

Abstract
Background:
The evaluation for skin disorders forms an important component of primary health care practice for all including children. The prevalence of certain skin diseases in children can reflect status of health, hygiene, and personal cleanliness of a community.
Aims:
This study was planned to evaluate the magnitude of skin diseases, pattern of various dermatoses, factors contributing to these dermatoses and concurrent systemic disease among children up to five years of age.
Materials and Methods:
Consecutive 1000 children, aged up to five years, attending the Dermatology OPD of RNT Medical College and MB Government Hospital, Udaipur were the subjects of this study. A detailed general, systemic and cutaneous examination followed by relevant investigations were carried out. The findings were recorded in a proforma for analysis and interpretation of data.
Results:
One thousand twenty seven (1027) diagnoses were made in 1000 children. Etiological analysis revealed that majority (417; 40.60%) of dermatoses belonged to infection and infestation group followed by eczematous (358; 34.86%) and hypersensitivity (105; 10.22%) groups. Of the infection and infestation group, bacterial infection (141; 13.72%) was the most common entity followed by scabies (107; 10.42%), fungal (67; 6.52%), and viral infection (35; 3.40%).
Conclusion:
This study provides a preliminary baseline data for future clinical research. It might also help to assess the changing trends of pediatric dermatoses.
Keywords: Bacterial infections, fungal infections, pediatric dermatoses, scabies, viral infections
Introduction

The pattern of skin disease is a consequence of poverty, malnutrition, overcrowding, poor hygiene, illiteracy, and social backwardness in many parts of India.[1] The evaluation for skin disorders is an important component of primary health care practice for all, including children.[2] Status of health, hygiene and personal cleanliness of a society can be judged from the prevalence of certain skin diseases in the children of the community.[3]
Wide range of primary skin disorders are seen during childhood and skin is often a marker of underlying systemic diseases and hereditary syndromes.[4] The pattern of skin diseases varies from country to country with pyoderma and malnutrition being more prevalent in developing countries, while eczemas are more common in developed countries. This can be attributed to differing climatic, cultural and socio-economic factors.[5] Dermatological problems account for about 30% of primary and secondary reasons for pediatric clinic visits and 30% of all visits to dermatologists involve patients of pediatric age group.[6] The incidence of skin diseases in children has been reported to be 9%-37% in various studies.[2,5,7–10]
This study was carried out to share our experience about various dermatoses prevalent among children up to five years of age attending skin OPD at RNT Medical College and MB Government Hospital, Udaipur.
Materials and Methods
Consecutive 1000 children, aged up to five years, attending the Dermatology outpatient department of RNT Medical College and MB Government Hospital, Udaipur were the subjects of this study. A detailed general, systemic and cutaneous examination was done. Relevant investigations were carried out whenever deemed necessary. The findings were recorded in a proforma for analysis and interpretation of data.
Results
Out of total 46,321 patients examined, 1000 (2.16%) patients were children up to five years of age. Males slightly outnumbered females; the male: female ratio was 1.23:1.
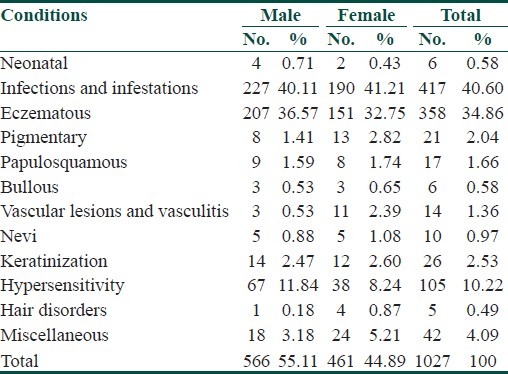
Some of the patients had more than one dermatosis. A total of 1027 dermatoses were recorded in 1000 patients. The majority (417; 40.60%) of dermatoses belonged to infection and infestation group followed by eczematous (358; 34.86%) and hypersensitivity (105; 10.22%) groups. The pattern of other dermatoses is depicted in Table 1.
Table 1.
Pattern of dermatoses (n=1027)
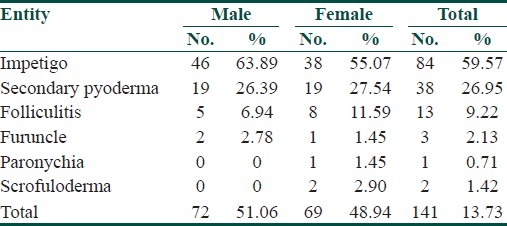
Amongst the infective dermatoses, bacterial infection (141; 13.72%) was the most common entity followed by fungal (67; 6.52%) and viral infection (35; 3.40%). Out of bacterial infections, impetigo (84; 59.57%) was the commonest entity followed by secondary pyoderma (38; 26.95%). The pattern of bacterial infections is shown in Table 2. Of the infestation group, scabies was the most common entity recorded in 107 (10.42%) patients. Molluscum contagiosum (21; 60%) was the commonest viral infection followed by warts (7; 20%). Out of various fungal infections, tinea capitis was seen in majority (47; 70.15%) of the cases followed by tinea faciei (7; 10.45%) and tinea corporis (7; 10.45%).
