

Abstract
Functional neurosurgery includes surgery conducted to ablate, augment, or modulate targets that lead to improvement in neurological function or behavior. Surgical approaches for this purpose include destructive lesioning with different mechanical or biologic agents or energy sources, non-destructive electrical modulation, and cellular or chemical augmentation. Our purpose was to review the role of stereotactic radiosurgery used for functional indications and to discuss future applications and potential techniques. Imaging and neurophysiological research will enable surgeons to consider new targets and circuits that may be clinically important. Radiosurgery is one minimal access approach to those targets.
Keywords: Radiosurgery, functional neurosurgery, stereotactic
INTRODUCTION
Functional neurosurgery has been “in development” for decades. Functional surgeries were some of the most commonly performed in the 1940s (behavioral neurosurgery) and 1950s (Parkinson's disease) before their renaissance in the current era of high-resolution imaging. The history of stereotactic radiosurgery goes back almost as far as the history of functional neurosurgery when tools were being developed not only for stereotactic localization but also for lesioning. Leksell initially conceived the idea of closed-skull, single-session irradiation of a precisely defined intracranial target in 1951, only 2 years after the development of his first stereotactic frame. He applied this concept immediately to functional neurosurgery.[24] At a time when functional destruction of normal brain required thermal energy or chemical injection, Leksell crossfired photon or proton radiation beams to achieve his goal.
In those first years, the limitations of imaging were obvious. The procedure would not be totally noninvasive since contrast encephalography was necessary to identify the target. Although the ganglionic portion of the trigeminal nerve could be indirectly located using cisternography, deep brain targets required air or positive contrast ventriculography. Direct visualization of the target for functional radiosurgery required the later development of computed imaging technology (CT). Radiosurgical techniques were used to create brain lesions without neurophysiologic guidance. This was controversial. Lack of neurophysiologic guidance retarded the use of radiosurgery for functional disorders.
What led to the current interest in the use of functional stereotactic radiosurgery? The value of radiosurgery as a “lesion generator” was based on small and large animal studies that defined the critical dose, the volume, and the temporal evolution of the radiosurgical lesion. Subsequently, functional radiosurgery was compared to microsurgical, chemical, and thermal electrode-based techniques to create a lesion. Current anatomic targets include the trigeminal nerve (for facial pain syndromes), the thalamus (for tremor or pain), the cingulate gyrus or anterior internal capsule (for pain or behavioral illness), the hypothalamus (for cancer pain and perhaps for eating disorders), and the hippocampus or other brain targets (for epilepsy).[30,48]
To treat his initial few patients with trigeminal neuralgia, Leksell coupled an orthovoltage X-ray tube to his early generation stereotactic frame.[25] Application of radiosurgery to intraparenchymal brain lesioning would require more sophistication. He began work with physicist Borje Larsson to crossfire proton beams[23] and subsequently tested a modified linear accelerator. His decision to build and then use the first Gamma Knife in 1967 reflected his frustration with particle beam technology which required travel of the patient to a special cyclotron center. His goal was a hospital-based functional radiosurgery tool. As originally designed, the first Gamma Knife had collimator helmets that created discoid shaped lesions that could “section” white matter tracts or brain tissue in a manner similar to a leucotome or other instrument. Subsequent refinements of the Gamma Knife provided more flexibility in the creation of lesions with different sized circular collimators better suited to structural pathologies like tumors or vascular malformations. Robotic delivery, integrated imaging, enhanced software, and greater efficiency emerged.
THE EARLY FOUNDATION
Radiosurgery was clearly ahead of its time. Functional radiosurgery was performed for a limited number of patients with intractable pain related to malignancy,[26,43] movement disorders,[30] psychiatric illness,[27,42] and trigeminal neuralgia.[25] At the same time, percutaneous retrogasserian glycerol rhizotomy was developed in an observation made during the refinement of the Gamma Knife technique for trigeminal neuralgia. Hakänsson and Leksell attempted to localize the trigeminal nerve within its cistern using glycerol mixed with tantalum powder (as a radiopaque marker) placed in advance of radiosurgery. However, after injection of the glycerol, trigeminal neuralgia pain was relieved and a new operation was conceived.
For intractable pain related to malignancy, radiosurgery was used both for hypophysectomy as well as for medial thalamotomy. Steiner and colleagues published an autopsy study of the effects of radiosurgery used for cancer pain in 1980.[43] The dose selected was estimated from prior animal experiments.[2,23,40] Using small 4-mm beams, doses in excess of 150 Gy provided reproducible small volume tissue necrosis in animal models. Much was learned from these initial procedures which stimulated further use of radiosurgical techniques for movement disorders.
