

Abstract
Objective
To examine gender differences in inpatient experiences and how they vary by dimensions of care and other patient characteristics.
Data Source
A total of 1,971,632 patients (medical and surgical service lines) discharged from 3,830 hospitals, July 2007–June 2008, and completing the HCAHPS survey.
Study Design
We compare the experiences of male and female inpatients on 10 HCAHPS dimensions using multiple linear regression, adjusting for survey mode and patient mix. Additional models add additional patient characteristics and their interactions with patient gender.
Principal Findings
We find generally less positive experiences for women than men, especially for Communication about Medicines, Discharge Information, and Cleanliness. Gender differences are similar in magnitude to previously reported HCAHPS differences by race/ethnicity. The gender gap is generally larger for older patients and for patients with worse self-reported health status. Gender disparities are largest in for-profit hospitals.
Conclusions
Targeting the experiences of women may be a promising means of improving overall patient experience scores (because women comprise a majority of all inpatients); the experiences of older and sicker women, and those in for-profit hospitals, may merit additional examination.
Keywords: Patient experience, CAHPS, hospitals, gender/sex differences in health and health care
The public reporting of the CAHPS (Consumer Assessment of Healthcare Providers and Systems) Hospital Survey, or HCAHPS survey, has brought new attention to patient experiences with hospital care (Goldstein et al. 2004; Centers for Medicare & Medicaid Services). The financial incentives linked to hospitals' HCAHPS performance under Hospital Value-Based Purchasing under the recently enacted Patient Protection and Affordable Care Act of 2010 (P.L. 111–148; Section 3001) are likely to intensify this attention. More than ever before, hospitals have the means to measure this dimension of their performance and incentives to improve it (Giordano et al. 2002).
There is early evidence that overall HCAHPS quality improvement has begun (Elliott et al. 2009c). In addition to general improvement strategies, hospitals may want to identify subgroups of patients with experiences below the average of all patients at their hospital and target them for particular study and attention, including subgroups defined by service sought or by characteristics of the patient.
While some patient characteristics, such as race/ethnicity, have received relatively much attention (Goldstein et al. 2010), the differences between women and men in their patient experiences has received relatively little attention. This is somewhat surprising, in that women use considerably more health care services than men (Owens 1999), spending more than twice as much as men per capita (Woolhandler and Himmelstein 1997) and constituting a strong majority of hospital patients (including 63 percent of HCAHPS patients; Elliott et al. 2009b). Thus, in addition to direct interest in eliminating any disparities that may exist, study of women's experiences of hospital care has potentially large leverage to both control costs and to improve overall hospital standing on a high-visibility and incentivized measure of performance.
Prior studies that have examined gender differences in patient experiences have primarily examined outpatient experiences but have found few differences by gender (Hall and Dornan 2006; Sitzia and Wood 2003; Buchner and Probst 2009; Zaslavsky et al. 2001; Roohan et al. 2008). When differences have been identified, men have generally reported better experiences with specific aspects of outpatient care, such as getting care quickly (Cleary, Zaslavsky, and Cioffi 1995; Weisman et al. 1997). In Scandinavia, several studies of patient experiences find that female patients are more likely to express dissatisfaction with nursing care (Larsson 2000; Foss 2010b) and staff attitude; male patients' complaints, in contrast, focused more on equipment defects, the doctor, and waiting times.
This is the first national study to examine whether inpatient reports of hospital experiences, as measured by the HCAHPS survey, differ by gender. The very large sample size allows us to detect and explore variation in gender differences by both patient and hospital characteristics. Our analysis is also the first to investigate the extent to which gender differences in overall evaluation of hospital care can be explained by gender differences in emphasis placed upon specific care experiences.
Data and Methods
Data
We analyze HCAHPS survey data collected from 3,830 acute care hospitals for inpatients discharged from July 2007 to June 2008. This study includes approximately 80 percent of U.S. “general acute care” hospitals and virtually all hospitals paid under the Inpatient Prospective Payment System. The HCAHPS survey includes the following eligibility criteria: 18 years or older at the time of admission, at least one overnight stay in the hospital, nonpsychiatric principal diagnosis, and alive at time of discharge. For details on HCAHPS survey administration, see HCAHPS Quality Assurance Guidelines V5.0 (Centers for Medicare & Medicaid Services 2010b).
The survey is conducted between 2 and 42 days after discharge using one of four approved survey modes: mail only, telephone only, mail with telephone follow-up of nonrespondents, and active Interactive Voice Response; scores are adjusted for survey mode and patient mix (also known as case mix) (Elliott et al. 2009a). The patient gender indicator is obtained from hospital administrative records and is missing for 0.5 percent of patients; these patients are excluded from the present analyses. Because the maternity/obstetrics line (19 percent of female cases) is applicable only to women, it was not considered in these analyses. The dataset analyzed includes 1,971,632 completed surveys (1,147,918 or 58 percent female). The average response rate for the hospitals included in this study was 34 percent.
In HCAHPS development, focus groups and cognitive testing employed a balance of men and women to identify gender-specific issues in how experiences were described and items answered.
HCAHPS Survey Measures
The HCAHPS survey produces 10 measures of patients' hospital experience, including six composite measures (Communication with Nurses, Communication with Doctors, Responsiveness of Hospital Staff, Pain Management, Communication about Medicines, and Discharge Information) each composed of two or three individual survey questions. In addition, there are two stand-alone report items (Cleanliness of the Hospital Environment and Quietness of the Hospital Environment) and two global measures (Overall Rating and Recommend the Hospital). See http://www.hcahpsonline.org for the full survey instrument and administration protocols.
The Cleanliness and Quietness items as well as the items comprising five of six composites have a standard set of response options: never, sometimes, usually, and always. The Discharge Information composite employs yes/no response options. Response options are 0–10 for the Overall Rating (with 0 labeled “worst possible” and 10 labeled “best possible”) and definitely no, probably no, probably yes, and definitely yes for the “Recommend to Friends and Family” item. All measures were linearly rescaled to a possible range of 0–100 for comparability and ease of interpretation, so that the transformed score y = 100*(x − a)/(b − a), where original score x was on a scale from a to b.
Analytic Approach
At the sample sizes employed here, the central limit theorem ensures that the assumption that the standard errors of regression coefficients are normally distributed is well satisfied for these CAHPS measures as model outcomes (Zaslavsky et al. 2001).
