

Abstract
Background: The electrocardiogram (ECG) can be used to predict cardiovascular risk; however, like all risk factors with imperfect specificity, studies in low risk populations have been plagued by poor predictive accuracy. Although predictive accuracy might be improved among cohorts with a higher likelihood of cardiovascular events, this would also affect the prevalence of abnormal parameters and their exclusions.
Method: To determine the magnitude of these changes in a cohort with ischemic cardiomyopathy we analyzed 15 previously validated high‐risk parameters from the resting and ambulatory ECG in subjects enrolled in the Prediction of Arrhythmic Events with Positron Emission Tomography (PAREPET) study (n = 198).
Results: Using the published exclusion criteria from the validation studies (i.e., atrial fibrillation, persistent pacing, prolonged QRS), only 4 high‐risk ECG parameters (27%) could be evaluated in all subjects and only 42% of subjects could have all 15 ECG parameters assessed. Nevertheless, almost every subject (97%) had at least one abnormal parameter. On average, there were 3.4 ± 1.8 (range, 0–8) high‐risk ECG parameters per subject among the 11.7 ± 4.5 (range, 4–15) parameters that could be assessed.
Conclusions: Thus, 34% of all assessable parameters were abnormal. In conclusion, a significant proportion of ECG parameters cannot be assessed in patients with ischemic cardiomyopathy, but high‐risk results are ubiquitous. The influence of these issues will be clarified when the results of the PAREPET study are available to actually determine the predictive value of these parameters on cause‐specific mortality in a high‐risk cohort.
Keywords: electrocardiography, ischemic cardiomyopathy, high‐risk, cardiac death
In view of its limited cost and universal availability, the electrocardiogram (ECG) is an integral part of almost every cardiovascular evaluation. This ubiquity has facilitated numerous large scale investigations that have clearly shown that selected parameters can predict cardiovascular events and mortality. Nevertheless, these investigations have primarily involved relatively low risk populations in whom low event rates have resulted in poor predictive accuracy of individual ECG parameters. 1 , 2 , 3 , 4 , 5 , 6
At the other end of the clinical spectrum are the patients with known coronary artery disease. Although the subsequent death is likely to be cardiac, predicting the eventual mode of death (i.e., sudden versus nonsudden, implantable defibrillator utilization) or time‐to‐event has significant clinical and research implication. 7 , 8 Interestingly, investigations of ECG predictors in these patients has primarily focused on novel and sophisticated parameters rather than the simple and straightforward indices that have been so extensively validated in lower risk populations. The explanation for this deficiency is not entirely clear; however, we hypothesized two potentially complementary factors that could undermine the prognostic utility of ECG parameters in patients with ischemic cardiomyopathy. First, there would be such a high prevalence of ECG parameters associated with high‐risk that a complex analytic scheme would be required to stratify and prioritize parameters. Second, a high prevalence of coexisting conditions (i.e., atrial fibrillation and persistent ventricular pacing) would preclude the evaluation of many parameters; in addition complicating attempts to categorize levels of risk. Accordingly, this study was specifically designed to determine the prevalence of high‐risk ECG parameters and the frequency of previously published exclusion criteria in patients with ischemic cardiomyopathy.
METHODS
Subjects for this investigation are from the ongoing PAREPET study (Prediction of Arrhythmic Events with Positron Emission Tomography), a National Institute of Health‐funded observational cohort study evaluating positron emission tomography to predict sudden cardiac death (SCD). 9 The PAREPET study enrolled patients with documented ischemic cardiomyopathy with an ejection fraction (EF) ≤35% with New York State Heart Association (NYHA) functional Class I–III heart failure, and no plans for coronary revascularization. Exclusion criteria included: history of resuscitated SCD, sustained ventricular tachycardia (VT), implantable‐cardioverter defibrillator discharge, unexplained syncope; recent myocardial infarction (30 days), percutaneous coronary intervention (3 months), coronary bypass surgery (1 year); or comorbidities that reduced life expectancy to fewer than 2 years.
Electrocardiographic Monitoring
All subjects had high resolution (1000 samples per second) ambulatory 12‐lead ECG monitoring (H12+ Holter recorders, V3.12, Mortara Instruments; Milwaukee, WI, USA) with the Mason‐Likar lead configuration, resulting in high fidelity recordings with a frequency response of 0.05–60 Hz. For the resting 12‐lead ECG variables, the first ECG of the monitoring period was selected while the subject was supine. The ELI LINK program (Mortara Instruments) was used to export a single 12‐lead ECG with the standard filter setting of 0.05–150 Hz for subsequent analysis. Among patients with intermittent ventricular pacing, a high resolution 12‐lead ECG was also exported for analysis during periods of intrinsic rhythm. Standard 12‐lead ECGs were then analyzed by a reviewer blinded to all clinical data.
High‐Risk ECG Parameters
Fifteen high‐risk ECG parameters were identified from the literature to be consistently associated with cardiac mortality and/or SCD. The previously validated operational definitions, cutoff‐points for risk, and exclusion criteria were applied. Table 1 shows the frequency of various exclusion criteria and the high‐risk parameters affected.
Table 1.