Early animal experiments showed consistent lesion creation at doses at or above 150 Gy.[2,40] Trigeminal pain relief occurred usually within 3 weeks after radiosurgery.[43] We performed extensive studies using a rat radiosurgery model. After delivering 200 Gy using a single 4-mm isocenter, we found a consistent relationship for lesion generatio n that substantiated observations from that human study.[17] Doses of 200 Gy were delivered to the rat frontal brain and then the brain was studied at 1, 7, 14, 21, 60, and 90 days after irradiation. Between 1 and 7 days afterward, we noted that the brain appeared normal. At 21 days, a well-circumscribed volume of necrosis was identified within the radiation volume (4 mm diameter). Thus, the clinical observation of pain relief at 21 days noted by Steiner et al. correlated with laboratory findings at the 200 Gy dose.
The ablative radiosurgery lesion appears as a punched-out, circumscribed volume of complete parenchymal necrosis with cavitation. The lesion was surrounded by a 1–3 mm rim that characterizes the steep fall-off in radiation dose. In this zone, blood vessels appear thickened and hyalinized, and often protein extravasation can be identified. Magnetic resonance (MR) imaging demonstrates all of these features after radiosurgical thalamotomy – a sharply defined, contrast-enhanced rim that defines the low-signal lesion (on short TR images) surrounded by a zone of high-signal (on long TR images) brain tissue.[28] Friehs and colleagues found similar effects and recommended single 4-mm isocenter lesions at doses below 160 Gy.[7] In our own work using a sub-human primate model, doses at or above 100 Gy caused reliable necrosis, but the delay to necrosis was longer.[15,17] To identify the effect of increasing volume, we used an 8-mm collimator in a baboon model and found that half of the animals developed an 8-mm-diameter necrotic lesion even at doses as low as 50 Gy and that this lesion was stable.[2,31] Dose, volume, and time are the three key factors that determine the nature of the functional ablative lesion.
Given that the above-mentioned studies were conducted, why is radiosurgery infrequently used as a functional lesion generator? Perhaps it is due to the occasional variation in the lesion volume noted clinically. Dose fall-off outside the target becomes less steep with increasing volume. The risk of perilesional reactive edema beyond the desired target volume becomes problematic.[13] At small volumes (i.e. single 4-mm collimator), the radiosurgery-created lesion appears more consistent.
FUNCTIONAL RADIOSURGERY RELIES ON IMAGING
Since physiological information is excluded from the targeting component of a functional radiosurgery procedure, high-quality stereotactic neuroimaging must be performed. The imaging must be accurate since small volumes are irradiated and this accuracy must be confirmed at each institution.[20] In addition, the imaging must be of sufficient resolution not only to identify the target structure but also to show important regional tissues. Magnetic resonance imaging (MRI) is the preferred imaging tool for functional radiosurgery.[5,18,47] At the same time, selected patients may not be suitable for MRI. CT images at 1.25-mm slice intervals typically provide adequate resolution of the anterior and posterior commissures, or trigeminal nerve for acceptable localization. There is no doubt that further improvements in subcortical imaging using higher field strength magnets will reach clinical practice soon. We think that radiosurgery will play an expanded role in movement disorders with even more confident imaging. At the same time, manufacturers will need to adjust to this more challenging MR environment. Refinements in materials for stereotactic frames using non-metal construction may be necessary.
RADIOSURGICAL THALAMOTOMY
One of the oldest and most established indications for functional neurosurgery is the ventrolateral thalamotomy used to manage Parkinsonian or essential tremor. The ventralis intermedius (VIM) nucleus thalamic target has been accessed by placement of an electrode into the thalamus, physiologic recording and stimulation at the target site, and creation of a lesion or providing electrical stimulation. Radiosurgical thalamotomy by definition avoids placement of the electrode and evaluation of the physiologic response. In radiosurgery, imaging definition alone is used to determine lesion placement. Initially through the use of contrast ventriculography and later with CT imaging, and over the past two decades with stereotactic MRI, thalamotomy using the Gamma Knife has been performed at centers across the world.[5,12,35,36] The issue is not whether radiosurgery can abolish tremor. It is whether better results may be possible with the adjustable features of deep brain stimulation (DBS). However, DBS is not always available for the elderly, those with medical comorbidities, or those on anticoagulation. With an aging population, this patient group is not insignificant.