Because of concerns about the comparability of global ratings and recommendations across demographic groups (Elliott et al. 2010a), primary comparisons of inpatient experiences are restricted to the six composite measures and the two stand-alone report items. Ratings and recommendations are used only as criteria to infer the relative importance of the specific aspects of care assessed by composites and stand-alone report items, as the differences in extreme response tendency that may affect comparisons are less concerning within gender groups.
We begin by estimating a series of eight overall linear regression models of gender differences (one model for each of the six composites and two stand-alone report measures employed here) predicting HCAHPS measures from female indicators and patient-mix adjustors identified in previous research (Elliott et al. 2009a): education, age, self-reported health status, emergency room admission, service line (a surgical indicator, with medical as the reference category), response order, and an age by surgical service line interaction. An additional series of models (results not shown) added hospital fixed effects to these models to estimate within-hospital gender differences.
Next, to assess variation in gender differences for these same eight measures, we estimate a series of eight models that further add fixed effects for race/ethnicity, hospital ownership, and the interactions of age, race/ethnicity, education, self-reported health status, hospital ownership (government-affiliated, private nonprofit, and for-profit) with gender. Government-affiliated hospitals include city, county, and state hospitals, including state university medical centers. These models also included random effects for hospital and female by hospital interaction random effects to capture hospital variation in gender gaps not associated with specific hypothesized factors. Additional analyses (postestimation tests) employ these models to illustrate gender differences at specified values of these covariates.
Finally, to investigate the extent to which gender differences in overall hospital assessments (Rating and Recommend) are affected by gender differences in the relative importance of composite and stand-alone indicators of specific patient experiences, we infer the implicit importance of each composite to overall patient assessments of hospitals in a series of three models following the approach of Elliott et al. (2005). Model 1 regresses overall patient assessment on gender, controlling for mode and patient-mix adjustors. Model 2 adds the six composite measures and two stand-alone report items. Model 3 adds interactions between each composite measure and gender.
Results
Gender Differences in Inpatient Characteristics
As seen in Table 1, the demographic characteristics (age and race/ethnicity) of male and female HCAHPS patients in the medical and surgical lines are similar, with small differences as noted. Emergency room admissions are higher for men (49 percent versus 46 percent for women); male patients are more likely to be in the surgical service line (41 percent versus 38 percent) and more educated, with 22 percent having a 4-year college degree or more (versus 17 percent). Patients with unknown gender, who were excluded from primary analyses, are somewhat more likely to be white, less likely to be admitted through an emergency room, and more likely to be 4-year college graduates, but otherwise they do not differ from the overall sample described in Table 1 (not shown).
Table 1.
Inpatient Demographics by Gender (in %), July 2007–June 2008 Discharges, Excluding Maternity Service Line
| Overall (N = 1,971,632) | Male (N = 823,714) | Female (N = 1,147,918) | |
|---|---|---|---|
| Race/ethnicity*** | |||
| Non-Hispanic white | 79 | 81 | 78 |
| Hispanic | 6 | 6 | 6 |
| African American | 8 | 7 | 9 |
| Asian/Pacific Islander | 2 | 2 | 2 |
| American Indian/Alaska Native | <1 | <1 | <1 |
| Multiracial | 1 | 1 | 1 |
| Unknown | 3 | 3 | 3 |
| Age (years)*** | |||
| 18–34 | 7 | 4 | 8 |
| 35–54 | 20 | 18 | 21 |
| 55–64 | 19 | 21 | 18 |
| 65–74 | 23 | 26 | 21 |
| 75–84 | 22 | 23 | 21 |
| 85+ | 9 | 8 | 10 |
| Non-English primary language*** | 4 | 4† | 4‡ |
| Emergency room admission*** | 47 | 49 | 46 |
| Service line*** | |||
| Surgical | 39 | 41 | 38 |
| Medical | 60 | 59 | 60 |
| Overall health*** | |||
| Excellent | 9 | 9 | 10 |
| Very good | 24 | 25 | 24 |
| Good | 35 | 35 | 34 |
| Fair | 23 | 23 | 23 |
| Poor | 8 | 9 | 8 |
| Education*** | |||
| Grade 8 or less | 7 | 7 | 7 |
| Some high school | 11 | 10 | 11 |
| High school graduate or GED | 35 | 33 | 36 |
| Some college or 2-year degree | 28 | 26 | 29 |
| 4-Year college graduate | 9 | 10 | 9 |
p < .001 compared to males.
Value is 3.76.
Value is 3.87.
Source: HCAHPS data from July 2007–June 2008 hospital discharges, excluding maternity service line.
Average Gender Differences in Inpatient Experiences
Table 2 displays the means for each of the 10 HCAHPS measures by gender, adjusted for mode and patient mix. Women's means were lower for the Overall Rating (−0.7 points, p < .001 for all differences noted in this paragraph) and the Recommend (−1.0 points) measures relative to men's in the same service lines. In general, women also reported less positive experiences of care relative to men, especially for Communication about Medicines (−3.6 points), Discharge Information (−3.0 points), and Cleanliness of the Hospital environment (−3.7 points). The only measure for which women report a more positive experience relative to men is Doctor Communication (+0.6 points). Additional models (results not shown) that added hospital-fixed effects to these models found very similar gender coefficients.
Table 2.
HCAHPS Mean Composite and Stand-Alone Report Scores (SE), Adjusted for Survey Mode and Patient Mix (N = 1,971,632), July 2007–June 2008 Discharges, Excluding Maternity Service Line
| Mean | ||||
|---|---|---|---|---|
| Item | Item Type | Male (n = 823,714) | Female (n = 1,147,918) | Female–Male Difference |
| Overall Rating | Global | 86.2† | 85.6 | −0.6*** |
| Recommendation | Global | 86.6 | 85.6 | −1.0*** |
| Nurse Communication | Composite | 89.0 | 88.3 | −0.7*** |
| Doctor Communication | Composite | 90.5 | 91.1 | 0.6*** |
| Staff Responsiveness | Composite | 82.8 | 81.4 | −1.4*** |
| Pain Management | Composite | 86.3 | 86.0 | −0.3*** |
| Communication about Medicines | Composite | 75.4 | 71.8 | −3.6*** |
| Discharge Information | Composite | 81.1 | 78.1 | −3.0*** |
| Cleanliness | Stand-alone | 87.8 | 84.1 | −3.7*** |
| Quietness | Stand-alone | 79.0 | 78.6 | −0.4*** |
p < .001.
