

Abstract
Aim:
The aim of this study was to evaluate the long-term complications and problems related to gastrostomy and jejunostomy feeding tubes used for home enteral nutrition support and the effect these have on health care use.
Materials and Methods:
The medical records of 31 patients having gastrostomy (27 patients) and jejunostomy (4) feeding tubes inserted in our Department were retrospectively studied. All were discharged on long-term (>3 months) enteral nutrition and followed up at regular intervals by a dedicated nurse. Any problem or complication associated with tube feeding as well as the intervention, if any, that occurred, was recorded. Data were collected and analyzed.
Results:
All the patients were followed up for a mean of 17.5 months (4–78). The most frequent tube-related complications included inadvertent removal of the tube (broken tube, plugged tube; 45.1%), tube leakage (6.4%), dermatitis of the stoma (6.4%), and diarrhea (6.4%). There were 92 unscheduled health care contacts, with an average rate of such 2.9 contacts over the mean follow-up time of 17.5 months.
Conclusion:
In patients receiving long-term home enteral nutrition, feeding tube-related complications and problems are frequent and result in significant health care use. Further studies are needed to address their optimal prevention modalities and management.
Keywords: Complications, Gastrostomy, Home enteral nutrition, Jejunostomy
INTRODUCTION
The most common home infusion therapy today is home enteral nutrition (HEN) or tube feeding. HEN should be used in patients who cannot meet their nutrient requirements by oral intake, yet have a functional gastrointestinal tract, and who are able to receive therapy outside of an acute care setting. It is estimated that more than 300,000 people of all ages in the USA are receiving enteral nutrition at home, whereas in Europe, enteral tube feeding in the community has also considerably increased in the last few years. Epidemiologic data from UK show that, at any one time, over 19,500 patients receive enteral tube feeding in the UK community, more than twice that in hospitals.[1]
Several reasons have contributed to the rapid growth of HEN, including increased awareness of therapeutic nutrition, developments in artificial nutrition, higher proportion of elderly people in the population, reduction in the number of hospital beds, as well as promotion and marketing of HEN by commercial companies.
Gastrostomy and/or jejunostomy feeding tubes are frequently inserted and used for long-term home enteral nutrition support. Although insertion of these tubes is usually related to minor morbidity, their long-term use may contribute to various complications and problems which may affect quality of life and have significant economic consequences on health care use. As there are only few studies that address long-term complications related to feeding tubes, the purpose of this study is to examine the long-term complications and problems related to tube malfunction and the effect these have on health care use.
MATERIALS AND METHODS
The medical records of 31 patients having gastrostomy and/or jejunostomy feeding tubes inserted in our department were retrospectively studied; of these, 27 patients had gastrostomy and 4 had jejunostomy tubes. Dysphagia was the most common primary reason for tube insertion commonly as a result of cerebrovascular accident, cancer of the upper gastrointestinal tract, head and neck cancer, and cerebral trauma [Table 1]. The gastrostomy tubes used were made of polyurethane and their diameter ranged between 20 and 22 Fr. These tubes had a “mushroom”-shaped part on the inside of the stomach and a suture holding outside to keep them in place and to avoid sinking into the stomach. Out of the 27 gastrostomy patients, 25 had surgical Stamm gastrostomies and 2 had PEGs performed according to the “push” technique. The jejunostomy tubes used were T-tubes, with a diameter of 14–16 Fr. These tubes were kept in place by a suture on the skin. Enteral tube feeding was initiated in hospital and the patients were subsequently discharged. Prior to the discharge, all patients and caregivers were seen by a physician, nurse, and dietician, and their ability to be trained and perform the tasks associated with HEN, reimbursement for HEN, and the home environment was evaluated. They were also advised regarding their tube-feeding regimen, tube and site care, as well as regarding the potential complications that they may encounter related to their feeding tube. All 31 patients were discharged home on long-term HEN (>3 months), and were followed up once per month by a dedicated nurse for all the time they received HEN. Any problem or complication that occurred associated with tube feeding as well as the intervention, if any, was recorded and referred to our Artificial Nutrition Unit. Data were collected and analyzed.
Table 1.
Reasons for feeding tube insertion in the 31 patients

RESULTS
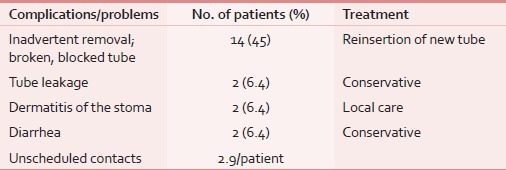
In the study, those patients were included who were followed up after their discharge from the hospital for the entire duration of their HEN, i.e., until their HEN support stopped for any reason, including death. Those who did not meet the previously described HEN discharge criteria and those who were lost to follow-up were excluded. So, a total of 31 patients were finally included in the study. These patients were followed up for a mean of 17.5 months (range 4–78). The most frequent tube-related complications included inadvertent tube removal (broken tube, tube occlusion; 45.1%), tube leakage (6.4%), dermatitis of the stoma (6.4%), and diarrhea (6.4%; Table 2). Tube dysfunction, such as inadvertent removal, broken, blocked, and leaking tube, was the complication requiring the most frequent intervention by a physician or nurse. There were a total of 92 unscheduled health care contacts for many of these tube-related problems and complications, for an average rate of such 2.9 contacts over the mean follow-up time of 17.5 months, resulting in significant economic consequences for the caregivers.
