

Abstract
This paper examines crash characteristics and the resulting injuries to occupants whose seat position is on the side of impact in a vehicle exposed to a side collision. The databases of the 1988–96 NASS/CDS and the 1995–98 William Lehman Injury Research Center (WLIRC) are examined in this study. The subset of cases analyzed is those in which there is a vehicle-to-vehicle near-side collision, occupant compartment damage and no subsequent collision or rollover. The WLIRC data contains highly detailed occupant injury data not available in NASS.
The WLIRC database 1995–1998 contains 92 side impact cases. Sixty-four cases involved occupants seated on the side impacted. The 64 near-side impacts are filtered according to object struck, presence of occupant compartment damage and no subsequent collision or rollover, resulting in a total of 46 cases.
The NASS/CDS database injuries are described on the basis of body region and severity. The most frequent MAIS 3+ injured body regions in NASS/CDS are: chest/abdomen 49%, head/face 24%, pelvic/lower extremity 14%, and neck/spine 4%. The largest sources of AIS 6 injuries in the NASS/CDS are arterial injuries, followed by brain and heart injuries. The WLIRC data is more representative of severe crashes than NASS in terms of struck vehicle lateral delta-V and side crush and provides more detailed injury descriptions. In comparison to NASS/CDS, this database contains a higher percentage of the following chest/abdominal injuries: thoracic aorta 15%, heart 11%; and spleen 11%. MAIS 3+ head injuries occur in 17% of cases studied. The organs most frequently causing fatalities are: brain 21%, thoracic aorta 21%, and heart 18%.
The WLIRC data contains 21 occupants in near-side vehicle-to-vehicle crashes with MAIS 3+ brain injury. Overall, the most frequent source of brain injury was the striking vehicle (35%).
Heart injuries were present in 6 of the WLIRC cases, all fatal. These cases were severe crashes with a lateral delta-V for the struck vehicle in excess of 13.4 m/s or a vehicle side crush in excess of 0.61 meters. The lower side interior was the contact in 5 cases and the shoulder belt was the contact in one case. The existing triage criteria identified brain and heart injuries at the scene.
The WLIRC data contains 12 cases of thoracic aortic injury. There were 11 fatalities; it is of note that 8 of the 12 initially survived the crash and were transported to a hospital. Development of additional crash scene triage criteria could be vital to assist in the early identification of these difficult-to-detect, time-critical aortic injuries. Several similarities were observed regarding the vehicle damage patterns among seven cases with the least severe door intrusion. These include: oblique principal direction of force (PDOF) relative to the struck vehicle, direct damage to the struck vehicle beginning at the front wheels and damage on the door at a high vertical level, often with limited sill intrusion. Other factors include: older occupants, female occupants, and an unrestrained occupant on the far side of the vehicle.
METHODOLOGY AND DATABASES
The data sources for this analysis are the National Accident Sampling System/Crashworthiness (NASS/CDS) database, 1988 to 1996, and the William Lehman Injury Research Center (WLIRC) database, 1995 to 1998. The NASS/CDS is used to examine overall injury distribution in near-side collisions. The WLIRC database is used for in-depth analysis of the characteristics of the crashes and the injuries among occupants who are severely injured in near-side collisions.
The National Highway Traffic Safety Administration (NHTSA) maintains the NASS/CDS database of vehicle crashes in the United States. The NASS/CDS, is a nationally representative sample of light vehicles involved in highway crashes of any severity that were reported by the police and involved sufficient damage that one vehicle was towed from the crash scene. The database was compiled between 1988 and 1996 and is used extensively by NHTSA and others to assess the distribution of crashes and injuries occurring annually on US highways. Prior to 1986, the NASS sampled a broader range of crashes. The NASS ‘85 was a stratified sample of all police reported crashes and contained many crashes with minor or no injuries.
The WLIRC database provides in-depth crash and injury information on a census of the most severely injured motor vehicle occupants in Miami-Dade County, Florida. Since 1995, the William Lehman Injury Research Center at the University of Miami School of Medicine has investigated 92 side impact collisions. In each case, the occupant was either transported to the Ryder Trauma Center (RTC) at the University of Miami/Jackson Memorial Medical Center, or directly to the Dade County Medical Examiner’s Office. Detailed data has been collected from the crash scene, the damaged vehicle, and the injured occupant(s).
The criteria for admission to the WLIRC side impact study is as follows: (1) the subject must have been involved in a side collision, (2) the subject must not have been completely ejected from the vehicle, (3) the subject must have met trauma triage criteria and (4) the subject must sign a written consent to participate. Criteria (3) and (4) do not apply in medical examiner cases. Subject screening is 100% of all occupants involved in side collisions arriving at either the RTC or the Dade County Medical Examiner’s office. Less than 10% of the subjects who met study criteria refused to participate.
Fire rescue personnel in Miami-Dade County employ the use of trauma triage criteria as indicators of injury severity and appropriate selection of occupant transport protocols. At the scene of a crash, if an injured occupant meets any one of the following criteria, trauma center transport is required. All but one are measurable/objective parameters defined by the Florida Department of Health and Human Services. The paramedic high index of suspicion criteria is a county added option. It is designed to give flexibility to experienced rescue personnel in cases where a subject may not meet any other criteria, but where other factors at the scene may lead to the suspicion of injury.
Systolic BP ≤ 90 (Shock)
Respiratory rate < 10 per minute or > 29 per minute
Glasgow Coma Scale ≤ 12
Penetrating injury to head, neck, chest, abdomen or groin
Paralysis
Second or third degree burns ≥ 15% Total Body Surface Area
Amputation proximal to wrist or ankle
Paramedic Judgment — High Index of Suspicion of Injury
FACTORS INFLUENCING INJURY LOCATION AND SEVERITY
In the analysis of data and previous studies involving side impact collisions, there appears to be four primary factors which influence the location and severity of occupant injuries: collision type, occupant exposure, impact location, and crash direction. Seat belt use does not seem to be a significant factor. Results reported by Jones (1982), Dalmotas (1983), Rouhana (1983), and Fildes, (1990), found that in near-side crashes, belt use was effective in reducing ejection and rebound impacts, but did not appreciably influence the injuries from initial impacts with interior vehicle surfaces.