The standard error for all cells in the second and third columns (“male” and “female”) is 0.1.
Variation in Gender Differences in Inpatient Experiences by Patient and Hospital Characteristics
Tables 3 and 4 display gender differences in HCAHPS measures by patient and hospital characteristics. Table 3 shows model coefficients and the statistical significance of interaction terms from the second series of regression models. We first consider the random effects. The female by hospital interaction variance components (measuring unexplained hospital-level variation in gender gaps) are small relative to the hospital variance components, which means that male and female experiences correlate strongly within hospitals. These correlations can be calculated as the square root of the ratio of the hospital variance component to the sum of the hospital and hospital by female variance components. This finding is consistent with an earlier study of the correlation of hospital HCAHPS scores across various patient subgroups (Elliott et al. 2009b). The square roots of these interaction components, which are hospital-level standard deviations of the gender effect or slope, are small-to-moderate relative to the female fixed effects (the average gender gap), so while the size of the gender gap varies a bit from hospital to hospital (even after considering hospital ownership), variation is small enough that male-favoring disparities still exist at most hospitals.
Table 3.
Multivariate Model of HCAHPS Composite and Stand-Alone Measures Predicted by Gender, and Other Patient and Hospital Characteristics, Including Gender Interactions, Adjusted for Survey Mode, Patient-Mix, and Hospital Random Effects (N = 1,971,632)
| Nurse Communication | Doctor Communication | Staff Responsiveness | Pain Management | Communication about Medicines | Discharge Information | Cleanliness | Quietness | |
|---|---|---|---|---|---|---|---|---|
| Female gender | −0.83*** | 0.91*** | −1.69*** | −0.32** | −3.34*** | −1.71*** | −3.70*** | −0.23 |
| Age (years) | ||||||||
| 18–24 | −4.89*** | −5.44*** | −8.45*** | −7.68*** | −1.24*** | −5.20*** | −0.05 | 1.66*** |
| 25–34 | −3.99*** | −4.16*** | −5.56*** | −6.15*** | −1.18*** | −3.20*** | −0.78*** | 1.43*** |
| 35–44 | −2.88*** | −2.51*** | −4.02*** | −4.38*** | −1.25*** | −1.81*** | −0.97*** | −0.76*** |
| 45–54 | −1.43*** | −1.44*** | −1.98*** | −2.44*** | −0.90*** | −0.90*** | −0.51*** | −1.40*** |
| 55–64 (reference) | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| 65–74 | 0.33*** | 0.51*** | 0.47*** | 0.89*** | −0.11 | −0.61*** | 0.35*** | 0.48*** |
| 75–84 | −0.29*** | −0.68*** | −0.32*** | 0.12 | −2.22*** | −2.91*** | 1.60*** | 0.87*** |
| 85+ | −1.74*** | −2.26*** | −2.19*** | −1.43*** | −5.80*** | −4.08*** | 2.85*** | 1.43*** |
| Female×age interaction† | 0.05** | −0.16*** | −0.15*** | −0.17*** | 0.07 | −0.74*** | 0.35*** | −0.16*** |
| Race/ethnicity | ||||||||
| Non-Hispanic white (reference) | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Hispanic | 0.66*** | 1.15*** | 0.78*** | 1.11*** | 2.31*** | 1.25*** | 0.04 | 4.29*** |
| African American | 1.92*** | 1.51*** | 0.67*** | 1.16*** | 3.26*** | −0.37* | 1.86*** | 7.95*** |
| Asian/Pacific Islander | −1.27*** | −0.99*** | −1.87*** | −3.02*** | 0.40 | −0.52 | −2.43*** | 4.27*** |
| American Indian/Alaska Native | −0.33 | −1.15*** | −0.17 | −0.87** | 0.79 | −1.36** | 0.09 | 2.96*** |
| Multiracial | −0.06 | −0.92*** | −0.07 | −1.33*** | 0.01 | −0.90** | 0.72** | 2.14*** |
| Unknown | −2.61*** | −2.79*** | −2.92*** | −3.06*** | −4.25*** | −3.98*** | −2.51*** | −0.06 |
| Female×Hispanic | 0.34** | 0.31** | 0.56*** | 1.15*** | 1.71*** | 0.54* | 0.37* | −0.43* |
| Female×African American | 0.35*** | 0.10 | 0.57*** | 1.20*** | 1.30*** | −0.47* | −0.22 | −0.67*** |
| Female×Asian/Pacific Islander | 0.38 | 0.28 | 0.33 | 1.08*** | 3.16*** | 2.39*** | 1.72*** | −1.51*** |
| Female×American Indian/Alaska Native | −0.87** | −0.27 | −0.75 | −0.25 | −0.50 | 0.34 | −0.87* | −0.78 |
| Female×multiracial | −0.59** | −0.13 | −1.00** | −0.30 | −0.45 | −0.26 | −0.89** | −0.92** |
| Female×unknown | −0.15 | 0.00 | −0.09 | 0.41 | 0.34 | −0.50 | −0.09 | 0.24 |
| Self-rated health‡ | 2.58*** | 2.72*** | 3.31*** | 3.53*** | 4.07*** | 1.92*** | 2.15*** | 2.34*** |
| Female × self-rated health‡ | 0.27*** | 0.16*** | 0.42*** | 0.28*** | 0.04 | 0.36*** | 0.09* | 0.04 |
| Education§ | −0.62*** | −0.53*** | −0.93*** | −0.75*** | −1.66*** | −0.82*** | −0.63*** | −1.73*** |
| Female × education§ | −0.25*** | −0.27*** | −0.31*** | −0.49*** | −0.81*** | −0.64*** | −0.51*** | −0.35*** |
| Hospital ownership | ||||||||
| For-profit (reference) | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| Government | 2.53*** | 1.93*** | 3.45*** | 1.68*** | 4.18*** | 0.46 | 2.64*** | 0.72 |
| Nonprofit | 1.84*** | 0.72*** | 1.37*** | 0.99*** | 2.20*** | 1.20*** | 1.78*** | −2.66*** |
| Female×government | 0.49*** | 0.07 | 0.62*** | 0.39** | 0.60* | 0.08 | 0.58*** | 0.21 |
| Female×nonprofit | 0.27** | −0.09 | 0.68*** | 0.17 | −0.07 | −0.75*** | 0.03 | 0.14 |
| Random effects (variance) | ||||||||
| Hospital variance | 12.58*** | 9.15*** | 31.02*** | 10.61*** | 32.59*** | 31.25*** | 19.64*** | 43.00*** |
| Female×hospital variance | 0.48*** | 0.28*** | 1.69*** | 0.40*** | 1.56*** | 3.30*** | 2.62*** | 1.07*** |
| Residual variance | 306.07*** | 299.11*** | 542.40*** | 389.68*** | 868.32*** | 1061.24*** | 585.97*** | 711.72*** |
p < .001,
p < .01,
p < .05.