Table 2.
Pattern of bacterial infections (n=141)
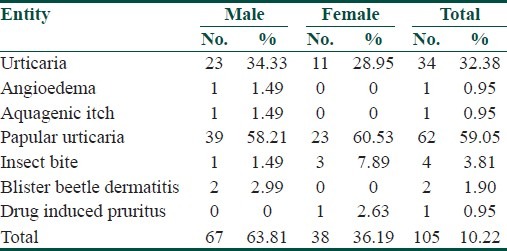
Pattern of eczematous disorders [Table 3] revealed atopic dermatitis to be the commonest (198; 55.31%) followed by seborrhoeic dermatitis (60; 16.76%) and pityriasis alba (29; 8.10%). Twenty four patients of atopic dermatitis had atopic background. Among the hypersensitivity disorders, papular urticaria formed the largest (62; 59.05%) group followed by urticaria (34; 32.38%) as shown in Table 4.
Table 3.
Pattern of eczematous disorders (n=358)
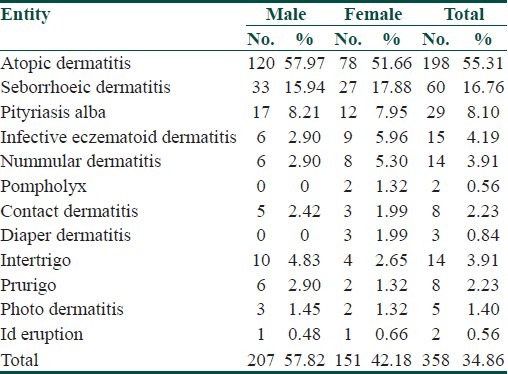
Table 4.
Pattern of hypersensitivity disorders (n=105)
Keratoderma (13; 50%) and ichthyosis (9; 34.62%) were the two most common keratinization disorders. Pigmentary disorders were recorded in 21 patients, of which post inflammatory hypopigmentation was the commonest (14; 66.67%), followed by vitiligo (6; 28.57%). Lichen striatus (6; 35.29%) and lichen nitidus (5; 29.41%) were the commonest entities amongst papulosquamous disorders. No case of lichen planus was recorded. Among the vascular lesions, hemangioma (11; 78.57%) was the most frequent. Out of the 10 patients of nevi, naevus depigmentosus and epidermal nevi were seen in 5 and 4 patients, respectively. Among the miscellaneous disorders, xerosis (19; 45.24%) constituted the largest group followed by acrodermatitis enteropathica (7; 16.67) and miliaria (4; 9.52%).
A pattern of seasonal variation was observed in six common dermatoses. Patients with impetigo and dermatophytic infections were recorded mainly in rainy and summer seasons, while scabies was mostly seen in winter and rainy seasons. Atopic dermatitis and seborrhoeic dermatitis were documented more in winter season and papular urticaria presented predominantly in rainy season.
Discussion
The pattern of skin diseases in pediatric age group vary from one country to another and within the same country from one state to another due to various climatic, cultural and socio-economic factors.[5] The infants are mostly confined to their household, while preschool children aged one to five years are exposed to their neighborhood. Thus, childhood age may be considered as a surrogate marker for environmental risks.[11]
Pattern of pediatric dermatoses has varied in different studies. In this study, majority (417; 40.60%) of dermatoses belonged to infections and infestations group followed by eczemas (358; 34.86%) and hypersensitivity (105; 10.22%) groups. A similar pattern of dermatoses has also been reported in several other studies.[2,5,8,9,12–16] However, in a few studies,[17–20] eczema group has been the predominant dermatoses.