High Risk ECG Parameters and Their Respective Previously Published Exclusion Criteria
| n = 198 | OR/HR | Exclusion Criteria | ||||
|---|---|---|---|---|---|---|
| None | Persistent RV or BiV Pacing | Atrial Fibrillation | LBBB | QRSd ≥ 120 ms | ||
| Number of subjects excluded | 0 | 43 | 20 | 11 | 114 | |
| % of Subjects excluded | 0% | 22% | 10% | 6% | 58% | |
| ECG features | ||||||
| 1 Atrial Fibrillation | 1.4 4 | X | ||||
| 2 Nonsustained VT | 2.9 15 | X | ||||
| 3 Fragmented QRS | 1.5 31 | X | ||||
| 4 Persistent RV pacing | 3.0 18 | X | ||||
| 5 Q waves | 2.2 5 | X | ||||
| 6 Left ventricular hypertrophy | 1.5 12 | X | ||||
| 7 Left bundle branch block | 2.5 20 | X | ||||
| 8 Dynamic ST depression | 5.3 21 | X | X | |||
| 9 Elevated minimum HR | 2.1 6 | X | X | |||
| 10 Frequent premature ventricular complexes | 2.8 6 | X | X | |||
| 11 Prolonged QRSd | 1.2 12 | X | X | |||
| 12 Low heart rate variability | 5.0 24 | X | X | |||
| 13 Prolonged QTc | 2.5 2 | X | X | X | ||
| 14 Steep QT/RR slope | 1.6 13 | X | X | X | ||
| 15 Wide spatial QRS‐T angle | 2.4 7 | X | X | X | X |
OR = odds ratio; HR = hazards ratio; RV = right ventricle; BiV = biventricular pacing; LBBB = left bundle branch block; QRSd = QRS duration; VT = ventricular tachycardia; HR = heart rate; QTc = corrected QT interval; RR = R to R interval.
-
1
Assessed in all subjects:
-
(i)
Atrial Fibrillation: any presence of irregular R–R intervals with absence of P waves, (manually obtained). 5
-
(ii)
Nonsustained VT (NSVT): at least one episode of three or more consecutive premature ventricular complexes (PVCs) at rate ≥120 beats per minute (bpm, manually obtained). 10
-
(iii)
Fragmented QRS Complexes (fQRS): with a narrow QRS complex (<120 ms) any RSR morphology, notching in the nadir of the S wave or more than one R wave in two contiguous leads 11 ; or with a prolonged QRS complex (≥120 ms) due to bundle branch block, nonspecific intraventricular conduction disturbance or paced rhythm an fQRS was defined as the presence of >2 R’ or >2 notches in the nadir of the S wave (manually obtained). 12
-
(iv)
Persistent Right Ventricular (RV) Pacing: continuous (100% of monitoring time) prolonged QRS complexes with single‐chamber ventricular pacemaker spikes (automated measure). 13 Biventricular (BiV) pacing was not considered a high‐risk parameter.
-
2
Excluding subjects with persistent RV or BiV pacing:
-
(v)
Q Waves: at least one pathologic Q wave (≥40 ms wide and 1/4 of R wave amplitude) in each of anterior, lateral, and inferior territories (manually obtained). 3 In order to determine the potential impact of the Mason‐Likar lead configuration on the frequency of Q waves, standard ECGs were reviewed on a subset of subjects (n = 20). There was close correlation between the number of leads with Q waves (r = 0.57) and the number of regions with Q waves (r = 0.63) between the two lead systems. Similarly, there was very good agreement among regions with Q waves (intraclass correlation coefficient = 0.74). Nevertheless, the American Heart Association scientific statement cautions that there are differences in the ECG waveforms when electrodes are moved from standard wrist/ankle positions to the torso. 14
-
(vi)
Left Ventricular Hypertrophy (LVH): Cornell criteria of the sum of SV3 and RaVL voltage > 20 mm (women) or 28 mm (men), (manually obtained). 15
-
(vii)
Left Bundle Branch Block (LBBB): QRSd ≥120 ms plus broad notched or slurred R wave in leads I, aVL, V5‐V6, and an RS pattern in V5‐V6 (manually obtained). 16
-
3
Excluding subjects with LBBB or persistent RV or BiV pacing:
-
(viii)
Dynamic ST Depression: at least one episode of J‐point depression of ≥0.5 mm in leads V2‐V3 or ≥1 mm in all other leads in two or more contiguous leads for at least 5 minutes (manually obtained). 17
-
4
Excluding subjects with atrial fibrillation or persistent RV or BiV pacing:
-
(ix)
Elevated Minimum Heart Rate (min HR): minimum HR averaged for any five second period during monitoring ≥65 bpm (automated measure). 1
