpinar, Bilgili and Erdoğan analyzed the present status of medical waste management, in the light of the Medical Waste Control Regulation (MWCR) in Istanbul. They showed that the estimated quantity of medical wastes from a hospital is about 22 tons/day and the average generation rate is 0.63 kg/bed/day. Recyclable materials are collected separately at a rate of 83%. Separate collection of different types of wastes is consistently practiced, but 25% of the hospitals still use inappropriate containers for medical waste collection, and nearly 23% of them have inappropriate equipment for their personnel. The percentage of hospitals that have temporary storage depots is 63%. Medical waste management in Istanbul is carried out by applying the MWCR.[3]
In Nanjing, China, Yong and Guanxing, Tao and Dawei found that medical waste generation rate ranges from 0.5 to 0.8 kg/bed/day with a weighted average of 0.68 kg/bed/day. The segregated collection of various types of medical waste has been conducted in 73% of the hospitals, but 20% of them still use unqualified staffs for medical waste collection. Additionally, 93.3% of the hospitals have temporary storage areas. However, only 20% of the hospitals have ongoing training and education. It was found that a centralized disposal system has been constructed based on incineration technology, and the disposal cost of medical waste is about 580 US $/ton. The results also suggested that there is no sufficient public commitment about medical waste management, and just 77% of respondents think medical waste management is an important factor in selecting hospital services.[4]
In northern part of Jordan, Bdour, Altrabsheh, Hadadin and Al-Sharif showed that there are no specific regulations or guidelines for segregation or classification of infected wastes. Furthermore, none of the sites surveyed could provide estimated quantities of waste generated by each department, based upon the known variables within the departments. Average generation rates of total medical wastes in the hospitals were estimated to be 6.10 kg/patient/day (3.49 kg/bed/day), 5.62 kg/patient/day (3.14 kg/bed/day), and 4.02 kg/patient/day (1.88 kg/bed/day) for public, maternity, and private hospitals, respectively. For medical laboratories, rates were found to be in the range of 0.053– 0.065 kg/test/day for governmental laboratories, and 0.034–0.102 kg/test/day for private laboratories. Although, based on their type, domestic or general waste makes up a large proportion of the waste volume, so that if such wastes are not mixed with patient derived wastes, they can be easily vanished. However, it is important for healthcare staff to take precautions in handling sharp and pathological wastes, which comprises only about 26% of the total infectious wastes.[5]
Waste generation rate in Daro-Salaam (Tanzania) hospitals in 1993 were reported to be between 0.84 and 5.8 kg/bed/day.[6]
Another study on European hospitals showed that there were incinerators for hospital waste disposal except Sabadell Hospital.[7]
Iran Cities
According to Amouei, in 2003 the waste generation rate in three major hospitals in Babol was 2.01 kg/patient/day of which 0.67 kg was infected wastes. Furthermore, the average density of the wastes was 313 kg/m3.[8]
Taghipour and Mosafer in a study to determine the quantity, generation rate, quality, and composition of medical waste generated in Tabriz indicated that the average (weighted mean) of total medical waste, hazardous–infectious waste, and general waste generation rates in Tabriz city are 3.48, 1.039, and 2.439 kg/bed-day, respectively. In the hospital studies, wastes consisted of 70.11% general waste, 29.44% of hazardous–infectious waste, and 0.45% of sharp waste. The average composition of hazardous–infectious waste was determined to be 35.72% plastics, 20.84% textiles, 16.70% liquids, 11.36% paper/cardboard, 7.17% glass, 1.35% sharps, and 6.86% others. The average composition of general waste was determined to be 46.87% food waste, 16.40% plastics, 13.33% paper/cardboard, 7.65% liquids, 6.05% textiles, 2.60% glass, 0.92% metals, and 6.18% others. The average bulk densities of total medical waste, hazardous–infectious waste, and general waste were determined to be 99.58, 96.16, and 101.26kg/m3, respectively.[9]
Omrani and his team found that medical waste composition in Shahrekord was as follows: 14.0% food wastes, 11.6% plastics, 4.6% papers, 4.4% glasses, 1.4% metals, 4.8% textiles, 2.2% nylons, 57% other wastes. They found that infected and non-infected waste generation rate is 1.04 kg/patient/day and 2.44 kg/patient/day, respectively.[10]
METHODS
Data Collection
Data collected were based upon a 10 page researcher-made questionnaire distributed to 10 hospitals. Questionnaires were used to survey the hospital wastes in terms of collection, transportation, segregation, treatment, and disposal and to collect available information for system analysis. Other data such as waste generation rate and composition were measured in field by researcher.
Sampling and Analysis
The collection of clinical waste samples and analysis were carried out in December 2009 to April 2010 with standard methods. The waste characterization study was carried out in accordance with the latest WHO guidelines.[11] All of the wastes generated in 10 hospitals were segregated and weighed during a period of five months, manually. Environmental health experts as well as members of the nosocomial infection control committee of hospitals or managers of waste transportation, collection and sorting, provided data in terms of collection, transportation, segregation, treatment and disposal. The quantity and composition of the wastes were determined at each hospital. Along with the interviews, the physical compositions of wastes in hospitals were determined. Before segregation, wastes were sprayed by disinfectant solution (0.5% sodium hypochlorite). Masks and large forceps were used when dividing waste into several types. During separation, each type of medical waste was discarded into bags. General and medical wastes from outpatient and inpatient services were collected separately. The medical wastes were previously sorted into various components such as serum, syringe and needle (in safety boxes), etc. Then, wastes were transported to a special site for storage and final disposal.
The raw survey data was compiled and managed to enable the estimation of waste generation quantities and management practices.
Samples were made from stack gases of incinerator in Fatemeh-Zahra hospital to evaluate the combustion efficiency, using standard IMR 2800 instrument.
The treatment efficiency of a pre-vacuum autoclave in Amin hospital was evaluated using TST and spore tests. TST which is a chemical test was done in every autoclave cycle. If the sensitive orange mark of the test changed into gray, the tests are acceptable. If the color was different, the test has to be repeated. If results of TST test were still unacceptable, then the spore test was done. Spore test was done every two weeks or in emergency conditions. These purple tests contained Bacillus stearothermophilus. After each autoclave cycle, tests were incubated for 48 hours in 60°C. If the color did not change, the test is acceptable [Figures 1 and 2].
Figure 1.