Surgeons experienced with “open” thalamic surgery began to explore the value of radiosurgery. Ohye performed radiosurgical thalamotomy contralateral to a prior radiofrequency lesion or to enlarge a previously mapped lesion.[12] Duma et al. reported a 5-year experience with 38 thalamotomies using the Gamma Knife and 28-month mean follow-up.[5] Complete tremor abolition was noted in 24%, excellent relief in 26%, good improvement in 29%, and little to no benefit in 21%. The median time to improvement was 2 months, consistent with data from previous animal experiments. They used a dose range of 110–165 Gy with better results at higher doses. Young et al. reported that 88% of 27 patients who had radiosurgical thalamotomy for tremor (120–160 Gy) became tremor free or “nearly” tremor free.[47] Hirato et al. also found tremor suppression after Gamma Knife thalamotomy in a small patient series.[12] Friehs et al. reported an experience of radiosurgical thalamotomy (n=3) and caudatotomy (n=10), with clinical improvement in most patients and no morbidity.[8]
The mean age of 77 years in the initial Pittsburgh radiosurgery report is older than the mean age of 60 years in their DBS series.[21] Eighteen patients (69%) improved both action tremor and writing scores and an additional 6 (23%) patients improved their action tremor scores. Thirteen patients (50%) had either no or only slight intermittent tremor in the affected extremity and 90% had some degree of clinically significant tremor improvement. Overall, the mean Fahn–Tolosa–Marin tremor score improved from 3.8 to 1.7 (P < 0.000015). MRI typically performed 4 months later showed a 4- to 5-mm round, well-circumscribed lesion with peripheral contrast enhancement surrounding a low-signal region [Figure 1]. A localized area of high signal (seen on long relaxation time studies) demonstrated the peripheral neuronal effect. Two patients with complications had different MRI findings. Although the enhancing lesion created in one patient was unexpectedly large, complete resolution was seen on subsequent imaging. This indicated that the response was related to temporary blood brain barrier changes, and not to permanent radiation injury.
Figure 1.
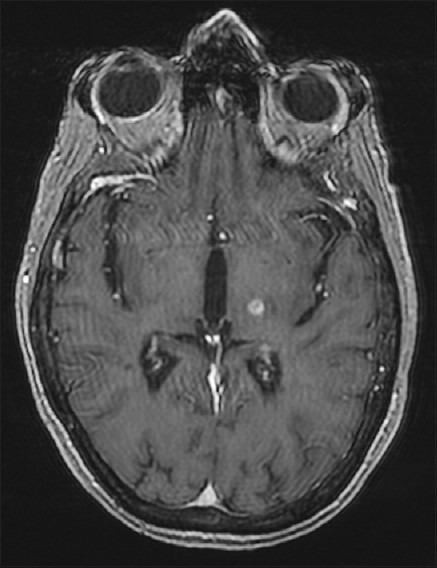
Axial contrast-enhanced MR image 4 months after a left radiosurgical thalamotomy shows the effect at the target site
In a recent overview of our entire radiosurgical thalamotomy experience, 86 patients (88 procedures) underwent gamma knife thalamotomy (GKT) for disabling tremor. Tremor was due to essential tremor (n=48; 19 > age 80 and 3 > 90), Parkinson's disease (29; 11 > age 80), or multiple sclerosis.[11] The median follow-up was 23 months. The mean tremor score was 3.28 ± 0.79 preoperatively and 1.81 ± 1.15 (P < 0.0001) after radiosurgery. The mean handwriting score was 2.78 ± 0.82 before GKT and 1.62 ± 1.04 (P < 0.0001) afterward. The mean drinking score was 3.14 ± 0.78 preoperatively and 1.80 ± 1.15 (P < 0.0001) afterward. After radiosurgery, 57 patients (66%) showed improvement in all three scores, 11 patients (13%) in two scores, two patients (2%) in just one score, and 16 patients (19%) did not show improvement in any of the scores. There were two complications involving temporary hemiparesis.
Thus, the ability to create a small-volume lesion using radiosurgery without placement of a burr hole and the invasive placement of an electrode remains attractive. To that end, several surgeons have evaluated the use of radiosurgery for medial thalamotomy and for pallidotomy, procedures where the usefulness of physiologic recording or stimulation initially was less clear. However, with radiosurgical pallidotomy, we have seen inconsistent lesions perhaps due to the perforating artery supply or mineralization of the pallidum. In addition, the optic tract lies only a few millimeters below the target. There are reports from several centers, but we currently do not perform this procedure.[6,22,37,47]
RADIOSURGERY FOR PAIN
The use of radiosurgery as an ablative tool to treat pain has a long history, but case series are limited. Since the case report by Leksell in 1968 and the larger series by Steiner et al. in 1980, little has been written.[26,43] Young et al. performed medial thalamotomy for the treatment of chronic non-cancer pain in patients who had failed comprehensive medical, surgical, and behavioral therapies.[46] In 1996, they described that two-thirds of their 41-patient series had at least a 50% reduction in pain intensity estimates with improvements in physical and social functioning.[48] As might be expected, patients with deafferentation pain responded poorly, but more encouraging results were identified in patients with nociceptive syndromes.