-
(x)
Frequent PVCs: ≥10 premature QRS complexes with ectopic morphology and QRSd >120 ms per hour, for at least 20 hours of the recording period (manually obtained). 10
-
(xi)
Prolonged QRS Duration (QRSd): the global QRS duration (earliest onset to the latest offset) averaged among all leads >110 ms (automated measure). 18
-
(xii)
Low HR Variability (HRV): beat‐to‐beat frequency analysis of the RR intervals (automated measure) with at least one of the following: (a) standard deviation of normal‐to‐normal RR intervals <50 ms (SDNN); (b) the square root of the mean squared differences of successive normal‐to‐normal intervals <15 ms (rmsSD); or (c) the frequency of interval differences of successive normal‐to‐normal intervals greater than 50 ms <75% (rr50). 19 , 20
-
5
Excluding subjects with atrial fibrillation, LBBB or persistent RV or BiV pacing:
-
(xiii)
Prolonged Corrected QT Interval (QTc): QT interval corrected for HR using the Bazett formula (QT/RR1/2) >450 ms (men) or >470 ms (women) (automated measure). 4
-
(xiv)
Steep QT/RR Slope: regression line slope of the beat‐to‐beat QT and RR relationship over the entire monitoring period >0.22 (automated measure). 21 , 22
-
6
Excluding subjects with atrial fibrillation, persistent RV or BiV pacing or QRSd ≥120 ms:
Echocardiography
Two‐dimensional transthoracic echocardiography was performed in all subjects with a 2.25 MHz phased‐array transducer with harmonic imaging, including standard parasternal long‐ and short‐axis, apical two‐ and four‐chamber, and subcostal views. Ventricular volumes and EF were obtained from the apical two‐chamber and apical four‐chamber views, as recommended by the American Society of Echocardiography. 25 , 26 Criteria for echocardiographic evidence of LVH were ≥96 g/m2 in women and ≥116 g/m2 in men. 27
Statistical Analysis
All values are mean ± standard deviation. The degree of association between the number of high‐risk ECG parameters and various demographic and electrocardiographic parameters was determined using the Pearson's correlation coefficient (r). All statistical analyses were performed with SPSS (Version 17). P < 0.05 was considered statistically significant.
RESULTS
Key demographic and clinical characteristics of the 198 subjects included in this analysis are shown in Table 2. Consistent with their diagnosis of ischemic cardiomyopathy, almost all subjects were pharmacologically managed with beta blockers (96%) and angiotensin receptor blockers or angiotensin converting enzyme inhibitors (88%).
Table 2.
Baseline Characteristics (n = 198)
| Variable | Mean ± SD |
|---|---|
| Age (years) | 67.2 ± 11.7 |
| Male sex, n (%) | 179 (90%) |
| NYHA functional class | 2.1 ± 0.8 |
| CCS angina class | 1.7 ± 0.7 |
| End‐diastolic volume index (mL/m2) | 87.5 ± 29.2 |
| End‐systolic volume index (mL/m2) | 64.6 ± 26.1 |
| Mitral regurgitation severity | 1.6 ± 1.2 |
| Ejection fraction | 0.27 ± 0.09 |
SD = standard deviation; NYHA = New York State Heart Association; CCS = Canadian Cardiovascular Society.
High‐Risk ECG Parameters
Ambulatory monitoring was performed for 23.9 ± 0.8 hours (range, 16–24 hours) and high quality interpretable signals were obtained in all subjects. A representative 12 lead ECG illustrating several high‐risk ECG parameters is shown in Figure 1. The average HR over the recording period was 72 ± 10 bpm (range, 52–116). Only 4 of the 15 (27%) high‐risk ECG parameters could be assessed in all subjects (Table 1), and only 84 subjects (42%) could have all high‐risk ECG parameters assessed. The frequency of high‐risk ECG parameters in this population is shown in Table 3 and Figure 2.
Figure 1.
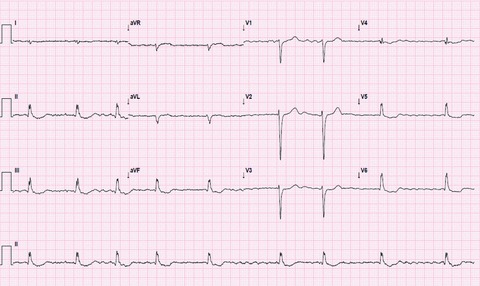
Representative Resting ECG. A high resolution resting 12‐lead ECG with multiple high‐risk parameters including: atrial fibrillation, prolonged QRS duration, prolonged QTc, and fragmented QRS complexes.
Table 3.