TST test of pilot autoclave of Amin Hospital
Figure 2.

Comparison of spore tests with samples
Data Analysis
Quantities of hospital wastes were presented in terms of kg/day for a total amount of waste generation. The data gathered from the questionnaire were compiled by statistical Excel and SPSS.
RESULTS
Hospitals Status
In Isfahan, most of the hospitals do not have any facilities to treat their wastes. They collect their wastes, and through a contracted agreement, the urban services’ organization of the municipality conducts these wastes out of the hospital every two days. These hospitals have a source separation system to separate infected wastes from non-infected. Unfortunately, this organization performs no treatment on these wastes and buries them in a not well-operated landfill located at Zainal Neck near Isfahan. There is only one active incinerator in Fatemeh Zahra hospital and a pre-vacuum autoclave in Amin hospital.
Average medical waste generation in Isfahan hospitals is shown in Table 1. Average medical waste generation in different cities of Iran is shown in Table 2.[8,9,12,13]
Table 1.
Average medical waste generation rate in Isfahan hospitals (kg/day/bed)
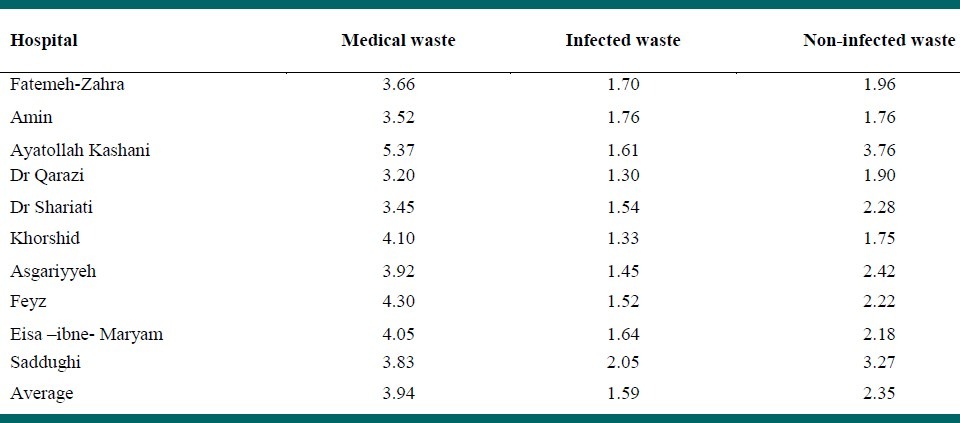
Table 2.
Average medical waste generation rate in different cities of Iran