Age specified in linear form was recoded so that values ranged from −4 to +3 where −4 = age 18–24, −3 = age 25–34, −2 = age 35–44, −1 = age 45–54, 0 = age 55–64, 1 = age 65–74, 2 = age 75–84, and 3 = age 85+.
Self-rated health was recoded so that values ranged from −2 to +2, where −2 = poor, −1 = fair, 0 = good, 1 = very good, and 2 = excellent.
Education was recoded so that values ranged from −2 to +3 where −2 = 8 grade or less, −1 = some high school, 0 = high school graduate or GED, 1 = some college or 2-year degree, 2 = 4-year college graduate, and 3 = more than 4-year college degree.
Table 4.
Multivariate Female–Male Differences for Specified Demographic Groups, Derived from the Models of Table 3 (N = 1,971,632)
| Nurse Communication | Doctor Communication | Staff Responsiveness | Pain Management | Communication about Medicines | Discharge Information | Cleanliness | Quietness | |
|---|---|---|---|---|---|---|---|---|
| Age 18–24 | −1.05*** | 1.57*** | −1.10*** | 0.36* | −3.62*** | 1.25*** | −5.10*** | 0.41* |
| Age 55–64 (reference) | −0.83*** | 0.91*** | −1.69*** | −0.32** | −3.34*** | −1.71*** | −3.70*** | −0.23 |
| Age 85+ | −0.67*** | 0.42*** | −2.14*** | −0.84*** | −3.13*** | −3.93*** | −2.65*** | −0.71*** |
| Non-Hispanic white (reference) | −0.83*** | 0.91*** | −1.69*** | −0.32** | −3.34*** | −1.71*** | −3.70*** | −0.23 |
| Hispanic | −0.49*** | 1.22*** | −1.13*** | 0.82*** | −1.63*** | −1.17*** | −3.33*** | −0.66*** |
| African American | −0.48*** | 1.01*** | −1.12*** | 0.88*** | −2.04*** | −2.18*** | −3.92*** | −0.90*** |
| Asian/Pacific Islander | −0.45* | 1.20*** | −1.36*** | 0.75* | −0.18 | 0.68 | −1.99*** | −1.73*** |
| American Indian/Alaska Native | −1.71*** | 0.64* | −2.44*** | −0.58 | −3.84*** | −1.37* | −4.57*** | −1.01* |
| Multiracial | −1.42*** | 0.79*** | −2.69*** | −0.62* | −3.79*** | −1.97*** | −4.59*** | −1.15*** |
| Unknown | −0.98*** | 0.92*** | −1.78*** | 0.08 | −3.00*** | −2.21*** | −3.79*** | 0.01 |
| Excellent health | −0.30** | 1.23*** | −0.86*** | 0.24 | −3.27*** | −0.99*** | −3.53*** | −0.15 |
| Good health (reference) | −0.83*** | 0.91*** | −1.69*** | −0.32** | −3.34*** | −1.71*** | −3.70*** | −0.23 |
| Poor health | −1.37*** | 0.59*** | −2.53*** | −0.89*** | −3.41*** | −2.43*** | −3.88*** | −0.31* |
| More than 4-year college degree | −1.58*** | 0.11 | −2.63*** | −1.79*** | −5.77*** | −3.63*** | −5.23*** | −1.27*** |
| High school degree (reference) | −0.83*** | 0.91*** | −1.69*** | −0.32** | −3.34*** | −1.71*** | −3.70*** | −0.23 |
| Grade 8 or less | −0.34*** | 1.45*** | −1.07*** | 0.65*** | −1.72*** | −0.43* | −2.68*** | 0.47** |
| For-profit (reference) | −0.83*** | 0.91*** | −1.69*** | −0.32** | −3.34*** | −1.71*** | −3.70*** | −0.23 |
| Government | −0.34*** | 0.98*** | −1.08*** | 0.06 | −2.74*** | −1.63*** | −3.13*** | −0.02 |
| Nonprofit | −0.56*** | 0.82*** | −1.02*** | −0.16** | −3.41*** | −2.46*** | −3.67*** | −0.09 |
p < .001,
p < .01,
p < .05.
We next turn to fixed effects. Given the presence of interactions with gender, the “female gender” coefficient estimates the female–male difference (or gender gap) in the reference group that is coded “0” on all interaction terms: 55- to 64-year-old non-Hispanic whites in good health with a high school degree, but no college, seen in a for-profit hospital. Table 4 uses these same models to illustrate gender differences at specified covariates values.
With respect to fixed effect interactions of patient and hospital characteristics with female gender, a significant and negative coefficient indicates a larger gender gap in favor of men. The gender gap is less advantageous for older women for five of eight report measures (Table 3). As can be seen in Table 4, three measures exhibit statistically significant crossover interactions of age and gender, which indicates that women ages 18–24 report significantly better experiences than men, while the reverse is true for ages 85 and older.
Of the four largest race/ethnic groups (non-Hispanic white, Hispanic, African American, and API), the gender gap is least favorable for women among non-Hispanic whites for five measures. For some measures, the gender gap is about twice as large for non-Hispanic white women as it is for API, black, and Hispanic women. In contrast, gender gaps for AIAN and multiracial respondents tend to be wider than for non-Hispanic whites. For several measures, the gender gap is about half as large for African Americans, Hispanics, and API as for non-Hispanic whites. Only Quietness shows a distinctly different pattern whereby the gender gap is narrower for non-Hispanic whites than it is for minority groups.