Prevalence of Cardiac Death High Risk ECG Features in Patients with Ischemic Cardiomyopathy (n = 198)
| Parameter | Mean ± SD (Range) | Cutoff Value for Risk of Cardiac Death | Abnormal n (%) | Prevalence*(%) |
|---|---|---|---|---|
| All patients (n = 198) | ||||
| Atrial fibrillation (count) | – | Present 4 | 20 (10.1) | 10.1 |
| Nonsustained VT (count) | 4.9 ± 11.1 (0‐61) | 1 episode of ≥3 consecutive PVCs 15 | 94 (47.5) | 47.5 |
| Fragmented QRS (count) | 1.5 ± 2.1 (0‐8) | 2 leads with fQRS in same territory 31 | 102 (51.5) | 51.5 |
| Pacing (% of recording) | 77.2 ± 37.8 (1‐100) | Persistent RV pacing 18 | 9 (4.5) | 4.5 |
| Excluding Persistent RV & BiV pacing (n = 155) | ||||
| Q Waves (count) | 1.8 ± 2.0 (0‐9) | One Q wave in each territory 5 | 15 (9.7) | 7.6 |
| Left ventricular hypertrophy (count) | – | Present per Cornell 19 | 16 (10.3) | 8.1 |
| Left Bundle Branch Block (count) | – | Present per AHA 20 | 11 (7.1) | 5.6 |
| Excluding LBBB or persistent RV & BiV pacing (n = 144) | ||||
| Dynamic ST depression (count) | – | >1 mm for 1 min in 2 consecutive leads 21 | 69 (47.9) | 34.8 |
| Excluding atrial fibrillation or persistent RV & BiV pacing (n = 141) | ||||
| Elevated minimum HR (beat/min) | 52 ± 10 (22‐91) | ≥65 22 | 12 (8.5) | 6.1 |
| Frequent premature Ventricular complexes (count) | 250 ± 155 (0‐880) | ≥10 PVCs per hr 15 | 62 (44.0) | 31.3 |
| Prolonged QRS duration (ms) | 125 ± 27 (67‐210) | >110 12 | 94 (66.7) | 47.5 |
| Low heart rate variability | 22 (15.6) | 11.1 | ||
| RR50 (%) | 12 ± 19 (0‐91) | <0.75 23 ‐ 24 or | ||
| rmsSD (ms) | 73 ± 67 (1‐591) | <15 23 ‐ 24 or | ||
| SDNN (ms) | 110 ± 52 (0‐377 | <50 23 ‐ 24 | ||
| Excluding atrial fibrillation, LBBB or persistent RV & BiV pacing (n = 130) | ||||
| Prolonged QTc (ms) | 447 ± 40 (350‐561) | >450 men or >470 women 2 | 32 (24.6) | 16.2 |
| Steep QT/RR slope (value) | 0.21 ± 0.12 (‐0.4‐0.9) | >0.22 13 | 49 (37.7) | 24.7 |
| Excluding atrial fibrillation, LBBB, persistent RV & BiV pacing, or wide (≥120ms) QRS complexes (n = 84) | ||||
| Wide QRS‐T angle (degrees) | 122 ± 38 (12‐176) | >100 7 | 61 (72.6) | 30.8 |
| Total | ||||
| Number of assessable features per patient | 11.7 ± 4.5 (4‐15) | – | – | – |
| Number of positive features per patient | 3.4 ± 1.8 (0‐8) |
HR = heart rate; VT = ventricular tachycardia; RV = right ventricle; BiV = biventricular; LBBB = left bundle branch block. (*) Prevalence is adjusted to the overall sample (n = 198).
Figure 2.
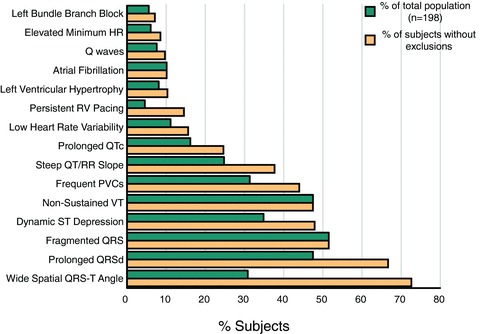
Prevalence of High‐Risk ECG Parameters in PAREPET Subjects. The prevalence of each of the 15 high‐risk ECG parameters is shown as both a percent of the entire population (green bars, n = 198) and as a percent of those subjects without exclusion criteria for analysis of that particular parameter (gold bars, n = 84–198).
Atrial Fibrillation, NSVT, fQRS, Persistent RV Pacing (n = 198)
The intrinsic rhythm was sinus in 178 subjects (90%) with atrial fibrillation in the remaining 20 (10%). An episode of NSVT occurred in almost half of the subjects (n = 94, 48%) and a majority had fragmented QRS complexes (n = 102, 52%). A pacemaker was present in 175 (88%), and 62 subjects (35%) had at least some ventricular pacing during monitoring. Persistent ventricular pacing was present in 43 subjects (22%) of whom 9 had single‐chamber RV pacing (a high‐risk parameter) and the remaining 34 had BiV pacing (not a high‐risk parameter).
Q Waves, LVH, LBBB (n = 155)
As expected in a population with ischemic cardiomyopathy, pathologic Q waves were frequently present (at least one pathologic Q wave in 139 subjects (90%); however, the high‐risk parameter of Q waves in each coronary distribution was uncommon (n = 15, 10%). A LBBB ventricular depolarization pattern was relatively uncommon (n = 11, 7%), at least in part related to the frequency of BiV pacing. Although there was echocardiographic evidence of LVH in 158 subjects (80%), ECG criteria were only present in 16 subjects (10%).
Dynamic ST Depression (n = 144)
Dynamic ST depression was associated with the highest odds/hazard ratio from the previous studies. 17 It was quite common in this cohort, occurring in almost half of those in whom it could be assessed (n = 69, 48%).
Min HR, PVCs, QRSd, HR Variability (n = 141)
The average minimum HR was 52 ± 10 bpm (range, 22–91), with 12 subjects (9%) having a minimum HR ≥65 bpm. A prolonged QRSd (>110 ms) was present in two thirds of the subjects (n = 94, 67%) and frequent PVCs occurred in 62 (44%). At least 1 of the 3 high‐risk thresholds for HRV (SDNN, rmsSD or rr50) was exceeded in 22 subjects (16%).