Comparing the per capita rate of different types of wastes in Isfahan with WHO standards show that the medical waste generation in Isfahan is higher than its normal value for East Mediterranean countries.[11] The comparison of waste generation rate in Isfahan with WHO Standard is shown in Figure 3.
Figure 3.

Comparison between waste generation rates in Isfahan with WHO Standard (kg/bed/day)
Hospital Waste Composition
The percentages of medical waste composition (infected and non-infected waste) in Isfahan hospitals are shown in Figures 4 and 5. The comparison of this item with other cities of Iran is shown in Figure 6.
Figure 4.

Non-Infected Medical Waste Composition in Isfahan's Hospitals
Figure 5.

Infected Medical Waste Composition in Isfahan's Hospitals
Figure 6.

Comparison of Medical Waste Composition with other cities of Iran
Waste Collection Methods and Time Duration
In all hospitals, infectious wastes were segregated from other wastes. Yellow bins were used for infected wastes and blue bins were used for non-infected wastes [Figure 7]. In general, in most of the hospitals, suitable and adequate number of containers was used and kept at proper places. In five of the hospitals, after these bins were full, they were emptied into larger bins and were carried to the temporary storage site using trolleys. White bins were considered for non-infected and red bins for infected wastes. To prevent bad odors, the temperature of storage sites was kept low around 10°C. Sharps were collected using special yellow safety boxes.
Figure 7.

Bins used to collect infected (yellow) and non-infected wastes (blue)
In six of the hospitals, wastes were collected at the end of each shift at 8:00 am, 2:00 pm and 8:00 pm. Hospital wastes were collected and transported to a temporary storage area by hospital staff. In two hospitals, medical wastes were collected daily and in 3 other hospitals, the collection program was unsteady. In five of the hospitals, these wastes were collected by trolleys, in five hospitals manually, and in one hospital both the systems were applied. The staff employed for handling the wastes in all hospitals used almost complete personal protective equipment (the protective equipment included special gowns, shirts and trousers along with at least two of the followings: Gloves, mask, boots, and apron).
In all studied hospitals, there were temporary storage sites. The distance between these sites to the nearest department was about 10–70 m. These sites included metal containers (1 hospital), concrete rooms (1 hospital), special rooms (7 hospitals), and open enclosure sites (2 hospitals). The infectious and non-infectious wastes were kept in separate containers and were not mixed in the hospital's temporary storage area. Only 8 hospitals had a well sanitized and secured temporary storage area, and the others had well secured, but poorly sanitized one. The storage time in those sites was 24 h (8 hospitals) and 24–48 h (3 hospitals).
The only autoclave under operation in Isfahan is in Amin hospital. As mentioned before, the treatment efficiency of this pre-vacuum autoclave was evaluated using TST and spore tests. TST and Spore Test results were negative in all samples. No needle stick was observed in autoclave cycles.
As previously mentioned, to evaluate the efficiency of the incinerator in Fatemeh Zahra hospital, 20 samples were made from stack gases of the incinerator with an IMR 2800. This device could measure six different gases and the temperature of the gases at the same time. The results are shown in Table 3.
Table 3.
Comparison of incinerator's stack gases analysis results with WHO standard values

