

Marijuana, the common name for Cannabis sativa, is a widely distributed hemp plant whose dried flowering tops and leaves have been used for medicinal purposes for 12,000 years by some estimates (1). The article by Malfait et al. (2) in this issue of PNAS is relevant to the question of whether such traditional uses of marijuana could be clinically justifiable today.
Contemporary discussions of the medical value of marijuana must be undertaken within a larger cultural, legal, and political context (Workshop on the Medical Utility of Marijuana, National Institutes of Health, http://www.nih. gov/news/medmarijuana/MedicalMarijuana.htm). The perceived behavioral and addictive effects of marijuana led to its prohibition from nonmedical uses by most states, taxation at the federal level, and eventual removal from the U.S. Pharmacopoeia in the 1930s and 1940s. Nonetheless, smoking of marijuana cigarettes continued and became the recreational drug practice of choice as well as a virtual rite of passage for young people during the Vietnam era. Some people who suffered chronic debilitating illnesses observed that marijuana eased some of their symptoms. A movement grew to redefine marijuana as a neglected, but valuable, therapeutic tool. Today, that movement has been subsumed under a more general advocacy for a whole spectrum of complementary and alternative health approaches (3).
Complementary and alternative medicine entails the use of unconventional diagnostic, preventative, and therapeutic approaches including acupuncture, chiropractic manipulation, homeopathy, and magnets, few of which have been tested according to rigorous scientific standards. Herbal and other botanical products are key components of many alternative health approaches. Numerous preparations are marketed in the United States as nutritional supplements with such promises as combating fatigue, restoring mental balance, warding off respiratory infections, losing weight, and relieving the pains of arthritis.
Were botanical products merely inert food supplements or condiments, there would be little concern over their use. But the very discoveries that yielded aspirin, digoxin, vincristine, taxol, and many other valuable plant-based drugs informed us as well of their potential for harm. Despite the common belief that natural substances must be healthful, the media and scientific literature today are rife with reports of serious adverse effects of particular botanical supplements and unexpected interactions between some supplements and proprietary drugs. Thus, the public need for definitive preclinical and clinical testing of botanicals and other unconventional healing approaches led to the creation in 1999 of the National Center for Complementary and Alternative Medicine at the National Institutes of Health.
With regard to marijuana, there are data to indicate that the plant, or at least some of its constituents, conveys some clinical benefits, but a number of risks as well. Comprehensive reviews of the medical utility of marijuana were undertaken by a National Institutes of Health workshop in 1997 and by the Institute of Medicine in 1999 (http: //www.nih.gov/news/medmarijuana/MedicalMarijuana.htm and ref. 4). These reviews concluded that smoking marijuana reduces intraocular pressure in glaucoma and is claimed to ameliorate pain, cachexia, nausea, and other debilitating conditions. Unfortunately, large controlled trials have not been conducted to support the majority of such claims. Moreover, there are better, well-defined treatments for virtually all such indications.
Far more certain than reports of the benefits of marijuana smoking, however, are the health risks it imposes. Studies have described its adverse psychological, cardiovascular, and pulmonary effects, and even raised the specter of an increased risk of cancer (5, 6).
In contrast to the incomplete state of the science regarding use of the plant itself, the identity, pharmacology, and clinical effects of several of marijuana's constituents are relatively well characterized (7, 8). Marijuana contains more than 60 distinct cannabinoids, of which a series of tetrahydrocannabinols (THC) and their metabolites are the primary psychoactive ingredients and best-known components (Fig. 1). Δ9-THC alleviates the nausea associated with cancer chemotherapy and AIDS wasting and is available for these indications as the prescription drug dronabinol. Even the nonpsychoactive cannabinoids have been shown to have cellular and physiologic effects that could prove of clinical value.
Figure 1.
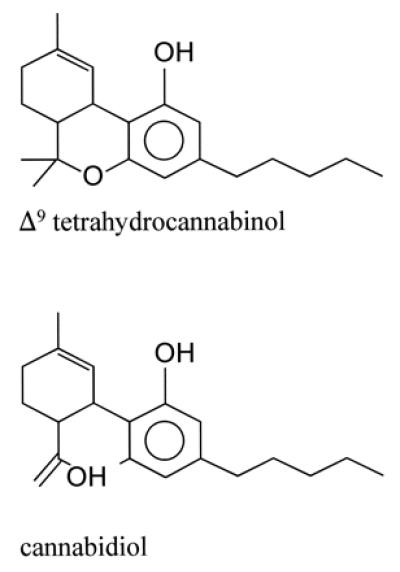
The chemical structures of Δ9-THC and cannabidiol.