Earlier studies have found that the two most important parameters in classifying lateral impacts are: (1) the impact location on the vehicle, whether inside or outside the passenger compartment region, and (2) the occupant seating position, whether on the impacted or opposite side (Otte, 1984). Crashes involving fixed objects, particularly narrow fixed objects have been found to be more hazardous than vehicle-to-vehicle crashes (Malliaris, 1992).
Conflicting conclusions have been reported regarding the most hazardous crash direction. Rouhana (1983) reported that the 10 and 2 o’clock directions were most hazardous while Otte (1984) found ‘rectangular’ crashes to be equally hazardous, and Reidelbach (1983) determined ‘rectangular’ crashes to be more hazardous.
The four primary factors influencing injury severity and location are applied to the NASS ’85 (Hackney, 1987), NASS/CDS and WLIRC databases. Table 1 compares distributions of side crashes by collision type (fixed object versus vehicle-to-vehicle), the occupant’s position relative to the crash, impact and damage location, and crash direction in AIS 3+ injured occupants.
Table 1.
MAIS 3+ Injured in NASS and WLIRC Databases
| CRASH COMPARISON | NASS 85 | NASS/CDS | WLIRC |
|---|---|---|---|
| Collision Type | |||
| Vehicle-to-vehicle | 72% | 75% | 78% |
| Fixed object | 28% | 25% | 22% |
| Occupant Exposure | |||
| Near Side | 67% | 66% | 70% |
| Far Side | 33% | 34% | 30% |
| Impact Location | |||
| Pax Compartment | 90% | 94% | 94% |
| Other | 10% | 6% | 6% |
| Crash Direction | |||
| 1&11 | 15% | 2% | 11% |
| 2&10 | 46% | 64% | 76% |
| 3&9 | 32% | 27% | 11% |
| 4&8 | 7% | 7% | 2% |
In all three data sets, the most frequent crash mode for the injured occupants is the vehicle-to-vehicle crash. The injured occupants are most frequently seated on the struck side of the vehicle, and the vehicle is damaged in the location of the seated occupant. Crashes with other vehicles comprised approximately 75% of the cases. Near-side occupants made up 66% of the MAIS 3+ injured in the NASS and 70% in the WLIRC. Near-side crashes with fixed objects constitute approximately 25% of the AIS 3+ injured occupants in NASS/CDS. The WLIRC database contains 22% fixed object impacts in which near-side occupants were injured.
Passenger compartment impacts accounted for 94% of the seriously injured occupants in near-side impacts in both the WLIRC and the NASS/CDS data, with 90% in the NASS ’85. The distribution of crash direction varies considerably among the databases. The crash direction variable (PDOF) is frequently difficult to assess precisely in side crashes, yet in all three databases impacts with angular PDOF are more frequent than impacts with perpendicular PDOF. As noted by Rouhana (1983), the 10 and 2 o’clock directions are the most injurious crash directions in all.
The comparisons in Table 1 indicate that the WLIRC data is very similar to the NASS databases with regard to the side collision type, occupant location, and damage location. It is higher with regard to the most injurious PDOF in the 2 and 10 o’clock and lower in the 3 and 9 o’clock directions. Given that the WLIRC data contains highly detailed occupant injury data not available in NASS, the injury patterns documented can be further examined for representativeness using the NASS/CDS.
INJURIES AND CRASH CHARACTERISTICS IN NEAR-SIDE COLLISIONS BY TYPE
Fixed Object Near-Side Impact Collisions
Crashes involving fixed objects, particularly narrow fixed objects have been found to be more hazardous than vehicle-to-vehicle crashes (Malliaris, 1992). Morris (1993) examined head injuries in UK side crashes and found that exterior objects were the most frequent source of AIS 3+ head injuries.
This is consistent with the findings in the WLIRC database. The frequency of fixed object side impacts is significantly less than vehicle-to-vehicle collisions, yet the fatality rate is very high (79%).
The vast majority of these crashes (86%) were impacts with narrow objects such as poles or trees. The injured occupants were young, the average age being 27.7 years. The crashes involved severe side crush, ranging from 0.38 to 1.1 meters with an average of 0.85 meters.
All but one of the fatally injured occupants was dead at the scene. Injured occupants suffered as many as 12 AIS 3+ injuries to different body organs. The average number of body organs injured per occupant was 5.
Severe brain injuries were present in 71% of the occupants. The most frequent contacts causing serious brain injuries were the B-pillar, the struck fixed object, and the roof rail.
Severe chest/abdominal injuries were present in 79% of the occupants. The most frequent organ injuries were as follows: lung 64%, rib 43%, aorta 36%, liver 29% and heart, spleen, bladder and kidney 24%. The side interior of the vehicle, including the B-pillar, was the most frequent contact that caused chest/abdominal injuries.
AIS 3+ pelvic injuries were present in 43% of the cases. Injuries to the pubis from contact with the lower side interior were most common.
The complexity of injuries in fixed object impacts suggests that countermeasures need to address brain injuries in addition to a multitude of chest/abdominal and pelvic injuries. Impacts with narrow objects induce more extensive intrusion than observed in vehicle-to-vehicle crashes, and they frequently present an intruding surface that impacts the head.