Prolonged QTc and Steep QT/RR Slope (n = 130)
QTc prolongation was present in 32 subjects (25%), and 49 (38%) had an abnormally steep QT/RR slope.
Spatial QRS‐T Angle (n = 84)
Although spatial QRS‐T angle could only be assessed in a minority of the total cohort, it was abnormal in most of them (n = 61, 73%).
Ubiquity of High‐Risk ECG Parameters
Among the entire cohort, at least one high‐risk ECG parameter was almost universally present (n = 191, 97%). The average subject had 3.4 ± 1.8 (range, 0–8) high‐risk ECG parameters among the 11.7 ± 4.5 (range, 4–15) parameters capable of being assessed (Fig. 3, left graph). Thus, there was a 34% prevalence of assessable high‐risk ECGs parameters in this population (Fig. 3, right graph). Not surprisingly given our experience with ischemic cardiomyopathy, 28 conduction delay abnormalities (prolonged QRSd and fQRS) were among the most prevalent parameters in the population, followed by arrhythmias (NSVT and PVCs; Fig. 2).
Figure 3.
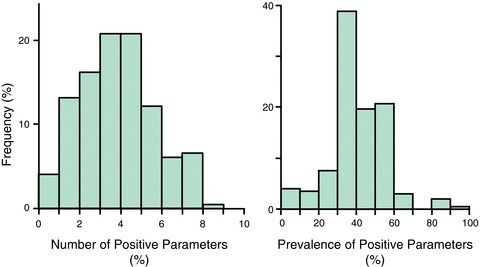
Frequency of High‐Risk ECG Parameters in PAREPET Subjects. The histogram on the left illustrates the number of positive high‐risk parameters among each of the PAREPET subjects (n = 198). Due to the frequent presence of exclusion criteria there were a variable number of high‐risk ECG parameters that could be evaluated in individual subjects. Therefore, the histogram on the right illustrates the prevalence of high‐risk positive parameters among those that could be assessed in each subject. There were 3.4 ± 1.8 high‐risk ECG parameters per subject, corresponding to a 34% frequency of positive parameters among those that could be assessed.
There were no significant correlations between the number of high‐risk ECG parameters and subjects’ age, sex, angina class, NYHA class, left ventricular end‐systolic or end‐diastolic volumes, severity of mitral regurgitation, or EF.
DISCUSSION
Assessment of ECG Parameters Associated with Cardiac Death and/or SCD
The ECG parameters evaluated in this investigation were primarily derived from large, relatively low‐risk cohorts, in which numerous exclusion criteria were applied in order to assess the parameters in all subjects. 1 , 2 , 3 , 4 , 5 , 6 Although this was useful for determining relevant risk factors in a population at large, the current study highlights the potential limitations of applying a similar approach to specific groups of patients. It is obviously unsatisfying and somewhat unrealistic to simply ignore the majority of subjects with potentially confounding exclusion criteria. However, the methodology of most prior studies has not suggested a rational approach for risk stratification when particular parameters cannot be assessed.
One progressive solution would be to more broadly apply ECG parameters to subjects with previously excluded conditions. This approach has been successfully applied to fQRS; which was initially validated in subjects with QRSd <120 ms, 29 but then subsequently shown to have predictive potential in the presence of prolonged QRSd and even ventricular pacing (with modest modifications in criteria). 12 A similar strategy is likely to be useful for including subjects with atrial fibrillation in the assessment of QRSd, QTc, QT/RR slope, and QRS‐T angle; and specific criteria, algorithms, and validation studies are currently under development.
Another appealing strategy is the use of combinations of ECG parameters, as exemplified by the Simplified ECG score. 5 This recently published approach took full advantage of digitized ECGs with automated measures to evaluate the predictive potential of 12 classic ECG abnormalities: right and LVH, right bundle branch block (RBBB) and LBBB, prolonged QRSd, Q waves, ST depression, atrial fibrillation, left atrial abnormality, right and left axis deviation, and prolonged QTc. In this large study of veterans, each ECG abnormality was more prevalent in nonsurvivors than survivors, and there was a progressive increase in cardiac mortality as a function of the number of abnormalities. Furthermore, the authors suggested that a cut‐point of five abnormalities yielded the greatest discriminatory potential. However, in contrast to the present investigation, previous validation as an independent predictor of cardiac mortality was not required of the ECG parameters included in their model. Nevertheless, both univariate and multivariate statistical analyses showed that this simple score outperformed other scoring systems including the Minnesota code, 30 Cardiac Injury Index Damage Score (CIIS), 31 and the Simplified Selvester Score. 32
Application of ECG Risk Factors in a High‐Risk Cohort
The ECG is particularly attractive for risk stratification in view of its almost universal availability and low cost; however, there are fundamental reasons why ECG parameters may be less predictive in a high‐risk cohort than a more general, low risk population. Consistent with this hypothesis, atrial fibrillation has reliably been shown to be an independent predictor of cardiac mortality in low risk groups; however, this association is reduced among those with poor LV function, and is absent in severe LV dysfunction. 33 In addition, ECG predictors of cardiac mortality may merely detect underlying heart disease, but by definition this is universally present in a high‐risk cohort. For example, the majority of subjects with ischemic cardiomyopathy in this study had abnormal parameters for infarction/scarring (fQRS) and ventricular irritability (PVCs and NSVT). Furthermore, medications commonly prescribed for cardiac patients may directly affect some ECG parameters or at least alter their predictive potential (i.e., β‐blockers effects on min HR and HR variability). Finally, since two‐thirds of deaths among patients with ischemic cardiomyopathy are attributable to a cardiac etiology, the cause‐specific mechanism of death (sudden vs nonsudden death) is a more clinically important end‐point than simply cardiac mortality.