Hayashi et al. performed pituitary gland-stalk ablation by Gamma Knife radiosurgery, targeting the border between the pituitary stalk and gland with a maximum dose of 160 Gy using the 8-mm collimator to control cancer pain. They enrolled nine patients who had bone metastases and pain controlled well by morphine, Karnofsky performance score (KPS) > 40, and no previous radiation therapy.[9] All patients became pain-free within a few days after radiosurgery, with no later recurrence during their remaining lifespan. In addition, they noted that no patient developed panhypopituitarism and diabetes insipidus. This strategy of pituitary gland–stalk ablation for pain control also showed a good initial response (88%) of 8 patients with thalamic pain syndrome; however, the majority of patients (71%) experienced pain recurrence during the 6-month follow-up.[10]
There is a large amount of literature on the use of stereotactic radiosurgery for trigeminal neuralgia including matched cohort comparisons to other surgical techniques and prospective trials. Over the past 20 years, radiosurgery has become an important option for patients and physicians and we think will continue to play a key management role.
RADIOSURGERY FOR BEHAVIORAL DISORDERS
There are several potential radiosurgery targets to be explored for patients with behavioral disorders. Deep brain stimulation, with the opportunity to conduct testing both on and off stimulation, is a valuable research tool to evaluate specific targets. On the other hand, radiosurgery is an excellent therapeutic tool because it is “always on” and avoids hardware placement or pulse generator failure. Nevertheless, this approach is not often performed but we think will have an expanding future role.
Of greatest current interest is the anterior internal capsule (anterior capsulotomy) in patients with medically refractory obsessive–compulsive disorder (OCD). Radiosurgery for obsessive–compulsive and anxiety neurosis has been performed for over 45 years.[27] The first radiosurgical capsulotomy was performed by Leksell in 1953 using 300 kV X-rays.[29] Initially, pneumoencephalography was used for target definition in the placement of bilateral anterior internal capsule lesions. Five of the initial seven patients had long-term benefit after 7 years of follow-up.[30] Since 1988, an additional 10 patients have been managed in Stockholm and they were recommended use of only 4-mm isocenters.[30] The results seem to be as efficacious as when conventional radiofrequency lesioning is performed.[1] Kihlstrom et al. described the stable imaging appearance of radiosurgical lesions 15-18 years after capsulotomy.[14] Oval-shaped radiosurgical lesions in the anterior internal capsule or cingulate gyrus may impact on affective disorders or anxiety neuroses. In 2008, Ruck et al. reported on long-term follow-up in 25 patients, 16 with an electrode and 9 with Gamma Knife surgery.[41] Response rates did not differ between methods and they concluded that capsulotomy was effective in reducing OCD symptoms.
We perform radiosurgical capsulotomy only after a comprehensive psychiatric evaluation and management regimen leading to a diagnosis of severe or extreme OCD and after failure of non-surgical approaches. In Pittsburgh, we have performed Gamma Knife surgery on four patients with severe, medically intractable OCD and reported on the initial three.[19] According to our protocol, all patients were evaluated by at least two psychiatrists who recommended the capsulotomy procedure. The patient had to request the procedure and should have had severe OCD according to the Yale Brown Obsessive Compulsive Scale (YBOCS). Patients’ ages were 37, 55, and 40, and pre-radiosurgery YBOCS scores were 32/40, 39/40, and 39/40. Bilateral lesions were created with two 4-mm isocenters to create an oval volume in the ventral capsule at the putaminal midpoint. A maximum dose of 140–150 Gy was used. All three patients had significant reductions in their YBOCS score.[19] One patient with compulsive skin picking and an open wound had later healing of their chronic wound.[16] We believe this technique should be evaluated further in patients with severe and disabling behavioral disorders. We are aware of other patients managed in Turkey and Brazil with encouraging results following radiosurgery for OCD.
RADIOSURGERY FOR EPILEPSY
There is clinical and research interest in the use of radiosurgery for patients with focal epilepsy. Focal brain irradiation can lead to amelioration of seizures due to brain tumors, vascular malformations, and other pathologies. The history of this research tells a tale that alternates between human and animal studies. In 1985, Barcia-Salorio et al. reported on six patients with epilepsy who had low-dose radiosurgery (10 Gy). The epileptic focus was localized by means of conventional scalp electroencephalogram (EEG), subarachnoid electrodes, and depth electrodes. In 1994, they provided a long-term analysis in a series of 11 patients using a dose range of 10–20 Gy. Five patients had complete cessation of seizures and an additional five improved. Seizures began to decrease gradually after 3–12 months following radiosurgery.[3] Following this work, Lindquist and colleagues at the Karolinska Institute began to perform epilepsy radiosurgery using advanced localization techniques that included magnetoencephalography (MEG) to define interictal activity.[11,30] In some patients, the epileptic dipole activity identified on MEG before radiosurgery later resolved along with seizure cessation. At the same time, radiosurgery was evaluated in animal models of epilepsy. We used the kainic acid model of hippocampal epilepsy in the rat and were able to stop seizures and improve animal behavior.[32,34] Rats were randomized to control or radiosurgery arms (20, 40, 60, or 100 Gy) and then evaluated with serial EEG, behavioral studies, functional MRI, and histology.