Near-Side Impact Vehicle-To-Vehicle Collisions
The remainder of the discussion will focus on a filtered data set which includes only near-side occupants in a vehicle to vehicle collision. Although Malliaris (1992) has reported that side collisions with fixed objects are the most injurious collision type, the frequency of vehicle-to- vehicle side impacts and the recent influx of light trucks (including the sport utility vehicles) and vans warrants an in-depth analysis of injury patterns in this subset.
In the discussion to follow, the criteria for study includes near-side occupants in vehicle-to-vehicle side impacts with occupant compartment damage, and without subsequent vehicle rollover or occupant ejection. The WLIRC database contains 46 cases that meet the study criteria. This type of crash comprises approximately 50% of the occupants in the WLIRC database who were injured in side crashes. Four cases with near-side occupants did not have damage to the occupant compartment and were excluded from the study.
Table 2 shows a further comparison of WLIRC and NASS/CDS side impact characteristics. It is evident from the comparison of delta-V and vehicle crush that the WLIRC cases contain fewer low severity crashes, fewer 90 degree impacts and more angular PDOF impacts than those in NASS. Additionally, there are more large cars as struck vehicles and more light trucks and vans (LTV) as striking vehicles compared to NASS.
Table 2.
MAIS 3+ Injured Occupants in Near Side Vehicle-to-Vehicle Crashes
| Delta-V, m/s | WLIRC | NASS |
| 0–9 | 39% | 64% |
| 9–11 | 37% | 19% |
| 11+ | 24% | 16% |
| Crush, m | WLIRC | NASS |
| 0–0.3 | 9% | 15% |
| 0.3–0.6 | 59% | 71% |
| 0.6+ | 33% | 14% |
| Age | WLIRC | NASS |
| 0–15 | 2% | 4% |
| 16–45 | 59% | 53% |
| 46–65 | 17% | 17% |
| 66+ | 22% | 27% |
| Struck Veh. | WLIRC | NASS |
| Sm Car | 37% | 42% |
| Med Car | 37% | 48% |
| Lg Car | 22% | 4% |
| Lt Truck | 4% | 6% |
| Striking Veh. | WLIRC | NASS |
| Car | 52% | 49% |
| LTV | 46% | 37% |
| Hv Truck | 2% | 13% |
The distribution of AIS 3+ injured occupants by most seriously injured body region is displayed in Table 3. Both data sets show that chest injuries are the most frequent, followed by head injuries. The WLIRC data shows a higher frequency of abdominal injuries and a lower frequency of pelvic injuries than shown in the NASS/CDS data. The frequency of abdominal injuries observed in the WLIRC data is consistent with that reported by Fildes (1990). Fildes analyzed Australian side impact injuries and found the most frequent body regions injured at the AIS 2+ level were the chest 47%, abdomen 30%, and the head 17%.
Table 3.
MAIS 3+ Injured Occupants in Near-side Vehicle-to-Vehicle Crashes
| Body Region | WLIRC | NASS |
|---|---|---|
| Head/Face | 20% | 24% |
| Chest | 48% | 44% |
| Abdomen | 20% | 5% |
| Pelvic/LX | 7% | 14% |
| Spine/Neck | 4% | 4% |
| Other | 2% | 9% |
The distribution of serious injuries by body region can be examined in numerous ways. One is by enumerating all injuries suffered by all occupants, AIS 3 and greater. The distribution of injuries counted in this way is shown in the column in Table 4 with the heading ‘AIS 3+ All’. In this study, multiple injuries to the same body organ or skeletal structure are combined and assigned a single value - the highest AIS.
Table 4.
Injuries in WLIRC Crashes that Meet the Study Criteria
| Body Region | AIS 3+ All | MAIS 3+ Worst | MAIS 4+ Fatal |
|---|---|---|---|
| Head | 17% | 17% | 21% |
| Chest | 43% | 50% | 61% |
| Abdomen | 16% | 20% | 15% |
| Pelvic/LX | 19% | 7% | 3% |
| Spine | 3% | 4% | |
| Other | 2% | 2% |
In an alternative accounting, only the most severe injury (MAIS) to each occupant counted. In the event multiple injuries of maximum severity occur, the hierarchical order for selecting the body region for the most severe injury is: brain, chest/abdominal region, and pelvic/lower extremity. This is the accounting system used in Table 3.
In examining fatally injured occupants in side impact, it was observed that AIS 5+ injuries frequently occurred to more than one body organ. Failure to account for all these life threatening injuries distorts the frequency of brain injuries relative to life threatening chest and abdominal injuries. In Table 4, the most serious AIS 3+ injury and all AIS 4+ injuries are grouped under the heading ‘MAIS 3+ Worst’. A similar accounting is used for the distribution of most serious injuries for the fatally injured occupants. This distribution is shown in the column of Table 4 with the heading ‘MAIS 4+ Fatal’. A small change in the MAIS 3+ injury distribution between Tables 3 and 4 is due to the difference in classifying the ‘worst’ injury.
The WLIRC database contains a much higher concentration of severe injuries and fatalities than the NASS/CDS database. Many of the WLIRC vehicle-to-vehicle, near-side crashes involve severe occupant compartment damage. Among the 46 cases, there are 26 fatalities – a very high percentage. However, only two of these fatalities were at crash severities so great that there were no cases of equivalent severity with survivors as well. There was a survivor with a lateral delta-V of 13.9 m/s and 0.89 meters of crush. The three most severe crashes with fatalities had maximum crush values of 0.84, 0.97 and 1 meters.
A comparison of the fatally injured cases and the seriously but non-fatally injured cases is shown in Table 5. As may be expected, the fatal cases have higher mean values for delta-V, maximum crush, and occupant age. For fatally injured occupants, small cars were most frequently the struck vehicle and least frequently the striking vehicle. Light trucks were most frequently the striking vehicle and least frequently the struck vehicle. Light trucks were striking vehicles in 53% of the fatally injured cases.
Table 5.