There are notable differences in the size of the gender gap based on self-reported health status, although the direction of the interaction varies across measures. Gender disparities are larger for patients with worse self-reported health for six of eight measures. As can be seen in Table 4, for three measures, gender disparities are small or even nonexistent for patients in excellent health. For Discharge Information, gender disparities are smaller for patients with better health, but they are still marked for even those with excellent health. Gender disparities are consistently largest for the most educated women and smallest, or even reversed, for the least educated.
Gender disparities are less favorable to men in for-profit hospitals than in government-affiliated or nonprofit hospitals fox six of eight measures, with only one instance of being more favorable to women in for-profit hospitals.
Gender Differences in the Emphasis Placed on Specific Patient Experiences in Overall Hospital Evaluations
Table 5 describes gender differences in overall patient assessments of hospitals (Overall Rating and Recommend), and gender differences in the inferred importance of each composite or stand-alone measure of specific patient care experience to patients' overall assessments. Model 1 results show that women provide less positive global evaluations than men, after controlling for survey mode and patient characteristics. Model 2 adds the six composites and two stand-alone HCAHPS measures and assumes that they have the same effect on global evaluations for men and women. Communication with Nurses was the most important measure in predicting global evaluations (for Overall Rating B = 0.359, p < .001; for Recommend B = 0.405, p < .001), while Communication about Medicines, Discharge Information, and Quietness were least important. After adjusting for women's worse-specific experiences (as measured by composites and stand-alone items), female patients provided higher Overall Ratings, but still lower Recommendations, relative to men with similar experiences on the six composite and two stand-alone report items (for Overall Rating B = 0.182, p < .001; for Recommended B = −0.263, p < .001).
Table 5.
Regression Predicting Overall Rating and Recommendation from Gender, Composites and Reports Measures, and the Interactions of Gender with Composite/Report Measures, Adjusted for Survey Mode and Patient-Mix
| Overall Rating | Recommendation | |||||
|---|---|---|---|---|---|---|
| Model 1 | Model 2 | Model 3 | Model 1 | Model 2 | Model 3 | |
| Female | −0.691*** | 0.182*** | −1.964*** | −1.193*** | −0.263*** | −1.811*** |
| Nurse Communication | 0.359*** | 0.338*** | 0.405*** | 0.378*** | ||
| Doctor Communication | 0.107*** | 0.109*** | 0.136*** | 0.142*** | ||
| Staff Responsiveness | 0.106*** | 0.093*** | 0.104*** | 0.090*** | ||
| Pain Management | 0.120*** | 0.126*** | 0.123*** | 0.133*** | ||
| Communication about Medicines | 0.051*** | 0.053*** | 0.050*** | 0.051*** | ||
| Discharge Information | 0.046*** | 0.049*** | 0.058*** | 0.063*** | ||
| Cleanliness | 0.096*** | 0.103*** | 0.102*** | 0.112*** | ||
| Quietness | 0.053*** | 0.050*** | 0.042*** | 0.040*** | ||
| Female × Nurse Communication | 0.031*** | 0.041*** | ||||
| Female × Doctor Communication | −0.002 | −0.009** | ||||
| Female × Staff Responsiveness | 0.021*** | 0.023*** | ||||
| Female × Pain Management | −0.010*** | −0.016*** | ||||
| Female × Communication about Medicines | −0.003* | −0.001 | ||||
| Female × Discharge Information | −0.005*** | −0.008*** | ||||
| Female × Cleanliness | −0.010*** | −0.015*** | ||||
| Female × Quietness | 0.003** | 0.003 | ||||
p < .001,
p < .01,
p < .05.
Model 3 allows the slopes associated with the composite and stand-alone measures to vary by gender. Differences in slope are generally statistically significant but small compared to the main effects of the objective measure; thus, the implicit importance of the composites varies somewhat by gender, but not by much. Women's overall experiences are more strongly associated with Nurse Communication and Staff Responsiveness than are men's, as indicated by the significant and positive interaction of these two items each with female gender. In contrast, women's global assessments of their hospital experiences are less strongly influenced by Pain Management, Discharge Information, and Cleanliness, compared with men, as indicated by the significant and negative interaction terms.
Conclusion
In this study, we examined gender differences in reported hospital experiences. Women reported generally less positive experiences than men on seven of eight measures of specific aspects of their experiences (with exception of Doctor Communication) and on both of overall assessments of experiences. These differences may reflect both differences in patient expectations and in the behavior of hospital staff; Safran et al. (1980) provide evidence that male and female patients behave differently when they present with the same objective symptoms and that physicians behave differently toward male and female patients based on different assumptions regarding gender. When Foss and Hofoss asked patients to describe the most positive aspects of patient care, male patients were more likely to praise “friendly and helpful nurses,” whereas female patients were more likely to express appreciation for being accommodated, which Foss interprets as reflecting in part “the general desire of men to be taken care of and women to be respected” (Foss and Hofoss 2011, p. 278) when in a vulnerable position.
Our findings that women report less positive interactions than men with nurses and nonphysician hospital staff, but better doctor communication, are consistent with several Scandinavian studies (Larsson 2000; Foss 2010b) and suggest a possible role of gender concordance in these interactions. While the HCAHPS survey does not include information about the gender of physicians, nurses, and other staff, future research with supplementary items might examine the extent to which gender concordance in communication dyads might mediate some of the observed findings, including the small tendency for more positive experiences for women than men with doctor communication.
The gender differences seen here were generally similar in magnitude to previously reported racial/ethnic differences in HCAHPS scores (Goldstein et al. 2010). Gender differences within hospitals were very similar to overall gender differences, suggesting that unlike differences in inpatient experience by race/ethnicity (Goldstein et al. 2010), very little of observed differences in inpatient experience by gender are attributable to differences in quality in the hospitals used by men and women.
The largest gender differences were for Cleanliness of the Hospital Environment and two measures of communications regarding posthospitalization care (Communication about New Medicines and Discharge Information). Women's traditional caregiving role may lead to women having higher expectations than men about specific care dimensions that are related to the caregiving role, such as cleanliness. With respect to communication regarding posthospitalization care, prior research suggests that female patients make more requests for information than male patients (Pendleton and Bochner 2005; Hooper et al. 2008). Our findings suggest that female patients' expectations for information about posthospitalization care are not being fully met, and thus the gender gap here persists; recognizing and meeting those expectations may be an important quality improvement opportunity.