More recently, radiosurgery has been of value in patients with gelastic or generalized seizures related to hypothalamic hamartomas.[33] A larger indication may rest with the use of epilepsy to create an amygdalohippocampal lesion for patients with mesial temporal sclerosis as proposed by Regis et al.[38,39] In 1993, Regis and associates in Marseille performed selective amygdalohippocampal radiosurgery for mesial temporal lobe epilepsy. Gamma Knife radiosurgery was used to create a conformal volume of radiation for the amygdala and hippocampus. This approximate 7-ml volume represented the largest functional target irradiated to that time. They delivered a margin dose of 25 Gy to the 50% isodose line, a dose that later caused target necrosis. The first patient became seizure free immediately and the second after a latency of almost 1 year. Serial MR scans showed target contrast enhancement that corresponded to the 50% isodose line.[38] Patients managed at their center have been part of a multidisciplinary prospective evaluation and treatment protocol. A recently published longer-term evaluation with 8-year mean follow-up (margin dose of 24 Gy) found that 9 of 16 patients were seizure free.[4] An initial prospective multicenter clinical epilepsy radiosurgery trial in the United States was completed that studied mesial temporal lobe epilepsy (MTLE). The optimal target may include both amygdala and hippocampus which is of larger volume than other functional radiosurgery targets. Thus, dose planning and selection must be carefully performed with attention to the dose received by structures such as the brainstem or optic tract. There appears to be similar outcomes when comparing radiosurgery to resection (using available data). As a result, a randomized trial comparing radiosurgery to resection is planned with the primary outcome being non-inferiority of radiosurgery.
Current issues that remain important for epilepsy radiosurgery include dose selection (necrotizing vs. non-necrotizing), localization methods for non-lesional epilepsy, the target volume necessary for irradiation, and the expected short- and long-term outcomes. It is not known what kind of tissue effect is required to stop the generation or propagation of seizures. Some groups have used low doses (i.e. 10–20 Gy) where tissue destruction would not be expected. Others have used doses as high as 100 Gy that cause target necrosis and regional brain edema.[44] A typical amygdalohippocampal radiosurgery maximum dose to a volume less than 7.5 ml is 40–50 Gy.
We think that stereotactic radiosurgery will play an increasing role in epilepsy management. There are many patients who are good surgical candidates but choose not to have surgery or are simply not referred for surgery. Radiosurgery may be an attractive option for them. Tools that enhance our ability to identify the seizure focus will increase the utility of radiosurgery.
FUNCTIONAL IMAGING AND RADIOSURGERY
Improvements in functional imaging eventually will impact radiosurgery. Functional MRI to localize cortical function prior to radiosurgery has been evaluated in pilot studies. Pre-radiosurgery localization of specific motor functions, visual and speech areas close to arteriovenous malformations and brain tumors has been used in dose planning.[45] Unfortunately, there are no prospectively collected data on the value of this concept. Advancements in functional imaging may improve the localization of epileptic foci and perhaps even regions of excitation in the basal ganglia. MEG is an exciting tool to identify functional activation. What is needed is more efficient data analysis to allow same day MEG and radiosurgery planning. An ability to identify hyperactivity in deep brain structures would be valuable. With further improvements in neuroimaging and non-invasive physiologic studies, the future will see a significant linkage between functional brain disorders and stereotactic radiosurgery.
Publication of this manuscript has been made possible by an educational grant from
 ELEKTA
ELEKTA
Footnotes
Disclaimer: The authors of this paper have received no outside funding, and have nothing to disclose.
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2012/3/2/3/91604
Contributor Information
Douglas Kondziolka, Email: kondziolkads@upmc.edu.
John C. Flickinger, Email: flickingerjc@upmc.edu.
Ajay Niranjan, Email: niranjana@upmc.edu.