Fatal, Non-Fatal and Total Injured Meeting the Study Criteria, WLIRC Database
| Injury Outcome | |||
|---|---|---|---|
| Non Fatal | Fatal | Total | |
| Number Of Cases | 20 | 26 | 46 |
| Crush, m | |||
| 0–0.5 | 24% | 17% | 41% |
| 0.5–0.65 | 11% | 17% | 28% |
| 0.65+ | 9% | 22% | 30% |
| Delta-V, m/s | |||
| 0–9 | 24% | 15% | 39% |
| 9–11 | 15% | 22% | 37% |
| 11+ | 4% | 20% | 24% |
| Occupant Age | |||
| 0–15 | 0% | 2% | 2% |
| 16–45 | 28% | 30% | 59% |
| 46–65 | 7% | 11% | 17% |
| 66+ | 9% | 13% | 22% |
| No. of AIS 3+ per Occupant | |||
| 0–1 | 17% | 2% | 20% |
| 2–5 | 24% | 37% | 61% |
| 6+ | 2% | 17% | 20% |
| Direction of Force, (Clock Position) | |||
| 1&11 | 4% | 7% | 11% |
| 2&10 | 37% | 39% | 76% |
| 3&9 | 2% | 9% | 11% |
| 4&8 | 0% | 2% | 2% |
| Struck Vehicle | |||
| Sm Car | 13% | 24% | 37% |
| Med Car | 17% | 20% | 37% |
| Lg Car | 11% | 11% | 22% |
| Lt Truck | 2% | 2% | 4% |
| Striking Vehicle | |||
| Sm Car | 13% | 2% | 15% |
| Med Car | 9% | 11% | 20% |
| Lg Car | 7% | 11% | 17% |
| Lt Truck | 15% | 30% | 46% |
| Lg Truck | 0% | 2% | 2% |
It is interesting to note the large number of AIS-3+ injuries suffered by occupants in the side impact crashes. Eighty percent suffered more than one AIS 3+ injury. About 20 percent suffered six or more AIS 3+ injuries.
In examining the WLIRC database, a vast difference between the fatally injured and the injured survivors exists. There were 26 fatalities among the 46 cases in the study. These 56% of the cases sustained 76% of the AIS 3+ injuries. For the injured survivors there was an average of 2.1 AIS 3+ injuries per occupant. For the fatally injured the average was 5 AIS 3+ injuries per occupant. The fatally injured were generally sustained severe injuries to a number of body components and body regions.
A further distribution of injuries by injured organ or skeletal structure is shown in Table 6. The most frequently injured body components are the ribs, lung, and brain. However, when considering only the most serious injuries, the aorta, heart, and spleen increase in frequency. Among the fatalities, the body components most frequently appearing with severe injuries are: aorta, brain, heart, and ribs. In all fatal cases with rib injuries, there were also internal chest or abdominal organ injuries that contributed substantially to the cause of death. In the WLIRC database there were six occupants with AIS 3+ heart injuries, all fatal. Eleven of the twelve occupants with AIS 3+ thoracic aortic injuries died. In seven of these cases, the aortic injury was the principal cause of death. There were 22 occupants with brain injuries of AIS 3+. In four of these cases, the brain injury was the principal cause of death.
Table 6.
Injuries in WLIRC Cases that Meet the Study Criteria
| Organ | AIS 3+ | MAIS 3+ | Fatal 4+ |
|---|---|---|---|
| Skull | 4% | ||
| Brain | 13% | 17% | 21% |
| Aorta | 8% | 15% | 21% |
| Rib | 16% | 19% | 18% |
| Lung | 13% | 4% | 3% |
| Heart | 4% | 11% | 18% |
| Diap. | 2% | 2% | |
| Liver | 6% | 6% | 3% |
| Spleen | 7% | 11% | 12% |
| Bladder | 2% | 4% | |
| Intest. | 2% | ||
| Pubic | 11% | 6% | |
| Pelvis | 5% | ||
| LowX | 3% | 2% | |
| Neck/Spine | 3% | 3% | 3% |
| Other | 2% | ||
| Number | 170 | 53 | 33 |
THE MOST SERIOUS INJURED BODY ORGANS
As shown in Table 6, the ‘Fatal AIS 4+’ column indicates that aorta, brain, heart, and spleen injuries are the most frequent among fatally injured occupants. A further assessment of these injury modes is presented in this section.
In the NASS/CDS database, brain injuries are the source of 23% of the AIS 6 injuries for crashes that meet the criteria for this study. In the WLIRC data there are 21 occupants with AIS 3+ brain injuries. The crash factors maximum vehicle crush and principal direction of force for the cases are summarized in Table 7. Two of the 21 occupants had brain injuries from two different sources. Forty-three percent of the occupants were restrained, 38% were older than 55, and 52% were female. The maximum crush ranged from 0.25 to 1 meters, with an average of 0.61 meters. Inside the vehicle, the B-pillar and the lower side interior (including window frame and sill) were most frequently contacted to cause the injury. Overall, the most frequent source of head injury was the striking vehicle (35%). In 6 of 8 cases, the striking vehicle that impacted the head was a light truck or van. Existing triage criteria was able to identify all cases in which brain injury was the most serious of all injuries.
Table 7.