Of the infective dermatoses, bacterial infections (141; 13.72%) were the most common followed by fungal (67; 6.52%) and viral infections (35; 3.40%). Similar pattern has been observed in some other studies as well.[2,9,16,21] Sayal et al.,[5] reported fungal infections to be more common, while viral infections out-numbered bacterial and fungal infections in a study by Wenk and Itin[18] and Gul et al.,[20] The variation among infective dermatoses can possibly be attributed to the region of study, prevalent environmental factors, type of population studied, and hygiene and nutritional status. Impetigo was the commonest (84; 59.57%) bacterial infection followed by secondary pyoderma (38; 26.95%). Most studies[2,5,10–12,17] report impetigo as the commonest bacterial infection. Molluscum contagiosum (21; 60%) was the commonest viral infection followed by warts (7; 20%). A similar observation has been made in several studies.[5,9,16,21] Nanda et al.,[17] however in their study recorded higher prevalence of warts compared to molluscum contagiosum. Tinea capitis was the most frequent fungal infection seen in majority (47; 70.15%) of cases followed by tinea faciei (7; 10.45%) and tinea corporis (7; 10.45%). This is in accordance with other studies[10,13,16] in which tinea capitis was the most common. However, in a study by Sharma and Mendiratta,[21] candidal intertrigo was the most common fungal infection (39.47%) with maximum incidence in infants (63.6%), followed by tinea capitis (34.3%) and tinea corporis (19.15%). This could be due to the pediatric population recruited for the study. Scabies was the most common infestation seen in 107 (10.42%) patients in our study. Almost a similar occurrence (10.61%) has been reported by Sardana et al.[16]
Of the eczema group, atopic dermatitis was the commonest (198; 55.31%) followed by seborrhoeic dermatitis (60; 16.76%) and pityriasis alba (29; 8.10%), a finding similar to other studies.[17,18] However, Hayden[2] documented diaper dermatitis (16%) to be more common followed by atopic dermatitis (9%) and seborrhoeic dermatitis (6%), while Sardana et al.,[16] found infantile seborrhoeic dermatitis (10.49%) to be more common compared to pityriasis alba (5.85%) and atopic dermatitis (5.27%). The incidence of eczemas’ primarily depends upon genetic constitution, individual predisposition, and environmental threats/allergens. Papular urticaria was the commonest hypersensitivity disorder (62; 59.05%) followed by urticaria (34; 32.38%). Sayal et al.,[5] and Sardana et al.,[16] also noticed a frequent occurrence of papular urticaria compared to urticaria, while in some studies,[9,17] urticaria has been reported to be more common than papular urticaria.
Of the nutritional disorders, acrodermatitis enteropathica was the only entity recorded in seven (0.68%) patients. A higher incidence (3.6%) of acrodermatitis enteropathica has also been reported in a study from Karachi by Javed et al.[10] Interestingly, there was only one case of psoriasis and no case of lichen planus found in our study. There was no significant association of various dermatoses with systemic diseases in our study except for a single case of pyoderma in whom hypothyroidism was associated.
The prevalence of certain dermatoses may be influenced by seasonal and climatic changes. This was quite evident in our study in which atopic dermatitis and seborrhoeic dermatitis were noted predominantly in winters while papular urticaria was seen more frequently in rainy season. Dhar et al.,[22] in a large series of 672 children of atopic dermatitis documented disease aggravation during winters in 67.14% and 58% of infantile and childhood atopic dermatitis cases, respectively. Banerjee et al.,[23] studied seasonal variations in pediatric dermatoses and found scabies and seborrhoeic dermatitis to be more prevalent during winter, while impetigo, furunculosis, and miliaria during summer and rainy seasons. Papular urticaria was more frequent in the rainy season. Almost a similar observation was documented in our study also.