L. Dade Lunsford, Email: lunsfordld@upmc.edu.
REFERENCES
- 1.Alexander E, Lindquist C. Special indications: Radiosurgery for functional neurosurgery and epilepsy. In: Alexander E, Loeffler JS, Lunsford LD, editors. Stereotactic Radiosurgery. New York: McGraw-Hill; 1993. pp. 221–5. [Google Scholar]
- 2.Andersson B, Larsson B, Leksell L, Mair W, Rexed B, Sourander P, et al. Histopathology of late local radiolesions in the goat brain. Acta Radiologica. 1970;9:385–94. doi: 10.3109/02841867009129115. [DOI] [PubMed] [Google Scholar]
- 3.Barcia-Salorio JL, Barcia JA, Hernandez G, Lopez Gomez L. Radiosurgery of epilepsy.Long-Term results. Acta Neurochir (suppl) 1994;62:111–3. doi: 10.1007/978-3-7091-9371-6_23. [DOI] [PubMed] [Google Scholar]
- 4.Bartolomei F, Hayashi M, Tamura M, Rey M, Fischer C, Chauvel P, et al. Long-term efficacy of gamma knife radiosurgery in mesial temporal lobe epilepsy. Neurology. 2008;70:1658–63. doi: 10.1212/01.wnl.0000294326.05118.d8. [DOI] [PubMed] [Google Scholar]
- 5.Duma CM, Jacques DB, Kopyov OV, Mark RJ, Copcutt B, Farokhi HK. Gamma Knife radiosurgery for thalamotomy in Parkinsonian tremor: A five-year experience. J Neurosurg. 1998;88:1044–9. doi: 10.3171/jns.1998.88.6.1044. [DOI] [PubMed] [Google Scholar]
- 6.Friedman JH, Epstein M, Sanes JN, Lieberman P, Cullen K, Lindquist C, et al. Gamma Knife pallidotomy in advanced Parkinson's disease. Ann Neurol. 1996;39:535–8. doi: 10.1002/ana.410390416. [DOI] [PubMed] [Google Scholar]
- 7.Friehs GM, Noren G, Ohye C, Duma CM, Mark R, Plombon J, et al. Lesion size following Gamma Knife treatment for functional disorders. Stereotact Funct Neurosurg. 1996;66(suppl 1):320–8. doi: 10.1159/000099731. [DOI] [PubMed] [Google Scholar]
- 8.Friehs G, Ojakangas CL, Pachatz P, Schrottner O, Ott E, Pendl G. Thalamotomy and caudatomy with the Gamma Knife as a treatment for Parkinsonism with a comment on lesion sizes. Stereotact Funct Neurosurg. 1995;64(suppl 1):209–21. doi: 10.1159/000098781. [DOI] [PubMed] [Google Scholar]
- 9.Hayashi M, Taira T, Chernov M, Fukuoka S, Liscak R, Yu CP, et al. Gamma Knife surgery for cancer pain-pituitary gland-stalk ablation: a multicenter prospective protocol since 2002. J Neurosurg. 2002;97:433–7. doi: 10.3171/jns.2002.97.supplement. [DOI] [PubMed] [Google Scholar]
- 10.Hayashi M, Taira T, Chernov M, Izawa M, Liscak R, Yu CP, et al. Role of pituitary radiosurgery for the management of intractable pain and potential future applications. Stereotact Funct Neurosurg. 2003;81:75–83. doi: 10.1159/000075108. [DOI] [PubMed] [Google Scholar]
- 11.Hellstrand DE, Abraham-Fuchs K, Jernberg B, Kihlstrom L, Knutsson E, Lindquist C, et al. MEG localization of interictal epileptic focal activity and concomitant stereotactic radiosurgery. A non-invasive approach for patient with focal epilepsy. Physiol Meas. 1993;14:131–6. doi: 10.1088/0967-3334/14/2/004. [DOI] [PubMed] [Google Scholar]
- 12.Hirato M, Ohye C, Shibazaki T, Nakamura M, Inoue HK, Andou Y. Gamma Knife thalamotomy for the treatment of functional disorders. Stereotact Funct Neurosurg. 1995;64(suppl 1):164–71. doi: 10.1159/000098776. [DOI] [PubMed] [Google Scholar]
- 13.Kihlstrom L, Guo WY, Lindquist C, Mindus P. Radiobiology of radiosurgery for refractory anxiety disorders. Neurosurgery. 1995;36:294–302. doi: 10.1227/00006123-199502000-00008. [DOI] [PubMed] [Google Scholar]
- 14.Kihlstrom L, Hindmarsh T, Lax I, Lippitz B, Mindus P, Lindquist C. Radiosurgical lesions in the normal human brain 17 years after Gamma Knife capsulotomy. Neurosurgery. 1997;41:396–402. doi: 10.1097/00006123-199708000-00011. [DOI] [PubMed] [Google Scholar]
- 15.Kondziolka D, Linskey ME, Lunsford LD. Animal models in radiosurgery. In: Alexander E, Loeffler JS, Lunsford LD, editors. Stereotactic Radiosurgery. New York: McGraw-Hill; 1993. pp. 51–64. [Google Scholar]