Crash Factors for AIS 3+ Brain, Heart, Spleen and Aortic Injuries
| Brain | Heart | Aorta | Spleen | |
|---|---|---|---|---|
| Number AIS 3+ Max Crush, m | 21 | 6 | 13 | 11 |
| 0–0.3 | 10% | |||
| 0.3–0.6 | 52% | 33% | 39% | 64% |
| 0.6+ | 38% | 67% | 61% | 36% |
| Crash Direction | ||||
| 1 & 11 | 24% | 8% | 18% | |
| 2 & 10 | 67% | 83% | 77% | 81% |
| 3 & 9 | 10% | 8% | ||
| 4 & 8 | 17% | 8% | ||
In the NASS/CDS database, heart injuries are the source of 12% of the AIS 6 injuries for crashes that meet the criteria for this study. In the WLIRC database there are six occupants with heart injuries, all fatal. Five of the six died at the scene. The characteristics of the cases are summarized in Table 7. Eighty-three percent of the occupants were restrained, 67% were older than 55, and 67% were female. For heart injuries, the maximum crush ranged from 0.45 to 1 meters, with an average of 0.71 meters. In all six cases, the impacting vehicle struck the side of the case vehicle at an angle. In all five of the driver cases, the injuring contact was the lower side interior (door). The average door intrusion was 0.51 meters and the average lateral delta-V was 11.9 m/s. The combination of high delta-V, angular direction of force and extensive door intrusion were common characteristics of crashes with heart injuries.
In the passenger case with serious heart injury, the seat belt was the source of the injury. In this case, the striking vehicle impacted the B-pillar with a longitudinal delta-V of 10.7 m/s, causing the belt anchor to move rearward and tightening the belt across the passenger’s chest. All occupants with heart injuries were either dead on scene or met existing triage criteria.
In the NASS/CDS database, spleen injuries are the source of 17% of the AIS 5 injuries, but negligible AIS 6 injuries in crashes that meet the criteria for this study. Spleen injuries were the second most frequent AIS 3+ serious chest/abdominal injury in the WLIRC database used for this study. There were eleven AIS 3+ spleen injuries, ten of which were AIS 4+. Sixty-three percent of the occupants were restrained, 27.3% were older than 55, and 45.5% were female. The average crush was 0.58 meters, the average door intrusion was 0.37 meters, and the average lateral delta-V was 11.2 m/s. The lower side interior was the contact causing 81.8% of the spleen injuries, and other occupants contributed to the remainder. Two of the 11 occupants with AIS 3+ spleen injuries did not meet trauma criteria at the scene. These injuries were identified by the high suspicion criteria and injuries were subsequently diagnosed and successfully treated.
For the population the NASS/CDS occupants that meet the study criteria, approximately 40% of the AIS 6 injuries are coded as arterial injuries caused by contact with the lower side interior. This is the largest source of AIS 6 injuries from side impact in the NASS/CDS. In the WLIRC database, there are 13 cases with arterial injuries. One of these cases was in the abdominal region. Twelve of these arterial injuries were to the isthmus of the descending thoracic aorta, just below the subclavian junction. These 12 aortic injuries contributed 21% of the most serious injuries among the fatal cases in the study. AIS 4+ aortic injuries were present in 46% of the fatally injured occupants. The characteristics of the WLIRC aortic injury cases are summarized in Table 7. In all cases, the contact causing the injury was the lower side interior. Fifty percent of the occupants were restrained, 50% were older than 55, and 75% were female. The predominate PDOF was 10’oclock for occupants on the left side and 2 o’clock for occupants on the right side. The average value of the maximum side crush for the twelve vehicles was 0.56 meters.
CHARACTERISTICS OF AORTIC INJURIES
The injuries to the descending aorta constitute a substantial fraction of injury harm in both fatal and non-fatal cases. These injuries are difficult to detect and an undetected descending aortic injury may result in fatality. The 12 cases with injuries to the descending thoracic aorta are summarized in Tables 8a and 8b. All the struck vehicles were passenger cars. In some cases, a second impact occurred after the primary side impact. However, these secondary impacts were generally minor and did not contribute to the aortic injury.
Table 8a.
Cases in the WLIRC Database with Aortic Injuries – Crash Factors
| Crash No. | Case Car | Bullet Vehicle | Occup. Location | Rest. | DOF | DVX m/s | DVY m/s | Max. Crush | Door Intrusion | Meets 214 |
|---|---|---|---|---|---|---|---|---|---|---|
| 96-008S | Lg | Lg Car | Driver | L&S | 10 | 2.2 | 6.3 | 0.33 | 0.20 | No |
| 97-029S | Md | LTV | Driver | None | 10 | 3.6 | 9.4 | 0.41 | 0.28 | No |
| 97-003S | Lg | Lg Car | Driver | None | 10 | 6.7 | 7.6 | 0.51 | 0.25 | No |
| 97-024S | Md | LTV | Driver | None | 10 | 5.4 | 9.4 | 0.48 | 0.36 | No |
| 97-032S | Md | Md Car | RFP | None | 2 | 4.0 | 6.7 | 0.56 | 0.18 | No |
| 97-040BL | Md | Lg Bus | Driver | L&S | 10 | 7.6 | 13.4 | 0.46 | 0.38 | No |
| 98-010SP | Md | Md Car | RRP | None | 11 | 9.4 | 10.7 | 0.66 | 0.30 | No |
| 97-031S | Md | Md Car | RRP | None | 2 | 5.8 | 9.8 | 0.84 | 0.53 | No |
| 97-005S | Md | Lg Car | Driver | L&S | 8 | 5.4 | 11.2 | 0.61 | 0.53 | Yes |
| 96-004S | Md | LTV | Driver | L&S | 9 | 2.7 | 15.2 | 0.61 | 0.43 | No |
| 97-039BL | Sm | LTV | RFP | S | 2 | 8.9 | 15.2 | 0.69 | 0.46 | No |
| 97-006S | Sm | LTV | Driver | S | 10 | 5.8 | 9.8 | 0.76 | 0.61 | No |
Table 8b.