Despite these potential limitations, the resting ECG has been shown to be useful for predicting risk of arrhythmic death and total mortality in a retrospective analysis of a high‐risk cohort. The Multicenter Unsustained Tachycardia Trial (MUSTT) enrolled patients with coronary artery disease, NSVT, and an EF <40% and reported that both arrhythmic death and total mortality could be predicted by prolonged QRSd from a nonspecific intraventricular conduction delay or LBBB (but not RBBB); and LVH was the only ECG predictor of arrhythmic death independent of total mortality. 34 However, the Multicenter Automatic Defibrillator Implantation Trial II (MADIT‐II) investigators also evaluated ECG parameters in a high‐risk cohort, and found that neither prolonged QRSd (>120 ms), LBBB, RBBB nor atrial fibrillation were associated with appropriate implantable defibrillator therapy. 35 Because the resting ECG used for these prior analyses were obtained before ICD implantation, the potentially confounding influences of ventricular pacing were avoided. However, in contrast to this study, these previous investigations were limited to evaluation of only a few parameters that could be obtained from the resting ECG in all subjects.
Study Limitations and Clinical Implications
Since the PAREPET study is ongoing, an association between ECG parameters and clinical end‐points remains to be evaluated. This reality also precludes our ability to directly evaluate the predictive potential of individual ECG parameters that would undoubtedly result in a smaller list of independent risk factors. Nevertheless, this does not diminish the novelty and potential importance of our findings regarding the frequency of ECG exclusion criteria in a high‐risk cohort (i.e., ventricular pacing, atrial fibrillation and prolonged QRSd) and the ubiquity of previously validated ECG parameters of risk.
Although the Mason‐Likar electrode configuration improves signal quality and patient comfort during ambulatory monitoring, it remains a methodological limitation because moving the limb leads from the distal limbs to the torso can alter the ECG. Comparison studies between the standard electrode placement and the Mason‐Likar configuration reveal that in particular inferior infarction diagnoses were confounded, 36 , 37 and an American Heart Association scientific statement cautions that there are differences in the ECG waveforms between the configurations. 14 , 36 Nevertheless, experts in electrocardiography have recently suggested that the standard 12‐lead ECG could be acquired with the Mason‐Likar configuration because many criteria continue to be developed from tracings obtained during invasive cardiac electrophysiology studies, exercise stress tests, and ambulatory monitoring; all of which use torso positioned limb leads. 38
In our high‐risk cohort with ischemic cardiomyopathy, only 4 of 15 previously validated ECG parameters could be assessed in all subjects. Thus, the prospective use of these or similar parameters as has been previously validated would require the exclusion of a large segment of the population. Furthermore, since nearly every subject had at least one high‐risk ECG parameter, any clinically applicable strategy will likely require a combination of parameters, which will only exacerbate the influence of exclusion criteria. Although future research will almost certainly permit the application of ECG parameters to subjects with previously excluded conditions (as discussed above), there will undoubtedly be some parameters that cannot be assessed in all subjects. Thus, creative approaches (e.g., neural networks, 39 alternate scoring strategies in subgroups, etc.) in more inclusive populations will be necessary to address this issue. It should also be acknowledged that although most interest in applying ECG parameters to high‐risk subjects has been to predict arrhythmic events for the cost‐effective targeting of ICDs, it may be equally important to identify a subgroup at high‐risk of heart failure (nonsudden) death for more aggressive medical and/or resynchronization therapy.
Acknowledgments
Acknowledgments: This study would not have been possible without the time and patience donated by our PAREPET subjects and their families. Suzanne Michalek and Brendan Heavey were instrumental in the ECG acquisition and analysis, respectively. We would like to acknowledge the technical assistance of John Gon and Wendy Klein (echocardiography), and Anne Coe for her assistance with the preparation of this manuscript.
Supported by Grants from the National Institutes of Health (K23 NR‐009716, MGC) and (RO1 HL‐076252, JMC and JAF).