The tendency for women to have somewhat worse patient experiences than men was more pronounced for women who were older, less healthy, more educated, non-Hispanic white, or who received care in a for-profit hospital. Our finding that gender differences are generally larger in for-profit hospitals may be due to the less intensive staffing, different hospital staff work conditions, and lower pay for nonphysician staff in for-profit hospitals compared with nonprofit and government hospitals, as reported previously in the literature (Arrington and Haddock ; Kessler and McClellan 1990; Bacon, Hughes, and Mark). Alternatively, recent work in outpatient settings (Elliott et al. 2010a) suggests that managed care forms of Medicare (Medicare Advantage) have bigger gender gaps than those in fee-for-service Medicare. Because a similar pattern was found for other groups whose care, like women's, tends to be more costly (Owens 1999), cost considerations may play a similar role in for-profit hospitals. Future research should examine how additional organizational characteristics may differentially affect the experiences of male and female patients, including staffing levels, and staff characteristics.
Some of the characteristics associated with larger gender gaps may be markers of vulnerability, such as older age and poorer health, and may reflect poorer health care received by vulnerable women relative to vulnerable men. Other characteristics (e.g., greater educational attainment) are not associated with vulnerability (Blumenthal, Mort, and Edwards 1990), but instead may be markers of higher expectations of health care that female patients hold compared to similar male patients (Foss 2010b). Other research (see review in Elliott et al. 2010a) suggests that negative response tendencies may be greatest in these groups, although prior research has not explored gender differences within these groups.
We find that a combination of different inpatient experiences and the value placed on specific hospital experiences, particularly nurse communication, largely explains female patients' lower overall rating of hospitals. This finding is consistent with prior research showing that Communication with Nurses is the strongest predictor of overall assessments (Elliott et al. 2005; Kutney-Lee, 1982). We also find that women place somewhat greater emphasis on communication with hospital staff than men, but less emphasis than men on pain management and cleanliness. Thus, women's poorer experiences with pain management and cleanliness do not appear to greatly influence their overall assessments.
A limitation of this study is that the overall average response rate was 34 percent. Groves, in recent reviews of the survey methodology literature (Groves 2005; Groves and Peytcheva 2010), suggests that among probability samples conducted with a standardized process that adheres to typical process standards of survey methodology, response rates are only weakly associated with nonresponse bias and may not be a strong proxy for nonresponse bias. Consistent with this argument, analyses of early HCAHPS data linked to a richer set of variables than are currently available for nonresponse analyses (Elliott et al. 2000) examined the association of HCAHPS nonresponse with age, gender, race/ethnicity, Spanish language preference, length of stay, admission source, Major Diagnostic Group, and discharge status, and found some evidence of higher nonresponse for younger, male, and minority patients. There was no evidence that the nonresponse weights implied by these logistic regression models reduced nonresponse bias after applying patient-mix adjustment. Later, Elliott et al. (2009a) reached similar conclusions using more recent HCAHPS data with a more limited set of predictors of nonresponse. To date, HCAHPS has not used patient gender as a patient-mix adjustor but has only partially adjusted for gender via adjustment for maternity service line (Elliott et al. 2009a). While we find evidence here that medical and surgical HCAHPS scores vary by patient gender within hospitals, the proportion of females within those service lines varies relatively little between hospitals (O'Malley et al. 2009). Because hospital scores are adjusted substantially only when a candidate adjustor is both predictive within hospitals and varies substantially between hospitals (Zaslavsky et al. 2001), additional adjustment for gender may be unnecessary.
On the other hand, these findings may have implications for quality improvement. Differences between women and men for Communication about New Medicines, Discharge Information, and Cleanliness of the Hospital Environment translate to 0.5–0.7 hospital-level standard deviations. Given that women comprise 63 percent of overall HCAHPS populations (Elliott et al. 2009b), a hospital that closed such a gender gap by bringing the experiences of its female patients on these three dimensions up to those of its male patients would improve its overall rank among hospitals by 4–19 percentile points (e.g., from ranking at the 40th percentile of hospitals to ranking as high as 59th percentile among hospitals). The potential for improvement is greater for hospitals such as for-profit hospitals, where the gender gaps are often somewhat wider than in nonprofit hospitals. Such improvements would have significant impacts on hospital reimbursement, given that these three measures constitute about one-third of the HCAHPS value-based purchasing score, which itself constitutes 30 percent of the overall value-based purchasing score under the Affordable Care Act.
In some cases, efforts might be made to meet what may be different expectations of care for women and men. Improving female patient experience in the medical and surgical service lines, particularly with respect to Communication with Nurses and staff responsiveness, should be a particular priority. Such efforts might focus on nursing and discharge communications and instructing nurses in how to solicit patient questions and feedback during patient interactions. Such improvement would also meaningfully improve hospitals' overall ratings, given that women comprise a majority of inpatients. The care of older and sicker women, and women in for-profit hospitals, bears additional examination and emphasis.