Cases in the WLIRC Database with Aortic Injuries – Injury Factors
| Crash Nr. | Age | Sex | Other Occup | Induced Injury | Aorta AIS | Rib AIS | Next Harmful | Trauma Criteria | Minutes To Death |
|---|---|---|---|---|---|---|---|---|---|
| 96-008S | 62 | M | No | N/A | 6 | 5 | Lung-4 | HS | 106 |
| 97-029S | 77 | F | UnR | Liver-2 | 6 | 5 | Lung-4 | Transfer | 265 |
| 97-003S | 49 | F | No | N/A | 5 | 4 | Leg-1 | Transfer | Survived |
| 97-024S | 27 | M | UnR | Rib-3 | 6 | 3 | Lung-3 | GCS | 140 |
| 97-032S | 74 | F | UnR | Rib-5 | 5 | 5 | Liver-4 | SBP | 4.5 days |
| 97-040BL | 77 | F | No | N/A* | 4 | 4 | Heart-6 | DOS | DOS |
| 98-010SP | 25 | F | UnR | Rib-1 | 6 | 1 | Lung-3 | DOS | DOS |
| 97-031S | 17 | F | UnR | Intest-3 | 4 | 0 | Spleen-5 | SBP | 160 |
| 97-005S | 57 | F | No | N/A | 5 | 5 | Heart-6 | SBP | 47 |
| 96-004S | 51 | M | No | N/A | 5 | 3 | Brain-6 | GCS | 39 |
| 97-039BL | 20 | F | S | N/A | 6 | 4 | Spleen-5 | DOS | DOS |
| 97-006S | 81 | F | No | N/A | 5 | 5 | Heart-6 | DOS | DOS |
AIS 3 brain injury from impact with 2nd vehicle
In Table 8a, ‘Case Car’ indicates the weight struck car (Sm=small, Md=medium, and Lg=large) and ‘Bullet Vehicle’ indicates the size and class of the striking vehicle. The restraint used by the injured occupant is designated by lap and shoulder belt (L&S) and shoulder belt only (S). The DOF is the clock direction of force for the struck vehicle, with 12 o’clock being straight ahead. ‘DVX’ and ‘DVY’ are the calculated change in longitudinal (X) and latitudinal (Y) velocity of the struck vehicle in m/s. The ‘Max Crush’ is the maximum deformation of the struck vehicle side, measured in meters. The ‘Door Intrusion’ is the maximum intrusion of the door adjacent to the injured occupant, measured in meters. Many of the cars on the road were constructed prior to the present side impact test requirements of crash test required by Federal Motor Vehicle Safety Standard 214. The column ‘Meets 214’ indicates whether or not the impacted vehicle was constructed to meet the standard.
Table 8b shows some of the occupant and injury factors associated with the aortic injuries. In 50% of the cases, there was another occupant in the vehicle that may have contributed to the injuries of the subject occupant. The column ‘Other Occup’ indicates the absence of another occupant (No) or, if present, the restraint in use by the other occupant (UnR=unrestrained; S=shoulder belt only). The loading of the subject occupant by an unrestrained occupant contributes to the injuries in a complex manner. Injuries that were identified as being induced by the other occupant are listed in the ‘Induced Injury’ column, along with the AIS of the injury. The AIS rating for the aortic, rib, and other harmful injuries are listed in Table 8b. The trauma triage criteria applied at the crash scene is listed in the column ‘Trauma Criteria’. The following definitions apply to the abbreviations in the column: HS – High suspicion of injury; Transfer – Inter-hospital transfer; GCS – Glasgow Coma Scale (brain function); SBP – Systolic blood pressure; and DOS- Dead on scene.
As shown in Table 8a, the struck vehicles were predominately mid-size cars (67%). The striking vehicles were predominately large cars or light trucks/vans (67%). In one case, a school bus was the impacting vehicle. Drivers were the most frequently involved (67%). However, 2 right rear passengers were involved – a high number in view of the low occupancy of the rear seat. Half of the subjects were unrestrained. The most frequent impact direction was 10 or 2 o’clock (75%). The average lateral delta-V for the cases was 10.3 m/s, the average maximum crush was 0.56 meters, and the average door intrusion was 0.38 meters.
Fifty percent of the subjects were over 55 and 75% were female. Other occupants in the vehicle who were unrestrained contributed to the injuries in 42% of the cases under study. Bilateral AIS 3+ rib fractures accompanied the aortic injuries in 83% of the cases. However, in two of the younger subjects, there were either AIS 1 or no rib injuries.
The aortic injury was the most serious injury in 7 of the 12 cases. Heart injuries were more serious in three of the cases. Brain injuries and spleen injuries were more serious in one case each. Four of the occupants died at the scene from heart and/or aortic ruptures. Severe heart and brain injuries contributed to the death within 60 minutes in two other cases. However, in 6 of 12 cases with aortic injury, the injured occupant survived for more than two hours. In 3 of 12 cases, the survivor did not meet trauma criteria at the scene, although their aortic injuries were subsequently classified as AIS 5 or AIS 6.
The aortagram for case 97-003 is shown in Figure 1. A clot formed on the descending aorta, preventing a catastrophic loss of blood, and limiting the drop in blood pressure. If an aortic injury is not rapidly diagnosed and treated, the risk of death is extremely high. The injury in this case was diagnosed in the Emergency Department and the patient immediately went to surgery for repair. The patient recovered from the aortic injury without significant impairment.
Figure 1.