REFERENCES
- 1. Engel G, Cho S, Ghayoumi A, et al Prognostic significance of PVCS and resting heart rate. Ann Noninvasi Electrocardiol 2007;12:121–129. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Goldberg R, Bengtson J, Chen Z, et al Duration of the QT interval and total and cardiovascular mortality in healthy persons (the Framingham Heart Study experience). Am J Cardiol. 1991;67:55–58. [DOI] [PubMed] [Google Scholar]
- 3. Richardson K, Engel G, Yamazaki T, et al Electrocardiographic damage scores and cardiovascular mortality. Am. Heart J 2005;149:458–463. [DOI] [PubMed] [Google Scholar]
- 4. Straus SMJM, Kors JA, De Bruin ML, et al Prolonged QTC interval and risk of sudden cardiac death in a population of older adults. J Am Coll Cardiol 2006;47:362–367. [DOI] [PubMed] [Google Scholar]
- 5. Tan SY, Sungar GW, Myers J, et al A simplified clinical electrocardiogram score for the prediction of cardiovascular mortality. Clin Cardiol 2009;32:82–86. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Yamazaki T, Froelicher VF, Myers J, et al Spatial QRS‐T angle predicts cardiac death in a clinical population. Heart Rhythm 2005;2:73–78. [DOI] [PubMed] [Google Scholar]
- 7. Moss AJ, Hall WJ, Cannom DS, et al Improved survival with an implanted defibrillator in patients with coronary disease at high risk for ventricular arrhythmia. N Engl J Med 1996;335:1933–1940. [DOI] [PubMed] [Google Scholar]
- 8. Raitt MH, Renfroe EG, Epstein AE, et al “Stable” ventricular tachycardia is not a benign rhythm : Insights from the antiarrhythmics versus implantable defibrillators (AVID) registry. Circulation 2001;103:244–252. [DOI] [PubMed] [Google Scholar]
- 9. Fallavollita JA, Luisi A Jr, Michalek SM, et al Prediction of ARrhythmic Events with Positron Emission Tomography: PAREPET study design and methods. Contemp Clin Trials 2006;27:374–388. [DOI] [PubMed] [Google Scholar]
- 10. Goldberger JJ, Cain ME, Hohnloser SH, et al American Heart Association/American College of Cardiology Foundation/Heart Rhythm Society scientific statement on noninvasive risk stratification techniques for identifying patients at risk for sudden cardiac death: A scientific statement from the American Heart Association Council on Clinical Cardiology Committee on Electrocardiography and Arrhythmias and Council on Epidemiology and Prevention. Circulation 2008;118:1497–1518. [PubMed] [Google Scholar]
- 11. Das MK, Khan B, Jacob S, et al Significance of a fragmented QRS complex versus a Q wave in patients with coronary artery disease. Circulation 2006;113:2495–2501. [DOI] [PubMed] [Google Scholar]
- 12. Das MK, Suradi H, Maskoun W, et al Fragmented wide QRS on a 12‐lead ECG: a sign of myocardial scar and poor prognosis. Circulation: Arrhythmia Electrophysiol 2008;1:258–268. [DOI] [PubMed] [Google Scholar]
- 13. Zehender M, Buchner C, Meinertz T, et al Prevalence, circumstances, mechanisms, and risk stratification of sudden cardiac death in unipolar single‐chamber ventricular pacing. Circulation 1992;85:596–605. [DOI] [PubMed] [Google Scholar]
- 14. Drew BJ, Califf RM, Funk M, et al Practice standards for electrocardiographic monitoring in hospital settings: An American Heart Association scientific statement from the Councils on Cardiovascular Nursing, Clinical Cardiology, and Cardiovascular Disease in the Young: Endorsed by the International Society of Computerized Electrocardiology and the American Association of Critical‐Care Nurses. Circulation 2004;110:2721–2746. [DOI] [PubMed] [Google Scholar]
- 15. Hancock EW, Deal BJ, Mirvis DM, et al AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part V: Electrocardiogram changes associated with cardiac chamber hypertrophy: A scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society: Endorsed by the International Society for Computerized Electrocardiology. Circulation 2009;119:e251–261. [DOI] [PubMed] [Google Scholar]
- 16. Surawicz B, Childers R, Deal BJ, et al AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part III: Intraventricular conduction disturbances a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol 2009;53:976–981. [DOI] [PubMed] [Google Scholar]
- 17. Wagner GS, Macfarlane P, Wellens H, et al AHA/ACCF/HRS recommendations for the standardization and interpretation of the electrocardiogram: Part VI: Acute ischemia/infarction a scientific statement from the American Heart Association Electrocardiography and Arrhythmias Committee, Council on Clinical Cardiology; the American College of Cardiology Foundation; and the Heart Rhythm Society endorsed by the International Society for Computerized Electrocardiology. J Am Coll Cardiol 2009;53:1003–1011. [DOI] [PubMed] [Google Scholar]
- 18. Rubulis A, Bergfeldt L, Rydén L, et al Prediction of cardiovascular death and myocardial infarction by the QRS‐T angle and T vector loop morphology after angioplasty in stable angina pectoris: An 8‐year follow‐up. J Electrocardiol 2010;43:310–317. [DOI] [PubMed] [Google Scholar]