SUPPORTING INFORMATION
Additional supporting information may be found in the online version of this article:
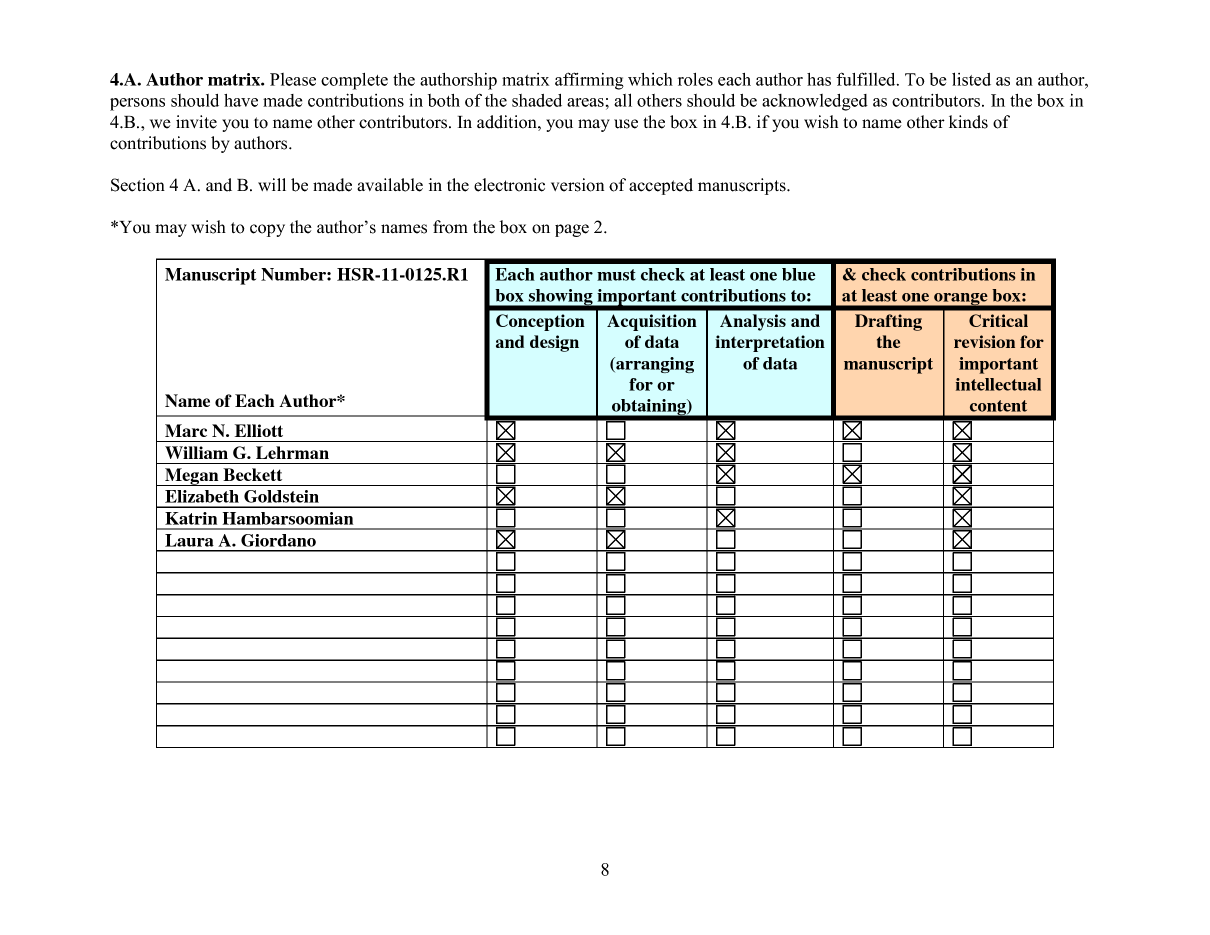
Appendix SA1: Author Matrix
{kind=link}
Please note: Wiley-Blackwell is not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article.
References
- Arrington B, Haddock CC. “Who Really Profits from Not-for-Profits?”. Health Services Research. 1990;25(2):291–304. [PMC free article] [PubMed] [Google Scholar]
- Bacon CT, Hughes LC, Mark BA. “Organizational Influences on Patient Perceptions of Symptom Management”. Research in Nursing and Health. 2009;32(3):321–34. doi: 10.1002/nur.20319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blumenthal D, Mort E, Edwards J. “The Efficacy of Primary Care for Vulnerable Population Groups”. Health Services Research. 1995;30(1 Pt 2):253–73. [PMC free article] [PubMed] [Google Scholar]
- Buchner DA, Probst LY. “The Member Satisfaction Survey as a Measure of Health Plan Accountability”. Quality Management in Health Care. 1999;7(2):41–9. doi: 10.1097/00019514-199907020-00005. [DOI] [PubMed] [Google Scholar]
- Centers for Medicare & Medicaid Services. 2010. “HCAHPS Fact Sheet 2010” [accessed on November 29, 2010]. Available at http://www.hcahpsonline.org/files/HCAHPS%20Fact%20Sheet%202010.pdf. [PubMed]
- Centers for Medicare & Medicaid Services. HCAHPS Quality Assurance Guidelines Version 5.0. Baltimore, MD: Centers for Medicare & Medicaid Services; 2010. [Google Scholar]
- Cleary PD, Zaslavsky AM, Cioffi M. “Sex Differences in Assessments of the Quality of Medicare Managed Care”. Womens Health Issues. 2000;10(2):70–9. doi: 10.1016/s1049-3867(99)00045-6. [DOI] [PubMed] [Google Scholar]
- Elliott MN, Edwards C, Angeles J, Hambarsoomian K, Hays RD. “Patterns of Unit and Item Nonresponse in the CAHPS Hospital Survey”. Health Services Research. 2005;40(6 Pt 2):2096–119. doi: 10.1111/j.1475-6773.2005.00476.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliott MN, Haviland AM, Kanouse DE, Hambarsoomian K, Hays RD. “Adjusting for Subgroup Differences in Extreme Response Tendency in Ratings of Health Care: Impact on Disparity Estimates”. Health Services Research. 2009;44(2 Pt 1):542–61. doi: 10.1111/j.1475-6773.2008.00922.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliott MN, Kanouse DE, Edwards CA, Hilborne LH. “Components of Care Vary in Importance for Overall Patient-Reported Experience by Type of Hospitalization”. Medical Care. 2009;47(8):842–9. doi: 10.1097/MLR.0b013e318197b22a. [DOI] [PubMed] [Google Scholar]
- Elliott MN, Zaslavsky AM, Goldstein E, Lehrman W, Hambarsoomian K, Beckett MK, Giordano L. “Effects of Survey Mode, Patient Mix, and Nonresponse on CAHPS Hospital Survey Scores”. Health Services Research. 2009;44(2 Pt 1):501–18. doi: 10.1111/j.1475-6773.2008.00914.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elliott MN, Lehrman WG, Goldstein E, Hambarsoomian K, Beckett MK, Giordano LA. “Do Hospitals Rank Differently on HCAHPS for Different Patient Subgroups?”. Medical Care Research and Review. 2010;67(1):56–73. doi: 10.1177/1077558709339066. [DOI] [PubMed] [Google Scholar]
- Elliott MN, Lehrman WG, Goldstein EH, Giordano LA, Beckett MK, Cohea CW, Cleary PD. “Hospital Survey Shows Improvements in Patient Experience”. Health Affairs (Millwood) 2010;29(11):2061–7. doi: 10.1377/hlthaff.2009.0876. [DOI] [PubMed] [Google Scholar]
- Elliott MN, Haviland AM, Orr N, Hambarsoomian K, Cleary PD. “How Do the Experiences of Medicare Beneficiary Subgroups Differ between Managed Care and Original Medicare?”. Health Services Research. 2011;46(4):1039–1058. doi: 10.1111/j.1475-6773.2011.01245.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Foss C. “Gender Bias in Nursing Care? Gender-Related Differences in Patient Satisfaction with the Quality of Nursing Care”. Scandinavian Journal of Caring Science. 2002;16(1):19–26. doi: 10.1046/j.1471-6712.2002.00045.x. [DOI] [PubMed] [Google Scholar]
- Foss C, Hofoss D. “Patients' Voices on Satisfaction: Unheeded Women and Maltreated Men?”. Scandinavian Journal of Caring Sciences. 2004;18(3):273–80. doi: 10.1111/j.1471-6712.2004.00290.x. [DOI] [PubMed] [Google Scholar]
- Giordano LA, Elliott MN, Goldstein E, Lehrman WG, Spencer PA. “Development, Implementation and Public Reporting of the HCAHPS Survey”. Medical Care Research and Review. 2010;67(1):27–37. doi: 10.1177/1077558709341065. [DOI] [PubMed] [Google Scholar]