The paper by Malfait et al. (2) summarizes in vitro and in vivo immunological studies of the marijuana constituent cannabidiol (CBD; Fig. 1) and its potential effects in the treatment of arthritis (1). Using a murine model in which arthritis is induced by immunization with type II collagen, the authors show that CBD blocks the inflammatory infiltrate and progression of joint damage. CBD appears effective both orally and intraperitoneally, but with a rather sharp dose-response peak, above or below which efficacy is less evident. A series of ex vivo studies indicate that CBD attenuates the oxidative burst in granulocytes, lymphocyte proliferation, and the release of proinflammatory cytokines.
Numerous prior studies of marijuana itself, unfractionated marijuana extracts, and individual cannabinoids revealed that they manifest a wide range of immunologic effects, both in vitro and in vivo, in animals as well as in human subjects (reviewed in ref. 9). Generally suppressive effects on T cell, B cell, macrophage, natural killer cell, and neutrophil functions have been described. Proliferation is impaired, as is release of selected cytokines and chemokines, but the findings differ by cell type, experimental conditions, and especially the concentration of the cannabinoids examined. The effects are sufficient, nonetheless, to impair host responses to animal challenges with several viral and bacterial pathogens. Moreover, the psychoactive potential of the molecule does not correlate with its immunological effects. For example, both THC and CBD were shown to inhibit release of IFN-γ and tumor necrosis factor α from cultured human peripheral blood mononuclear cells (10, 11). In some assays, the effects by one paralleled the other; in others, CBD was more potent. Importantly, the dose–response for either substance was complex, being stimulatory at concentrations of 0.01–0.1 μg/ml, the range of serum levels detected in marijuana smokers, but strongly inhibitory at 0.5–20 μg/ml. Given the tight peak response to CBD observed in the present report and its still undefined pharmacokinetics, it might be difficult to develop CBD into a useful anti-inflammatory or immunosuppressive drug.
Another issue that bears on the potential therapeutic utility of CBD, or any cannabinoid designed for prolonged use, is its toxicity, an issue that was not addressed by Malfait et al. (2). In addition to adverse effects like tremors, convulsions (12), and embryotoxicity (13) observed in formal animal studies, there are effects associated with its intended use, such as the suppression of inflammatory cytokine responses. Early experiences with the anti-tumor necrosis factor agents infliximab and etanercept revealed an increased incidence of intercurrent infections (14). Their long-term effects on dormant infections with mycobacteria or other intracellular pathogens are not known. An increased risk of lymphomas has been postulated as well (15).
Regardless of its eventual utility and safety, CBD is a potential lead to new classes of agents that would interfere with inflammatory pathways. Although one could only speculate as to why a common weed like Cannabis would evolve to contain THC and CBD, we do know something of the cellular mechanisms by which it acts on the mammalian immune and nervous systems. Two related cannabinoid receptors have been described: CB1 and CB2 (Table 1; refs. 16 and 17). They are both widely distributed G-coupled protein receptors. High densities of CB1 are found in the cortex, limbic system, and hippocampus, where endogenous ligands like anandamide serve as neurotransmitters. CB2 also is expressed in the brain, but is found in relatively higher concentrations than CB1 in various lymphocyte subpopulations, especially B cells. That CBD does not bind to either CB1 or CB2 implies that additional receptors remain to be discovered. The evolving work suggests that the differential expression of cannabinoid receptors, and the particular endogenous ligands accessible to them in specific tissues, constitute a rich regulatory network (18, 19).
Table 1.
The distribution and ligand affinitives of cannabinoid receptors
| Receptor
|
||
|---|---|---|
| CB1 | CB2 | |
| Ligand activity | ||
| Δ9-THC | Agonist | Weak antagonist |
| Cannabidiol | Does not bind | Does not bind |
| Anandamide | Agonist | Agonist |
| Tissue distribution | ||
| Greatest activity | Brain | Immune system |
Many proponents of complementary and alternative medicine find the discovery of neuro-immune effector molecules, such as the cannabinoid receptors and their endogenous ligands, to be an exciting validation of their traditional beliefs about the unity of mind and body. They extol the proverbial wisdom of nature in providing medicinal plants whose components can affect human cells through evolutionarily conserved biochemical mechanisms. They believe, as well, that the multiplicity of related constituents in medicinal plants act collectively to enhance overall beneficial effects while tempering adverse ones.
It is conceivable that marijuana contains a series of cannabinoids that, in the aggregate, could alleviate arthritis as implied in the present report (2), yet remain well tolerated. Remarkably, the claim that marijuana does so also was made 4,000 years ago by the Chinese emperor Shen-nung whose pharmacobotanical compendium, the Pen-ts'ao Ching, concluded that cannabis “undoes rheumatism” (cited in ref. 20). These are ideas that are now susceptible to critical scrutiny through controlled trials in which purified plant constituents are compared, alone and in combination, with whole-plant products.
