

Abstract
Though primitive neuroectodermal tumor has been considered to arise from a neoplastic transformation of primitive neuroepithelial cells with propensity to involve any part of the central nervous system, a primary intramedullary spinal primitive neuroectodermal tumor is very unusual. The authors describe a case of an 18-year-old female with conus intramedullary tumor diagnosed to be primary spinal primitive neuroectodermal tumor following histopathological examination after surgery. The diagnosis of such a tumor is very crucial as the management strategies for these are relatively unclear and are associated with a poorer outcome compared to the other common intramedullary spinal tumors.
Keywords: Intramedullary, management, primitive neuroectodermal tumor, spinal, tumor
Introduction
Ever since the term primitive neuroectodermal tumor (PNET) has been proposed by Hart and Earle to define a group of malignant neoplasms of presumed neural crest origin, a number of cases of the same have been described at various locations.[1] Primary PNET of the spine is unusual with very few cases reported in the literature.[2–4] Occurrence of primary spinal PNET in an intramedullary location is further uncommon[4]; more so in children. Very few case reports of primary pediatric spinal intramedullary PNET are reported in the literature.[3–10] We describe a case of an 18-year-old female with conus intramedullary tumor diagnosed to be a spinal primary PNET following surgery The diagnosis was not suspected until the same was confirmed following final histopathological examination. The importance of recognizing the same lies in the different management strategy and therapeutic outcome compared to the usual intramedullary spinal tumors for which surgery forms the cornerstone of treatment and are associated with a better clinical outcome compared to spinal PNET.
Case Report
An 18-year-old female presented with complaints of low back ache and weakness involving bilateral lower extremities for 3 months along with bowel bladder involvement for 1 week. Examination revealed tenderness in lower back with hypotonic and paraplegia (0/5 Medical Research Council grade) in bilateral lower limbs. Ninety percent sensory loss to all modalities of sensation was present with no evidence of sacral sparing. Magnetic resonance imaging (MRI) of the spine revealed an intramedullary lesion, predominantly isointense on TIW MRI with homogenous contrast enhancement and interspersed cystic/necrotic areas from D11-L2 [Figures 1 and 2]. A differential diagnosis of common intramedullary tumors namely ependymoma (myxopapillary variant), paraganglioma, other glial neoplasms, metastases or any inflammatory pathology was considered. Laminectomy and tumor decompression was performed. . Histopathology revealed a highly cellular tumor, consisting mainly of small round to oval cells with hyperchromatic nuclei and remarkably scanty cytoplasm along with the presence of Homer-Wright pseudorosettes; the tumor cells being immunopositive for CD 99 [Figure 3]. Bone scan and an intracranial MRI were done which did not reveal any evidence of tumor elsewhere and a diagnosis of primary intramedullary PNET was made. Post-operative course was uneventful with minimal improvement in power and the patient is awaiting adjuvant chemoradiotherapy.
Figure 1.

T1W Magnetic resonance imaging showing a predominantly isointense intramedullary tumor
Figure 2.
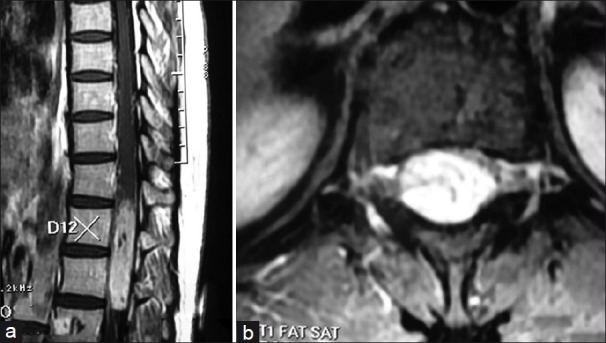
Sagittal (a) and axial (b) contrast enhanced Magnetic resonance imaging showing the homogenously enhancing intramedullary tumor with interspersed cystic/necrotic areas
Figure 3.