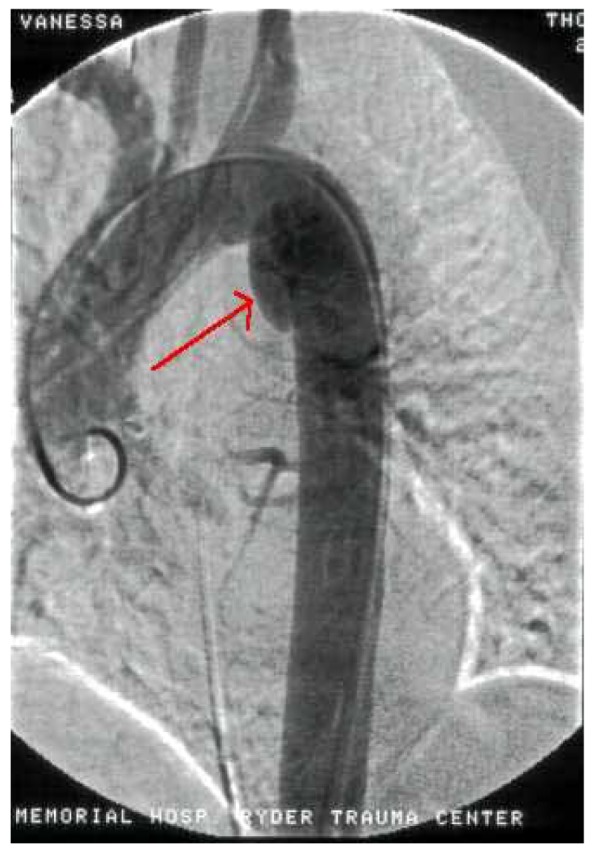
Aortagram from Case 97-003S
Viano (1983) described a range of aortic injuries involving partial tears to the vessel wall, typically the intimal and medial layer. In these cases, the intact adventitia and surrounding plura may limit blood loss. This passive condition is sensitive to a secondary rupture that may occur within weeks of the initial injury. The difficulty in identifying the presence of passive aortic injuries and the potential fatal consequence of these injuries increases the importance of developing criteria from the crash scene to predict these injuries.
The last five cases listed in Table 8 are extremely severe crashes and involve serious injuries other than aortic injuries. The remaining seven cases have the lowest extent of door intrusion, but share three factors in common. The first factor is the obliqueness of the crash. The PDOF was 10 or 11 o’clock for driver-side impacts, and 2 o’clock for passenger side impacts. Second, in all these cases the initial impact occurred in the vicinity of the front wheels, but extended to the location of the occupant. Third, the door adjacent to the injured occupant was displaced inward at the window sill more than at the lower door sill. Figure 2 shows the damage pattern that is typical of the seven cases. These vehicles all have direct impact damage in the region of the front wheels, as well as damage to the injured occupant’s door. In all of the cases, the location of the maximum crush for the door adjacent to the injured occupant was high on the side of the window, close to the window sill.
Figure 2.

Case 96-008S Vehicle Showing Typical Side Damage Pattern for Aortic Injury
DISCUSSION
The purpose of this study was to identify representative injuries and common crash characteristics in side impact collisions. A review of the literature and analysis of the data in NASS/CDS and the William Lehman Injury Research Center database support the concept that 4 primary crash characteristics significantly affect the location and severity of occupant injuries. These are collision type, occupant exposure, impact location, and crash direction.
In this analysis, a combination of these factors placed occupants at high risk of serious/fatal chest and abdominal injuries. Many of these are not easily identified at the scene of the crash but may be survivable if suspected and appropriately managed both on-scene and in the emergency or trauma department.
The findings presented here suggest that occupants in a small to mid-size passenger vehicles who are seated near the struck side in a vehicle-to-vehicle collision with a crash direction of 2 or 10 o’clock are at high risk for life threatening head, chest and abdominal organ injuries. Approximately 90% of all cases fitting this pattern also had passenger compartment intrusion.
Crash Characteristics
In all three data sets, the most frequent crash mode for the injured occupants is the vehicle-to-vehicle crash. Crashes with other vehicles comprised approximately 75% of the cases. Near-side crashes with fixed objects constitute approximately 25% of the AIS 3+ injured occupants in NASS/CDS. The WLIRC database contains 22% fixed object impacts in which near-side occupants were injured.
The injured occupants are most frequently seated on the struck side of the vehicle and the vehicle is damaged in the location of the seated occupant. Near-side occupants made up 66% of the cases in NASS and 70% in the WLIRC. In NASS/CDS vehicle-to-vehicle side crashes with MAIS 3+ injuries, passenger cars are the struck vehicle in over 90% of the cases. In 46% of the cases with MAIS 3+ injuries, the striking vehicle is a light or heavy truck. Crashes with occupant compartment damage are responsible for 95% of the MAIS 3+ injured occupants. Less than 15% of the MAIS 3+ injured occupants are in vehicles with extensive side damage. Occupants seated on the struck side of the vehicle comprise 65% of the MAIS 3+ injured.
Injury Location and Severity
The WLIRC data is consistent with NASS/CDS in terms of the most commonly injured body regions being the chest and head. The WLIRC data shows a higher percentage of injuries occurring in the abdomen (20%) when compared to NASS/CDS (5%). The most serious injuries and fatalities documented in the WLIRC are distributed between brain, heart, spleen and aorta.
Brain injuries occur as the most severe injury in 21 near-side vehicle-to-vehicle crashes. Overall, the most frequent source of brain injury was the striking vehicle (35%). In 6 of 8 cases, the striking vehicle that impacted the head was a light truck (including sports utility vehicles) or van. Inside the vehicle, the B-pillar and the lower side interior (including window frame and sill) were most frequently impacted to cause the injury.
Heart injuries were present in 6 of the WLIRC cases. All were severe crashes (lateral delta-V in excess of 13.4 m/s or vehicle side crush in excess of 0.61 meters) and all had fatal outcomes. Five of the six were dead on-scene, and the one on-scene survivor met exiting triage criteria.
Spleen injuries are the second most frequent AIS 3+ chest/abdominal organ injury among the WLIRC cases that meet the study criteria. There were eleven AIS 3+ spleen injuries, ten of which were AIS 4+. The average crush was 0.58 meters and the source of injury was attributed to lower side interior in 81.8% of cases.