Footnotes
See companion article on page 9561.
Article published online before print: Proc. Natl. Acad. Sci. USA, 10.1073/pnas.180314297.
Article and publication date are at www.pnas.org/cgi/doi/10.1073/pnas.180314297
References
- 1.Abel E L. Marijuana: The First Twelve Thousand Years. New York: Plenum; 1980. [Google Scholar]
- 2.Malfait A M, Gallily R, Sumariwalla P F, Malik A S, Andreakos E, Mechoulam R, Feldmann M. Proc Natl Acad Sci USA. 2000;97:9561–9566. doi: 10.1073/pnas.160105897. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Eisenberg D M, Davis R B, Ettner S L, Appel S, Wilkey S, Van Rompay M, Kessler R C. J Am Med Assoc. 1998;180:1569–1575. doi: 10.1001/jama.280.18.1569. [DOI] [PubMed] [Google Scholar]
- 4.Joy J E, Watson S J, Benson J A Jr, editors. Marijuana and Medicine: Assessing the Science Base. Washington, DC: Natl. Acad. Press; 1999. [PubMed] [Google Scholar]
- 5.Roth M D, Arora A, Barsky S H, Kleerup E C, Simmons M S, Tashkin D P. Am J Respir Crit Care Med. 1998;157:1–9. [Google Scholar]
- 6.Zhang Z F, Morgenstern H, Spita M R, Tashkin D P, Marshall J R, Hsu T C, Schantz S P. Cancer Epidemiol Biomarkers Prev. 1999;8:1071–1078. [PubMed] [Google Scholar]
- 7.Mechoulam R. Science. 1970;168:1159–1166. doi: 10.1126/science.168.3936.1159. [DOI] [PubMed] [Google Scholar]
- 8.Razdan R K. Pharmacol Rev. 1986;38:75–149. [PubMed] [Google Scholar]
- 9.Klein T W, Friedman H, Specter S. Neuroimmunology. 1998;83:102–105. doi: 10.1016/s0165-5728(97)00226-9. [DOI] [PubMed] [Google Scholar]
- 10.Watzl B, Scuderi P, Watson R R. Intl Soc Immunopharmacol. 1991;13:1091–1097. doi: 10.1016/0192-0561(91)90160-9. [DOI] [PubMed] [Google Scholar]
- 11.Srivastava M D, Srivastava B I S, Brouhard B. Immunopharmacology. 1998;40:179–185. doi: 10.1016/s0162-3109(98)00041-1. [DOI] [PubMed] [Google Scholar]
- 12.Rosenkrantz H, Fleischman R W, Grant R J. Toxicol Appl Pharmacol. 1981;58:118–131. doi: 10.1016/0041-008x(81)90122-8. [DOI] [PubMed] [Google Scholar]
- 13.Fleischman R W, Naqvi R H, Rosenkrantz H. J Environ Pathol Toxicol. 1980;4:471–482. [PubMed] [Google Scholar]
- 14.Maini R N, Taylor P C. Annu Rev Med. 2000;51:207–229. doi: 10.1146/annurev.med.51.1.207. [DOI] [PubMed] [Google Scholar]
- 15.Bickston S J, Lichtenstein G R, Arseneau K O, Cohen R B, Cominelli F. Gastroenterology. 1999;117:1433–1437. doi: 10.1016/s0016-5085(99)70294-5. [DOI] [PubMed] [Google Scholar]
- 16.Matsuda L A, Lolait S J, Brownstein M J, Young A C, Bonner T I. Nature (London) 1990;346:561–564. doi: 10.1038/346561a0. [DOI] [PubMed] [Google Scholar]
- 17.Munro S, Thomas K L, Abu-Shaar M. Nature (London) 1993;365:61–65. doi: 10.1038/365061a0. [DOI] [PubMed] [Google Scholar]
- 18.Martin B R, Mechoulam R, Razdan R K. Life Sci. 1999;65:573–595. doi: 10.1016/s0024-3205(99)00281-7. [DOI] [PubMed] [Google Scholar]
- 19.Klein T W, Newton C, Friedman H. Immunol Today. 1998;19:272–281. doi: 10.1016/s0167-5699(98)01300-0. [DOI] [PubMed] [Google Scholar]
- 20.Hui-Lin L. In: Cannabis and Culture. Rubin V, editor. The Hague: Mouton; 1975. pp. 51–62. [Google Scholar]