- 19. Umetani K, Singer D, McCraty R, et al Twenty‐four hour time domain heart rate variability and heart rate: Relations to age and gender over nine decades. J Am Coll Cardiol 1998;31:593–601. [DOI] [PubMed] [Google Scholar]
- 20. Nolan J, Batin PD, Andrews R, et al Prospective study of heart rate variability and mortality in chronic heart failure : Results of the United Kingdom Heart Failure Evaluation and Assessment of Risk Trial (UK‐HEART). Circulation 1998;98:1510–1516. [DOI] [PubMed] [Google Scholar]
- 21. Schillaci G, Pucci G, Pirro M, et al Abstract 2465: QT/RR slope: A novel arrhythmogenic substrate in hypertensive left ventricular hypertrophy. Circulation 2008;118:S731. [Google Scholar]
- 22. Cygankiewicz I, Zareba W, Vazquez R, et al Prognostic value of QT/RR slope in predicting mortality in patients with congestive heart failure. J Cardiovasc Electrophysiol 2008;19:1066–1072. [DOI] [PubMed] [Google Scholar]
- 23. Rautaharju PM, Prineas RJ, Zhang Z‐M. A simple procedure for estimation of the spatial QRS/T angle from the standard 12‐lead electrocardiogram. J Electrocardiol 2007;40:300–304. [DOI] [PubMed] [Google Scholar]
- 24. Scherptong RWC, Henkens IR, Man SC, et al Normal limits of the spatial QRS‐T angle and ventricular gradient in 12‐lead electrocardiograms of young adults: Dependence on sex and heart rate. J Electrocardiol 2008;41:648–655. [DOI] [PubMed] [Google Scholar]
- 25. Schiller N, Shah P, Crawford M, et al Recommendations for quantitation of the left ventricle by two‐dimensional echocardiography. American Society of Echocardiography committee on standards, subcommittee on quantitation of two‐dimensional echocardiograms. J Am Soc Echocardiogr 1989;2:358–367. [DOI] [PubMed] [Google Scholar]
- 26. Gottdiener JS, Bednarz J, Devereux R, et al American Society of Echocardiography recommendations for use of echocardiography in clinical trials: A report from the American Society of Echocardiography's Guidelines and Standards Committee and the task force on echocardiography in clinical trials. J Am Soc Echocardiogr 2004;17:1086–1119. [DOI] [PubMed] [Google Scholar]
- 27. Lang RM, Bierig M, Devereux RB, et al Recommendations for chamber quantification. Eur J Echocardiogr 2006;7:79–108. [DOI] [PubMed] [Google Scholar]
- 28. Carey MG, Luisi AJ, Baldwa S, et al The Selvester QRS Score is more accurate than Q waves and fragmented, QRS complexes using the Mason‐Likar configuration in estimating infarct volume in patients with ischemic cardiomyopathy. J Electrocardiol 2010;43:318–325. [DOI] [PMC free article] [PubMed]
- 29. Das MK, Zipes DP. Fragmented QRS: A predictor of mortality and sudden cardiac death. Heart Rhythm 2009;6:S8–S14. [DOI] [PubMed] [Google Scholar]
- 30. Prineas R, Crow R, Blackburn H. The Minnesota Code Manual of Electrocardiographic Findings. Boston , MA , John Wright PSG Inc, 1982. [Google Scholar]
- 31. Rautaharju P, Warren J, Jain U, et al Cardiac infarction injury score: An electrocardiographic coding scheme for ischemic heart disease. Circulation 1981;64:249–256. [DOI] [PubMed] [Google Scholar]
- 32. Selvester R, Collier C, Pearson R. Analog computer model of the vectorcardiogram. Circulation 1965;31:45–53. [DOI] [PubMed] [Google Scholar]
- 33. Pai RG, Varadarajan P. Prognostic significance of atrial fibrillation is a function of left ventricular ejection fraction. Clin Cardiol 2007;30:349–354. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Zimetbaum PJ, Buxton AE, Batsford W, et al Electrocardiographic predictors of arrhythmic death and total mortality in the multicenter unsustained tachycardia trial. Circulation 2004;110:766–769. [DOI] [PubMed] [Google Scholar]
- 35. Singh JP, Hall WJ, McNitt S, et al Factors influencing appropriate firing of the implanted defibrillator for ventricular tachycardia/fibrillation: Findings from the Multicenter Automatic Defibrillator Implantation Trial II (MADIT‐II). J Am Coll Cardiol 2005;46:1712–1720. [DOI] [PubMed] [Google Scholar]
- 36. Pahlm O, Haisty WK, Jr. , Edenbrandt L, et al Evaluation of changes in standard electrocardiographic QRS waveforms recorded from activity‐compatible proximal limb lead positions. Am J Cardiol 1992;69:253–257. [DOI] [PubMed] [Google Scholar]
- 37. Sevilla DC, Dohrmann ML, Somelofski CA, et al Invalidation of the resting electrocardiogram obtained via exercise electrode sites as a standard 12‐lead recording. Am J Cardiol 1989;63:35–39. [DOI] [PubMed] [Google Scholar]
- 38. Drew BJ. The standard 12‐lead electrocardiogram: Is the standard wrong? J Electrocardiol 2007;40:380–381. [Google Scholar]
- 39. Perez MV, Dewey FE, Tan SY, et al Added value of a resting ECG neural network that predicts cardiovascular mortality. Ann Noninvas Electrocardiol 2009;14:26–34. [DOI] [PMC free article] [PubMed] [Google Scholar]