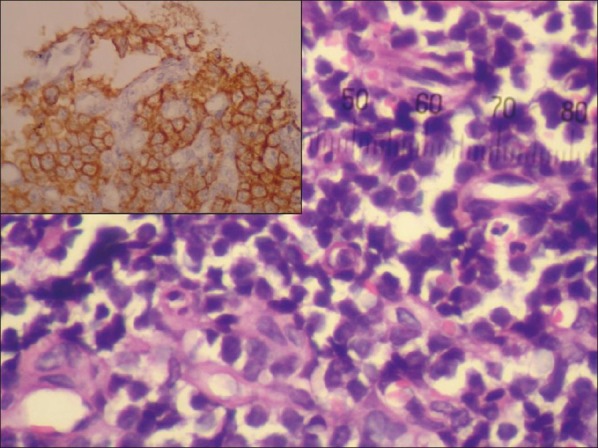
Microphotograph showing a highly cellular tumor, consisting mainly of small round to oval cells with hyperchromatic nuclei and remarkably scanty cytoplasm along with the presence of Homer-Wright pseudorosettes; the tumor cells being immunopositive for CD 99 (inset)
Discussion
PNETs are malignant tumors composed of highly undifferentiated neuroepithelial cells comprising of various lesions that are histologically similar and usually occur in the pediatric age. These are located mainly intracranially with management being surgical excision followed by craniospinal radiotherapy and a radiation boost to the primary tumor with or without chemotherapy. It has been postulated that PNETs arise from neoplastic transformation of primitive neuroepithelial cells in subependymal zones which are present in all areas of the central nervous system and may explain the presence of PNETs at locations other than the cerebellum.[2,11] Due to unknown reasons, primary PNET involving the spine is rare and can be intramedullary, intradural–extramedullary, or epidural, with the majority arising from the cauda equina.[2–4,12–18]
Drop metastasis from primary intracranial tumors disseminating via cerebrospinal fluid accounts for majority of spinal PNET.[2] Primary intraspinal PNETs are rare. Though, these tumors differ from central PNET in their immunohistochemical profile, genetic backgrounds and potential to metastasize outside CNS; the overall prognosis and survival is equally dismal.[2–4] Intramedullary primary PNET can present in both children and adults with no sex predilection across the whole spinal column with preferential involvement of the thoracic region.[3,4] Intramedullary location of a primary PNET is uncommon especially in children,[3–10] where glial neoplasms account for majority of intramedullary tumors. Only eight cases of clearly documented purely intramedullary spinal PNETs have been reported in the pediatric age group.[3–10] Though spinal PNET behaves differently from that of spinal cord astrocytoma or ependymoma, the common tumors at this location, the imaging features does not differentiate between them. This precludes the preoperative diagnosis of spinal PNET which usually is based on the histopathological finding with confirmation by immunohistochemical analysis. However, due to rarity of spinal cord PNET, the possibility of metastasis from a central or peripheral PNET should be ruled out before arriving at the diagnosis of primary spinal PNET as was done in the described case. Magnetic resonance imaging of the whole brain and spine or a FDG PET can be performed to exclude these possibilities.
The management and prognosis of this highly uncommon lesion in this location is different from the more common tumors involving this region and is uniformly poor. In view of the good clinical response to chemoradiation in medulloblastoma or supratentorial PNET the same should be considered even in spinal PNET, not withstanding the fact that complete excision is difficult to achieve in this eloquent location.
To conclude, PNET forms a very unusual differential for intramedullary spinal tumors. Recognition of this entity at this unusual location is important for prognostication and management as these tumors involve multidisciplinary treatment with poor overall outcome compared to other intramedullary tumors of the spinal cord which it can resemble radiologically.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
References
- 1.Crain Barbara J. Wilkins RH, editor. Primitive neuroectodermal tumours. Neurosurgery by Rengachary. 1996;2:1707–13. [Google Scholar]
- 2.Deme S, Ang LC, Skaf G, Rowed DW. Primary intramedullary primitive neuroectodermal tumor of the spinal cord: Case report and review of literature. Neurosurgery. 1997;1:1417–20. doi: 10.1097/00006123-199712000-00040. [DOI] [PubMed] [Google Scholar]