This study provides a preliminary baseline data for future epidemiological and clinical research. It might also help to assess the changing trends of pediatric dermatoses.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.Kandhari S. Ecology of skin diseases in India. In: Valia RG, Valia VR, editors. IADVL Textbook of Dematology. 3rd ed. Mumbai India: Bhalani Publishing House; 2008. pp. 1–6. [Google Scholar]
- 2.Hayden GF. Skin diseases encountered in a pediatric clinic. Am J Dis Child. 1985;139:36–8. doi: 10.1001/archpedi.1985.02140030038023. [DOI] [PubMed] [Google Scholar]
- 3.Sharma NK, Garg BK, Goel M. Pattern of skin diseases in urban school children. Indian J Dermatol Venereol Leprol. 1986;52:330–1. [PubMed] [Google Scholar]
- 4.Gupta P, Sarkar R. Common skin disorders and leprosy. In: Ghai OP, Gupta P, Paul VK, editors. Ghai Essential Pediatrics. 6th ed. New Delhi: CBS Publishers and Distributors; 2004. pp. 627–63. [Google Scholar]
- 5.Sayal SK, Bal AS, Gupta CM. Pattern of skin diseases in pediatric age group and adolescents. Indian J Dermatol Venereol Leprol. 1998;64:117–9. [PubMed] [Google Scholar]
- 6.Schachner LA, Hansen RG. Preface. In: Schachner LA, Hansen RG, editors. Pediatric dermatology. 2nd ed. New York: Churchill Livingstone; 1995. p. 9. [Google Scholar]
- 7.Gram YC. Skin diseases in children in Singapore. Ann Acad Med Singapore. 1988;17:569–72. [PubMed] [Google Scholar]
- 8.Porter MJ, Mack RW, Chaudhary MA. Pediatric skin disease in Pakistan: A study of three Punjab villages. Int J Dermatol. 1984;23:613–7. doi: 10.1111/j.1365-4362.1984.tb05701.x. [DOI] [PubMed] [Google Scholar]
- 9.Karthikeyan K, Thappa DM, Jeevankumar B. Pattern of pediatric dermatoses in a referral centre in South India. Indian Pediatr. 2004;41:373–7. [PubMed] [Google Scholar]
- 10.Javed M, Jairamani C. Pediatric dermatology: An audit at Hamdard University Hospital, Karachi. J Pak Assoc Dermatol. 2006;16:93–6. [Google Scholar]
- 11.Mitra M, Mitra C, Gangopadhyay DN. Effect of environment on pediatric dermatoses. Indian J Dermatol. 2005;50:64–7. [Google Scholar]
- 12.Koley SK, Sen MK, Sengupta SN. Incidence of skin diseases in children in the district of Bankura. Indian J Pediatr. 1975;42:106–9. doi: 10.1007/BF02796462. [DOI] [PubMed] [Google Scholar]
- 13.Ghosh SK, Saha DK, Roy AK. A clinico-aetiological study of dermatoses in paediatric age group. Indian J Dermatol. 1995;40:29–31. [Google Scholar]
- 14.Bhatia V. Extent and pattern of paediatric dermatoses in rural areas of Central India. Indian J Dermatol Venereol Leprol. 1997;63:22–5. [PubMed] [Google Scholar]
- 15.Negi KS, Kandpal SD, Parsad D. Pattern of skin diseases in children in Garhwal region of Uttar Pradesh. Indian Pediatr. 2001;38:77–80. [PubMed] [Google Scholar]
- 16.Sardana K, Mahajan S, Sarkar R, Mendiratta V, Bhushan P, Koranne RV, et al. The spectrum of skin disease among Indian children. Pediatr Dermatol. 2009;26:6–13. doi: 10.1111/j.1525-1470.2008.00814.x. [DOI] [PubMed] [Google Scholar]
- 17.Nanda A, Hasawi FA, Alsaleh QA. A prospective survey of pediatric dermatology clinic patients in Kuwait: An analysis of 10,000 cases. Pediatr Dermatol. 1999;16:6–11. doi: 10.1046/j.1525-1470.1999.99002.x. [DOI] [PubMed] [Google Scholar]
- 18.Wenk C, Itin PH. Epidemiology of pediatric dermatology and allergology in the region of Aargau, Switzerland. Pediatr Dermatol. 2003;20:482–7. doi: 10.1111/j.1525-1470.2003.20605.x. [DOI] [PubMed] [Google Scholar]
- 19.Hon KL, Leung TF, Wong Y, Ma KC, Fok TF. Skin diseases in Chinese children at a pediatric dermatology centre. Pediatr Dermatol. 2004;21:109–12. doi: 10.1111/j.0736-8046.2004.21203.x. [DOI] [PubMed] [Google Scholar]
- 20.Gul U, Cakmak SK, Gonul M, Kilic A, Bilgili S. Pediatric skin disorders encountered in a dermatology outpatient clinic in Turkey. Pediatr Dermatol. 2008;25:277–8. doi: 10.1111/j.1525-1470.2008.00656.x. [DOI] [PubMed] [Google Scholar]
- 21.Sharma RC, Mendiratta V. Clinical profile of cutaneous infections and infestations in the paediatric age group. Indian J Dermatol. 1999;44:174–8. [Google Scholar]
- 22.Dhar S, Kanwar A J. Epidemiology and clinical pattern of atopic dermatitis in a North Indian pediatric population. Pediatr Dermatol. 1998;15:347–51. doi: 10.1046/j.1525-1470.1998.1998015347.x. [DOI] [PubMed] [Google Scholar]
- 23.Banerjee S, Gangopadhyay DN, Jana S, Mitra C. Seasonal variations in pediatric dermatoses. Indian J Dermatol. 2010;55:44–6. doi: 10.4103/0019-5154.60351. [DOI] [PMC free article] [PubMed] [Google Scholar]