The WLIRC data contains 12 cases of injury to the descending thoracic aorta, 11 of which were fatal. It is of note, however, that 8 of the 12 initially survived the crash and were transported to a hospital while still alive. All of the aortic injuries occurred at the isthmus of the descending thoracic aorta. The injury location was similar for the eight drivers and four passengers with the injury. In seven aortic injury cases with the least door intrusion, several similarities were observed regarding the damage patterns. The characteristics were: (1) an oblique principal direction of force relative to the struck vehicle, (2) direct damage to the struck vehicle beginning at the front wheels, and (3) damage on the door at a high vertical level, often with limited door sill intrusion.
For the WLIRC cases that met the criteria for the study, the existing triage criteria adequately identified brain and heart injuries at the scene when these injuries were the most severe injury. The existing triage criteria identified all survivors with AIS 4+ spleen injuries, but not AIS 3 injuries. Additional criteria to predict this injury is desirable, but is not evident from the present data. The aortic injury is a particularly critical injury requiring early detection and treatment. In the WLIRC data, 92% of the occupants with this injury died but 50% survived for at least 90 minutes. Development of additional crash scene triage criteria could be vital to assist in the early identification of these difficult to detect, time-critical aortic injuries.
In summary, it appears that in the subset of near side vehicle-to-vehicle collisions identified as high risk, the injury distribution pattern is fairly consistent in terms of location and severity. For those cases where the injury is not readily identifiable at the scene of a crash, the use of the 4 high risk crash characteristics (near-side, 10 or 2 o’clock PDOF, passenger compartment intrusion, vehicle-to-vehicle) may prove beneficial as an aide to emergency rescue personnel in assessing high suspicion of injury. If used as ‘symptoms’ of potentially life threatening injuries, it may assist them in the early identification of occult injuries such as aortic tears, which are survivable in occupants arriving alive at a trauma center. Research to refine predictive algorithms will continue.
Several factors will likely affect the injury distribution and severity of future side impact crash victims. First, the majority of occupants studied were enrolled prior to the implementation of the Federal Motor Vehicle Safety Standard 214. The side impact collision standards contained within FMVSS 214 became required in 1997 for passenger vehicles and in 1998 for light trucks. The fleet of vehicles has yet to become broad enough to provide data on the efficacy of the new standards in affording near-side occupants greater protection in side collisions. Similarly, the use of side air bags in higher end vehicles may reduce the severity of head, chest and pelvic injuries, yet remains to be tested due to the scarcity of such vehicles in the general population. Secondly, more Americans are purchasing sports utility vehicles as the primary family car. The issue being, of course, the growing disparity between size, height and weight of these vehicles in comparison to small and mid-sized cars often driven by teenagers or young adults. An increase in severe brain injury from external contacts with the striking vehicle is likely to become more apparent in the future. Development of crash scene triage criteria could be vital to assist in the early identification of these difficult to detect, time-critical aortic injuries.
ACKNOWLEDGEMENTS
The authors would like to express appreciation to the United States Department of Transportation National Highway Traffic Safety Administration and the American Automobile Manufacturers Association for sponsoring this research.
Special thanks to the Office of the Dade County Medical Examiner physicians and staff, to Captain Brian Anderson and the entire Miami-Dade Fire Rescue Department as well as to Sergeant Gary King and all of the officers of the Miami-Dade Police Department Traffic Homicide Division for their unwavering assistance, participation, support and commitment to the WLIRC Crash Study.
REFERENCES
- Dalmotas D. Mechanisms of Injury to Vehicle Occupants Restrained by Three-Point Seat Belts. Proceedings of 24th Stapp Conference; 1980. pp. 441–476. SAE 801311. [Google Scholar]
- Dalmotas D. Injury Mechanisms to Occupants Restrained by Three-Point Seat Belts in Side Impacts. 1983 SAE, 830462. [Google Scholar]
- Fildes B, Vulcan P. Crash Performance and Occupant Safety in Passenger Cars Involved in Side Impacts. Proceedings of IRCOBI; 1990. pp. 121–140. [Google Scholar]
- Hackney J, Gabler H, Kanianthra J, Cohen D. Update of the NHTSA Research activity in thoracic Side Impact Protection for the Front Seat Occupant. 29th Stapp Conference; 1987. pp. 129–142. SAE 872207. [Google Scholar]
- Morris A, Hassan A, Mackay M, Hill J. Head Injuries in Lateral Impact Collisions. Proceedings of IRCOBI; 1993. pp. 41–55. [DOI] [PubMed] [Google Scholar]
- Otte D, Suren E, Appel H, Nehmzow J. Vehicle Parts Causing Injuries to Front Seat Car Passengers in Lateral Impact. Proceedings of the 28th Stapp Car Crash Conference; 1984. pp. 13–26. SAE 841651. [Google Scholar]
- Jones I. Injury Severity vs Crash Severity for Front Seat Car Occupants Involved in Front and Side Crashes. Proceedings of 26th AAAM Conference; 1982. [Google Scholar]
- Malliaris A. G. W. University Report. Apr, 1993. Vehicle Narrow Object Crashes in Highway Travel. [Google Scholar]
- Rouhana S, Foster M. Lateral Impact – An Analysis of the Statistics in the NCSS. Proceedings of 29th Stapp Car Crash Conference; 1985. pp. 79–99. SAE 851727. [Google Scholar]
- Reidelbach W, Zeidler F. What is a Realistic Lateral Impact Test. 1983 SAE830460. [Google Scholar]
- Viano D. Biomechanics of Nonpenetration Aortic Trauma: A Review. Proceedings of 27th Stapp Car Crash Conference; 1983. pp. 190–112. SAE 831608. [Google Scholar]
- Viano D, Culver C, Evans L, Frick M, Scott R. Involvement of Older Drivers in Multi-Vehicle Side Impact Crashes. 12th ESV Conference; 1989. pp. 699–705. [Google Scholar]