Table 2.
Feeding tube-related complications and treatment in patients receiving long-term home enteral nutrition
DISCUSSION
Despite the overall safety of feeding tubes, a number of complications can occur following their placement which are usually considered as minor including tube dislodgment, peristomal leakage, and wound infection;[2,3] also, most studies have suggested that complications are more likely to occur in elderly patients with comorbid illnesses, particularly those with an infectious process or who have a history of aspiration.[4] Nevertheless, enteral tube feeding is considered “routine” by many health care professionals involved with it, because these tubes are the most common and easiest to manage in the community. However, as tube feeding can still be a daunting thought for patients and caregivers, careful consideration should be given to predischarge planning and training. Planning for discharge on HEN should begin at the earliest opportunity and involve all the relevant health care professionals and community staff,[5] while discussing with the patients and caregivers what to expect on a daily basis when administering HEN.[6] Also, training patients and/or caregivers on caring for the tube, hygiene issues, safety, and basic problem solving is of paramount importance, and they must be clear regarding arrangements for supply of feed and equipment. Consequently, by the time of discharge, patients and caregivers should be adequately trained on the various aspects of the tube feeding system, to ensure safe and effective feeding at home.
Despite that all 31 patients of this study were well trained on all the aspects of the home tube feeding system, our results showed that tube-related complications, although not life threatening, were common and they were associated with increased health care use. Although these patients were followed up once a month by a dedicated nurse, there were 92 unscheduled health care contacts for an average rate of 2.9 contacts per patient over the mean follow-up time of 17.5 months. Similar findings have also been shown by other studies.[7–10]
As tube dysfunction was the most frequent complication related to its presence, some simple measures must be taken to prevent or, at least, to decrease its incidence. For example, tubes may become clogged or occluded if not flushed with water after each feeding, or, feedings may leak around the exit site of the tube if tube is too loose, if the balloon is broken, if the tract is enlarged, or the stomach too full. Consequently, it is required checking the placement of the tube frequently, as well as their resecuring to keep them in place. It is interesting to note that these late complications are common either in surgically placed gastrostomies or in PEGs.
In conclusion, in patients receiving long-term home enteral tube feeding, tube-related complications and problems are common and result in significant health care use. Further studies are needed to assess their exact effect on health care utilization and quality of life of these patients and primary caregivers, as well as to address their optimal prevention modalities and management.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Madigan SM, Fleming P, McCann S, Wright ME, MacAuley D. General Practitioners involvement in enteral tube feeding at home: A qualitative study. BMC Fam Pract. 2007;8:29. doi: 10.1186/1471-2296-8-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Taylor CA, Larson DE, Ballard DJ, Bergstrom LR, Silverstein MD, Zinsmeister AR, et al. Predictors of outcome after percutaneous endoscopic gastrostomy: A community-based study. Mayo Clin Proc. 1992;67:1042–9. doi: 10.1016/s0025-6196(12)61118-5. [DOI] [PubMed] [Google Scholar]
- 3.Larson DE, Burton DD, Schroeder KW, DiMagno EP. Percutaneous endoscopic gastrostomy. Indications, success, complications and mortality in 314 consecutive patients. Gastroenterology. 1987;93:48–52. [PubMed] [Google Scholar]
- 4.Raha SK, Woodhouse K. The use of percutaneous endoscopic gastrostomy (PEG) in 161 consecutive elderly patients. Age Ageing. 1994;23:162–3. doi: 10.1093/ageing/23.2.162. [DOI] [PubMed] [Google Scholar]
- 5.Mensforth A, Spelding D. Discharge planning for home enteral tube feeding. Clin Nutr Update. 1998;3:8–10. [Google Scholar]
- 6.Goff K. Enteral and parenteral nutrition transitioning from hospital to home. Nurs Case Manag. 1998;3:67–74. [PubMed] [Google Scholar]
- 7.Crosby J, Duerksen D. A retrospective survey of tube-related complications in patients receiving long-term home enteral nutrition. Dig Dis Sci. 2005;50:1712–7. doi: 10.1007/s10620-005-2923-z. [DOI] [PubMed] [Google Scholar]
- 8.Carey TS, Hanson L, Garrett JM, Lewis C, Phifer N, Cox CE, Jackman A. Expectations and outcomes of gastric feeding tubes. Am J Med. 2006;119(527):e11–6. doi: 10.1016/j.amjmed.2005.11.021. [DOI] [PubMed] [Google Scholar]
- 9.Crosby J, Duerksen D. A prospective study of tube- and feeding-related complications in patients receiving long-term home enteral nutrition. J Parenter Enteral Nutr. 2007;31:274–7. doi: 10.1177/0148607107031004274. [DOI] [PubMed] [Google Scholar]
- 10.Alivizatos V, Kotsikoris J, Souchlakis M, Zygomalas A, Terzakis P. Feeding tube-related complications in patients receiving long-term home enteral nutrition. Nutr Clin Pract. 2008;23:209. [Google Scholar]