Due to Table 3, the concentration of all pollutants in all samples is below WHO standards.[14] Only the maximum concentration of CO in samples is 4.5 times more than standard values. This high quantity of CO implies the incomplete combustion in the incinerator or the lack of oxygen during the incineration process. Since CO is one of the main pollutants, it is environmentally hazardous.
Due to the medical wastes administrative management regulations of waste management law of Iran, the combustion efficiency (CE) of incineration must be at least 99.50%, which is calculated as follows (Eq. 1):[15]

The CE for the average concentrations of samples would be 99.82%, which is in the norm range. In the worst condition (the maximum CO concentration, the minimum CO2 concentration), the CE is 98.05%.
DISCUSSION
Source separation was implemented in all hospitals under studied, but unfortunately these segregated wastes were finally mixed again in landfill. This means that waste management is not a continuous process in Isfahan.
According to Figure 3, the quantity of infected waste is 15 to 20% higher than WHO standards. Also from Table 2, it may be found that the percentage of infected waste in Isfahan is higher than all other Iranian cities under study. Comparing the infected and non-infected content of the medical waste in Isfahan with foreign cities also indicated its high amount. However, Jordan competes with Iran in producing high amounts of medical wastes. This may be mostly due to an inappropriate segregation process of wastes in Isfahan hospital, which shows the need to train personnel in this regard.
As may be seen from Figure 4, a great part of non-infected wastes in Isfahan is food waste. This indicates the poor consumption culture. It also shows the high potential of this waste to be recovered as methane in landfills.
From Figure 5, it is observed that a high amount of infected wastes are recyclable. Due to high percentage of infected waste in Isfahan hospitals compared to WHO standards which might be due to inappropriate segregation processes, it may be concluded that with a better segregation process, a great part of these recyclable wastes can be classified as infected and may be recycled before disposal.
Figure 6 shows that the plastic content of medical wastes in Isfahan is high compared to other cities and by applying appropriate segregation systems, a great portion of this content may be recycled. Metal waste consist almost the same percentage in all cities. The percentage of medical wastes in Shahrekord is different from the average pattern among other cities, which implies the need to reconsider the reported amounts.
Unfortunately, devices to measure the concentration of Furans and Dioxins from incinerator's stack gases were not available. Because of the absence of air pollution control devices like wet scrubbers, high concentration of these toxic and carcinogenic emissions is very probable. Thus, any judge about the stack gases’ analysis must be done by care. The CE is calculated to be 98.05% and thus, the incineration efficiency is not acceptable. This implies the necessity of air pollution control devices.
According to results, the studied hospitals need a more efficient disposal process to manage the hospital waste, particularly infectious one. The following discusses some of the problems and procedures associated with medical wastes of Isfahan:
Lack of comprehensive waste disposal plans for disposal and other technical aspects of hazardous wastes.
Lack of treatment facility such as incinerator or autoclaves for treatment of pathological and infectious wastes in most of the hospitals.
Lack of continued segregation, collection, transportation, and final disposal of infectious and other medical wastes.
Lack of sufficient knowledge and awareness among the hospital staff about the consequences of the potential risk of infectious, hazardous waste, and environmental impact.
Lack of proper guidelines, regulations, and instructions on the management of healthcare waste such as separation, collection, and disposal of various categories of wastes in a suitable manner to render it harmless.