- 16.Kondziolka D, Hudak R. Management of obsessive-compulsive disorder-related skin picking with gamma knife radiosurgical anterior capsulotomies: A case report. J Clin Psychiatry. 2008;69:1337–40. doi: 10.4088/jcp.v69n0819c. [DOI] [PubMed] [Google Scholar]
- 17.Kondziolka D, Lunsford LD, Claassen D, Maitz A, Flickinger J. Radiobiology of radiosurgery.Part I: The normal rat brain model. Neurosurgery. 1992;31:271–9. doi: 10.1227/00006123-199208000-00012. [DOI] [PubMed] [Google Scholar]
- 18.Kondziolka D, Lunsford LD, Flickinger JC, Young R, Vermeulen S, Duma C, et al. Stereotactic radiosurgery for trigeminal neuralgia: A multi-institution study using the gamma unit. J Neurosurg. 1996;84:940–5. doi: 10.3171/jns.1996.84.6.0940. [DOI] [PubMed] [Google Scholar]
- 19.Kondziolka D, Hudak R, Flickinger JC. Results following gamma knife radiosurgical anterior capsulotomies for obsessive compulsive disorder. Neurosurgery. 2011;68:28–33. doi: 10.1227/NEU.0b013e3181fc5c8b. [DOI] [PubMed] [Google Scholar]
- 20.Kondziolka D, Dempsey PK, Lunsford LD, Kestle J, Dolan E, Kanal E, et al. A comparison between magnetic resonance imaging and computed tomography for stereotactic coordinate determination. Neurosurgery. 1992;30:402–7. doi: 10.1227/00006123-199203000-00015. [DOI] [PubMed] [Google Scholar]
- 21.Kondziolka D, Ong J, Lee JY, Moore R, Flickinger J, Lunsford LD. Gamma knife thalamotomy for essential tremor. J Neurosurg. 2008;108:111–7. doi: 10.3171/JNS/2008/108/01/0111. [DOI] [PubMed] [Google Scholar]
- 22.Kwon Y, Whang CJ. Stereotactic Gamma Knife radiosurgery for the treatment of dystonia.2. Stereotact Funct Neurosurg. 1995;64(suppl 1):222–7. doi: 10.1159/000098782. [DOI] [PubMed] [Google Scholar]
- 23.Larsson B, Leksell L, Rexed B, Surander P, Mair W, Andersson B. The high-energy proton beam as a neurosurgical tool. Nature. 1958;182:1222–3. doi: 10.1038/1821222a0. [DOI] [PubMed] [Google Scholar]
- 24.Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. 1951;102:316–9. [PubMed] [Google Scholar]
- 25.Leksell L. Stereotaxic radiosurgery in trigeminal neuralgia. Acta Chir Scand. 1971;137:311–4. [PubMed] [Google Scholar]
- 26.Leksell L. Cerebral radiosurgery I.Gammathalamotomy in two cases of intractable pain. Acta Chir Scand. 1968;134:585–95. [PubMed] [Google Scholar]
- 27.Leksell L, Backlund EO. In: Stereotactic gammacapsulotomy. In: Modern Concepts in Psychiatric surgery. Hitchcock ER, Ballantine HT, Meyerson BA, editors. Amsterdam: Elsevier; 1979. pp. 213–6. [Google Scholar]
- 28.Leksell L, Herner T, Leksell D, Persson B, Lindquist C. Visualization of stereotactic radiolesions by nuclear magnetic resonance. J Neurol Neurosurg Psych. 1985;48:19–20. doi: 10.1136/jnnp.48.1.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Leksell L, Herner T, Liden K. Stereotaxic radiosurgery of the brain. Report of a case. Kungl Fysiogr Sallsk Lund Forhandl. 1955;25:1–10. [Google Scholar]
- 30.Lindquist C, Kihlstrom L, Hellstrand DE. Functional Neurosurgery-A future for the Gamma Knife? Stereotact Funct Neurosurg. 1991;57:72–81. doi: 10.1159/000099557. [DOI] [PubMed] [Google Scholar]
- 31.Lunsford LD, Altschuler EM, Flickinger JC, Wu A, Martinez AJ. In vivo biological effects of stereotactic radiosurgery: A primate model. Neurosurgery. 1990;27:373–82. doi: 10.1097/00006123-199009000-00006. [DOI] [PubMed] [Google Scholar]
- 32.Maesawa S, Kondziolka D, Dixon E, Balzer J, Fellows W, Lunsford LD. Subnecrotic stereotactic radiosurgery controlling epilepsy produced by kainic acid injection in rats. J Neurosurg. 2000;93:1033–40. doi: 10.3171/jns.2000.93.6.1033. [DOI] [PubMed] [Google Scholar]