- 3.Kumar R, Reddy SJ, Wani AA, Pal L. Primary spinal primitive neuroectodermal tumor: Case series and review of the literature. Pediatr Neurosurg. 2007;43:1–6. doi: 10.1159/000097517. [DOI] [PubMed] [Google Scholar]
- 4.Otero-Rodríguez A, Hinojosa J, Esparza J, Muñoz MJ, Iglesias S, Rodríguez-Gil Y, et al. Purely intramedullary spinal cord primitive neuroectodermal tumor: Case report and review of the literature. Neurocirugia (Astur) 2009;20:381–6. doi: 10.1016/s1130-1473(09)70159-9. [DOI] [PubMed] [Google Scholar]
- 5.Freyer DR, Hutchinson RJ, McKeever PE. Primary primitive neuroectodermal tumor of the spinal cord associated with neural tube defect. Pediatr Neurosci. 1989;15:181–7. doi: 10.1159/000120466. [DOI] [PubMed] [Google Scholar]
- 6.Ogasawara H, Kiya K, Kurisu K, Muttaqin Z, Uozumi T, Sugiyama K, et al. Intracranial metastasis from a spinal cord primitive neuroectodermal tumor: Case report. Surg Neurol. 1992;37:307–12. doi: 10.1016/0090-3019(92)90158-j. [DOI] [PubMed] [Google Scholar]
- 7.Kwon OK, Wang KC, Kim CJ, Kim IO, Chi JG, Cho BK. Primary intramedullary spinal cord primitive neuroectodermal tumor with intracranial seeding in an infant. Childs Nerv Syst. 1996;12:633–6. doi: 10.1007/BF00261661. [DOI] [PubMed] [Google Scholar]
- 8.Mottl H, Koutecky J. Treatment of spinal cord tumors in children. Med Pediatr Oncol. 1997;29:293–5. doi: 10.1002/(sici)1096-911x(199710)29:4<293::aid-mpo10>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 9.Kampman WA, Kros JM, De Jong TH, Lequin MH. Primitive neuroectodermal tumors (PNETs) located in the spinal canal: The relevance of classification as central or peripheral PNET. J Neurooncol. 2005;15:1–8. doi: 10.1007/s11060-005-9006-z. [DOI] [PubMed] [Google Scholar]
- 10.Kim YW, Jin BH, Kim TS, Cho YE. Primary intraspinal primitive neuroectodermal tumor at conus medullaris. Yonsei Med J. 2004;45:533–8. doi: 10.3349/ymj.2004.45.3.533. [DOI] [PubMed] [Google Scholar]
- 11.Rorke IB. The cerebellar medulloblastoma and its relationship to primitive neuroectodermal tumors. J Neuropath Exp Neurol. 1983;42:1–15. [PubMed] [Google Scholar]
- 12.Aydin MV, Sen O, Ozel S, Kayaselcuk F, Caner H, Altinors N. Primary primitive neuroectodermal tumor within the spinal epidural space: Report of a case and review of the literature. Neurol Res. 2004;26:774–7. doi: 10.1179/016164104225014111. [DOI] [PubMed] [Google Scholar]
- 13.Dorfmuller G, Wurtz FG, Umschaden HW, Kleinert R, Ambros PF. Intraspinal primitive neuroectodermal tumor: Report of two cases and review of the literature. Acta Neurochir (Wien) 1999;141:1169–75. doi: 10.1007/s007010050414. [DOI] [PubMed] [Google Scholar]
- 14.Hisaoka M, Hashimoto H, Murao T. Peripheral primitive neuroectodermal tumor with ganglioneuroma-like areas arising in the cauda equina. Virchows Arch. 1997;431:365–9. doi: 10.1007/s004280050112. [DOI] [PubMed] [Google Scholar]
- 15.Isotalo PA, Agbi C, Davidson B, Girard A, Verma S, Robertson SJ. Primary primitive neuroectodermal tumor of the cauda equina. Hum Pathol. 2000;31:999–1001. doi: 10.1053/hupa.2000.16532. [DOI] [PubMed] [Google Scholar]
- 16.Kepes JJ, Belton K, Roessmann U, Ketcherside WJ. Primitive neuroectodermal tumors of the cauda equina in adults with no detectable primary intracranial neoplasm—three case studies. Clin Neuropathol. 1985;4:1–11. [PubMed] [Google Scholar]
- 17.McDermott VG, El-Jabbour JN, Sellar RJ, Bell J. Primitive neuroectodermal tumor of the cauda equina. Neuroradiology. 1994;36:228–30. doi: 10.1007/BF00588138. [DOI] [PubMed] [Google Scholar]
- 18.Papadatos D, Albrecht S, Mohr G, Carpio-O’Donovan R. Exophytic primitive neuroectodermal tumor of the spinal cord. AJNR Am J Neuroradiol. 1998;19:787–9. [PMC free article] [PubMed] [Google Scholar]