- Goldstein L, Crofton C, Garfinkel S, Darby C. “Why Another Patient Survey Matters”. Health Services Research. 2005;40:1475. doi: 10.1111/j.1475-6773.2005.00477.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Goldstein E, Elliott MN, Lehrman WG, Hambarsoomian K, Giordano LA. “Racial/Ethnic Differences in Patients' Perceptions of Inpatient Care Using the HCAHPS Survey”. Medical Care Research and Review. 2010;67(1):74–92. doi: 10.1177/1077558709341066. [DOI] [PubMed] [Google Scholar]
- Groves RM. “Nonresponse Rates and Nonrespose Bias in Household Surveys”. Public Opinion Quarterly. 2006;70(4):646–75. [Google Scholar]
- Groves RM, Peytcheva E. “The Impact of Nonresponse Rates on Nonresponse Bias: A Meta-Analysis”. Public Opinion Quarterly. 2008;72(2):167–89. [Google Scholar]
- Hall JA, Dornan MC. “Patient Sociodemographic Characteristics as Predictors of Satisfaction with Medical Care: A Meta-Analysis”. Social Science & Medicine. 1990;30(7):811–8. doi: 10.1016/0277-9536(90)90205-7. [DOI] [PubMed] [Google Scholar]
- Hooper EM, Comstock LM, Goodwin JM, Goodwin JS. “Patient Characteristics that Influence Physician Behavior”. Medical Care. 1982;20(6):630–8. doi: 10.1097/00005650-198206000-00009. [DOI] [PubMed] [Google Scholar]
- Kessler DP, McClellan MB. “Is Hospital Competition Socially Wasteful?”. Quarterly Journal of Economics. 2000;115:577–615. [Google Scholar]
- Kutney-Lee A, McHugh MD, Sloane DM, Cimiotti JP, Flynn L, Neff DF, Aiken LH. “Nursing: A Key to Patient Satisfaction”. Health Affairs. 2009;28(4):w669–77. doi: 10.1377/hlthaff.28.4.w669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larsson BW. “Patients' Views on Quality of Care: Age Effects and Identification of Patient Profiles”. Journal of Clinical Nursing. 1999;8(6):693–700. doi: 10.1046/j.1365-2702.1999.00311.x. [DOI] [PubMed] [Google Scholar]
- O'Malley AJ, Zaslavsky AM, Elliott MN, Zaborski L, Cleary PD. “Case-Mix Adjustment of the CAHPS Hospital Survey”. Health Services Research. 2005;40(6 Pt 2):2162–81. doi: 10.1111/j.1475-6773.2005.00470.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Owens GM. “Gender Differences in Health Care Expenditures, Resource Utilization, and Quality of Care”. Journal of Managed Care Pharmacy. 2008;14(3 suppl):2–6. doi: 10.18553/jmcp.2008.14.S6-A.2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pendleton DA, Bochner S. “The Communication of Medical Information in General Practice Consultations as a Function of Patients' Social Class”. Social Science & Medicine. Medical Psychology & Medical Sociology. 1980;14A(6):669–73. doi: 10.1016/0160-7979(80)90072-7. [DOI] [PubMed] [Google Scholar]
- Roohan PJ, Franko SJ, Anarella JP, Dellehunt LK, Gesten FC. “Do Commercial Managed Care Members Rate Their Health Plans Differently Than Medicaid Managed Care Members?”. Health Services Research. 2003;38(4):1121–34. doi: 10.1111/1475-6773.00166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Safran DG, Rogers WH, Tarlov AR, McHorney CA, Ware JE., Jr “Gender Differences in Medical Treatment: The Case of Physician-Prescribed Activity Restrictions”. Social Science and Medicine. 1997;45(5):711–22. doi: 10.1016/s0277-9536(96)00405-4. [DOI] [PubMed] [Google Scholar]
- Sitzia J, Wood N. “Patient Satisfaction: A Review of Issues and Concepts”. Social Science and Medicine. 1997;45(12):1829–43. doi: 10.1016/s0277-9536(97)00128-7. [DOI] [PubMed] [Google Scholar]
- Weisman CS, Henderson JT, Schifrin E, Romans M, Clancy CM. “Gender and Patient Satisfaction in Managed Care Plans: Analysis of the 1999 HEDIS/CAHPS 2.0H Adult Survey”. Womens Health Issues. 2001;11(5):401–15. doi: 10.1016/s1049-3867(01)00093-7. [DOI] [PubMed] [Google Scholar]
- Woolhandler S, Himmelstein DU. “Consumer Directed Healthcare: Except for the Healthy and Wealthy It's Unwise”. Journal of General Internal Medicine. 2007;22(6):879–81. doi: 10.1007/s11606-007-0187-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zaslavsky AM, Zaborski LB, Ding L, Shaul JA, Cioffi MJ, Cleary PD. “Adjusting Performance Measures to Ensure Equitable Plan Comparisons”. Health Care Financing Review. 2001;22(3):109–26. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.