- 33.Mathieu D, Kondziolka D, Niranjan A, Lunsford LD, Flickinger JC. Gamma knife radiosurgery for epilepsy caused by hypothalamic hamartomas. Stereotact Funct Neurosurg. 2006;84:82–7. doi: 10.1159/000094036. [DOI] [PubMed] [Google Scholar]
- 34.Mori Y, Kondziolka D, Balzer J, Fellows W, Flickinger JC, Lunsford LD, et al. Effects of stereotactic radiosurgery on an animal model of hippocampal epilepsy. Neurosurgery. 2000;46:157–68. [PubMed] [Google Scholar]
- 35.Otsuki T, Jokura H, Takahashi K, Ishikawa S, Yoshimoto T, Kimura M, et al. Stereotactic gamma-thalamotomy with a computerized brain atlas: Technical case report. Neurosurgery. 1994;35:764–8. doi: 10.1227/00006123-199410000-00029. [DOI] [PubMed] [Google Scholar]
- 36.Pan L, Dai J, Wang BJ, Xu W, Zhou L, Chen XR. Stereotactic gamma thalamotomy for the treatment of Parkinsonism. Stereotact Funct Neurosurg. 1996;66(suppl 1):329–32. doi: 10.1159/000099732. [DOI] [PubMed] [Google Scholar]
- 37.Rand RW, Jacques DB, Melbye RW, Copcutt B, Fisher M, Levenick M. Gamma Knife thalamotomy and pallidotomy in patients with movement disorders: Preliminary results. Stereotact Funct Neurosurg. 1993;61(suppl):65–92. doi: 10.1159/000100662. [DOI] [PubMed] [Google Scholar]
- 38.Régis J, Peragut JC, Rey M, Samson Y, Levrier O, Porcheron D, et al. First selective amygdalohippocampal radiosurgery for mesial temporal lobe epilepsy. Stereotact Funct Neurosurg. 1995;64(Suppl 1):193–201. doi: 10.1159/000098779. [DOI] [PubMed] [Google Scholar]
- 39.Regis J, Rey M, Bartolomei F, Vladyka V, Liscak R, Schrottner O, et al. Gamma knife surgery in mesial temporal lobe epilepsy: A prospective multicenter study. Epilepsia. 2004;45:504–15. doi: 10.1111/j.0013-9580.2004.07903.x. [DOI] [PubMed] [Google Scholar]
- 40.Rexed B, Mair W, Sourander P, Larsson B, Leksell L. Effect of high energy protons on the brain of the rabbit. Acta Radiologica. 1960;53:289–99. doi: 10.3109/00016926009172547. [DOI] [PubMed] [Google Scholar]
- 41.Ruck C, Karlsson A, Steele JD, Edman G, Meyerson B, Ericson K, et al. Capsulotomy for obsessive-compulsive disorder.Long-term follow-up of 25 patients. Arch Gen Psych. 2008;65:914–22. doi: 10.1001/archpsyc.65.8.914. [DOI] [PubMed] [Google Scholar]
- 42.Rylander G. Stereotactic radiosurgery in anxiety and obsessive-compulsive states: Psychiatric aspects. In: Hitchcock ER, Ballantine HT, Meyerson BA, editors. Modern Concepts in Psychiatric Surgery. Amsterdam: Elsevier; 1979. pp. 235–40. [Google Scholar]
- 43.Steiner L, Forster D, Leksell L, Meyerson B, Boethius J. Gammathalamotomy in intractable pain. Acta Neurochir. 1980;52:173–84. doi: 10.1007/BF01402072. [DOI] [PubMed] [Google Scholar]
- 44.Whang CJ, Kim CJ. Short-term follow-up of stereotactic Gamma Knife radiosurgery in epilepsy. Stereotact Funct Neurosurg. 1995;64(suppl 1):202–8. doi: 10.1159/000098780. [DOI] [PubMed] [Google Scholar]
- 45.Witt TC, Kondziolka D, Baumann S, Noll D, Small S, Lunsford LD. Pre-operative cortical localization with functional MRI for use in stereotactic radiosurgery. Stereotact Funct Neurosurg. 1996;66:24–9. doi: 10.1159/000099663. [DOI] [PubMed] [Google Scholar]
- 46.Young RF, Jacques DB, Rand RW, Copcutt B. Medial thalamotomy with the Leksell Gamma Knife for treatment of chronic pain. Acta Neurochir (suppl) 1994;62:105–10. doi: 10.1007/978-3-7091-9371-6_22. [DOI] [PubMed] [Google Scholar]
- 47.Young RF, Shumway-Cook A, Vermeulen S, Grimm P, Blasko J, Posewitz A. Gamma Knife radiosurgery as a lesioning technique in movement disorder surgery. Neurosurg Focus. 1997;2:e11. doi: 10.3171/foc.1997.2.4.12. [DOI] [PubMed] [Google Scholar]
- 48.Young RF, Vermeulen S, Posewitz A, Grimm P, Blasko J, Jacques D, et al. Functional neurosurgery with the Leksell Gamma Knife. Radiosurgery. 1996;1:218–25. [Google Scholar]