In three of the /hospitals, wastes storage time was too much, which could probably result in odor problems as well as health hazards.
Disposal of liquid waste into the municipal sewerage system and MSW landfill without any prior treatment.
The basic approach to medical waste management is to reduce the quantity of waste at original source as much as possible. Hospital wastes should be recycled whenever feasible, with regard to the environmental aspects, to reduce the quantity of material entering the waste system.
Waste management requires a systematic approach, involving the handling, storage, transportation; treatment and disposal of waste by methods that at all stages minimize the risk to health and the environment.
All hospital personnel should be made aware of the potential risk of mishandling wastes.
This study may create awareness regarding the magnitude of the problem of waste management in hospitals of Isfahan and has generated interest for systematic control efforts for hospital waste disposal. Hospital waste management cannot succeed without documented plans, certain equipment, defined staff trainings, and periodic evaluations.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Shirazi A. Examination of the medical waste management in Yasouj in 2006. Med Univ Yasouj’ Res. 2008;15:253–300. [Google Scholar]
- 2.Eugene C, Cole T, Pierson K. Guidance for evaluating medical waste treatment technologies, Research Triangle Inst. 1998 [Google Scholar]
- 3.Birpinar M, Bilgili M, Erdoğan T. medical waste management in Turkey: The case study of Istanbul. Waste Manag. 2009;29:445–8. doi: 10.1016/j.wasman.2008.03.015. [DOI] [PubMed] [Google Scholar]
- 4.Yong Z, Gang X, Guanxing W, Tao Z, Dawei J. Medical Waste Management in China: A Case Study of Nanjing. Waste Manag. 2009;29:1376–82. doi: 10.1016/j.wasman.2008.10.023. [DOI] [PubMed] [Google Scholar]
- 5.Bdour A, Altrabsheh B, Hadadin N, Al-Shareif M. Assessment of medical wastes management practice: A case study of the northern part of Jordan. Waste Manag. 2007;27:746–59. doi: 10.1016/j.wasman.2006.03.004. [DOI] [PubMed] [Google Scholar]
- 6.Mato RR, Kaseva ME. Critical Review of Industrial and Medical Waste Practices in Dar es Salaam City. Resour Conserv Recy. 1999;25:271–87. [Google Scholar]
- 7.Muhlich M, Scherrer M, Daschner FD. Comparison of Infectious Waste Management in European Hospitals. J Hosp Infect. 2003;55:260–8. doi: 10.1016/j.jhin.2003.08.017. [DOI] [PubMed] [Google Scholar]
- 8.Amou’ei A. Determination of the Type and Quantity of the Medical Wastes in Major Hospitals of Babol in 2001. Med Univ Babol’ J. 2003;4:347–52. [Google Scholar]
- 9.Taghipour H, Mosafer M. Characterization of Medical Waste from Hospitals in Tabriz, Iran. Sci Total Environ. 2009;407:1527–35. doi: 10.1016/j.scitotenv.2008.11.032. [DOI] [PubMed] [Google Scholar]
- 10.Omrani Q, Etabi F, Sadeghi M, Banaei B. The comparison of technical, environmental and economical aspects of autoclaving, incineration and landfilling in medical wastes disposal. Environ Sci Technol. 2007;2:147–58. [Google Scholar]
- 11.Pruss A, Giroult E, Rushbrook P. Chapter 2: Definition and Characterization of Health-Care Waste. World Health Organization; 1999. Safe Management of Wastes from Health-Care Activities; pp. 12–18. [Google Scholar]
- 12.Masoumbeigi H, Karimi-Zarchi A, Tajik J. Examination of the Quantitative Condition of Medical Wastes in one the Major Specialized Hospitals of Tehran. Marital Med J. 2007;24:127–35. [Google Scholar]
- 13.Shirazi A. Examination of the Medical Waste Management in Yasouj in 2006. Med Univ Yasouj’ Res. 2008;15:253–300. [Google Scholar]
- 14.Pruss A, Giroult E, Rushbrook P. Chapter 8: Treatment and Disposal Technologies for Health-Care Waste. World Health Organization; 1999. Safe Management of Wastes from Health-Care Activities; pp. 77–112. [Google Scholar]
- 15.Medical Wastes Administrative Management Regulations of Waste Management Law of Iran. Commission of Sub Structural Affairs. Industry and Environment. 2008 [Google Scholar]