

Abstract
We report an unusual case of a foreign body removed from the urinary bladder of a 63-year-old male which mimicked a parasitic worm. The foreign body was identified as an artificial fishing worm by morphological comparison to a similar commercially produced product and by infrared spectrum analysis.
CASE REPORT
A63-year-old male presented to his urologist with complaints of sudden-onset urinary urgency, pelvic pain, and dysuria with decreased force of his urinary stream. He had had four suspected urinary tract infections in the past 12 months. Prior urine cultures had grown Escherichia coli, and his symptoms had improved following treatment with antibiotics. A physical examination, including genital and prostate examinations, revealed no abnormalities. A urine test strip was positive for blood, leukocytes, trace protein, and nitrite. An ultrasound postvoid residual procedure performed in the office demonstrated minimal residual urine but revealed calcifications within the bladder. His urine was sent for culture, and he was prescribed sulfamethoxazole and trimethoprim double strength and scheduled for an outpatient cystoscopy.
At cystoscopy, a large calculus which filled the entire bladder was visualized. A computed tomography (CT) scan of the pelvis was performed to further characterize the calculus (Fig. 1). The CT scan demonstrated a large spiral-shaped tubular calcific structure, measuring up to 7.0 by 5.2 cm in overall dimensions, within the urinary bladder. Mild thickening of the bladder wall and a streak artifact due to left hip arthroplasty were noted.
Fig 1.

CT scan of the pelvis, demonstrating a large spiral-shaped tubular calculus within the urinary bladder (arrow).
An open cystolithotomy was performed, and the extracted bladder calculus was submitted to the Metals Laboratory at the Mayo Clinic in Rochester, MN, for bladder stone analysis. Analysis of the 8.7 g of crystals removed from the specimen demonstrated a composition of 90% ammonium urate and 10% uric acid. During processing, the core of the calculus was noted to consist of two soft, gelatinous tubular structures resembling a worm. Therefore, the specimen was transferred to the Parasitology Laboratory at the Mayo Clinic in Rochester, MN, for further identification. Upon receipt, the specimen was noted to be yellow-green to black and cylindrical and to have annular circumferential ridges. It had previously been bisected; the reconstructed object measured approximately 16 cm in total length by 1.3 cm in greatest width.
On cut sectioning, the specimen revealed a gelatinous cut surface from which a minute amount of clear fluid could be expressed. Microscopic examination of touch preparations obtained from the cut surface and the expressed fluid revealed occasional sloughed urothelial cells and numerous polymorphic bacteria and yeasts. No helminth eggs were detected.
On longitudinal sectioning, there was an apparent absence of grossly discernible internal structures. This finding, in addition to the lack of expressed eggs and the uniform-appearing gelatinous cut surface, raised suspicion that the specimen was a nonorganic foreign body. Fortuitously present in the laboratory was a rubber fishing worm (Tiki-Stick, Pearl; Wave Industries, Lake Fork, TX) (5 in. in length) which had been stored in saline solution for approximately 3 years as part of an educational collection. The external and internal appearances of the artificial worm and the patient specimen were compared and found to be remarkably similar (Fig. 2). Comparison to an artificial worm contained within the original packaging provided a reference point for alterations that could occur during 3 years of immersion in fluid (Fig. 2).
Fig 2.
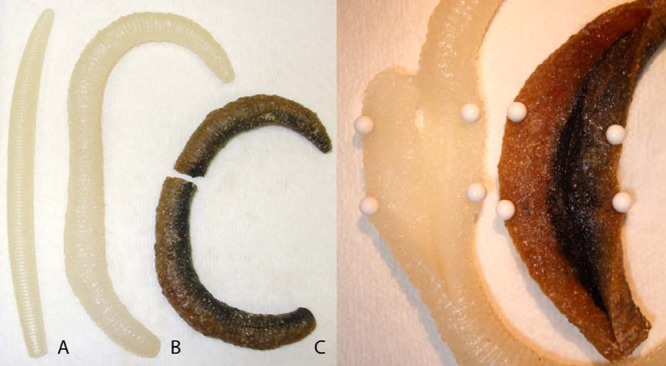
(Left) Artificial worms: A, fresh from the package; B, after immersion in saline solution for 3 years; C, patient specimen. (Right) Internal structure of the artificial worm after immersion in saline solution for 3 years (left) and the patient specimen (right).
In an effort to further elucidate the nature of the specimen, infrared spectrum (IR) analysis was conducted by comparing sections of the patient specimen to sections of the artificial fishing worm. The IR spectra of the reference artificial fishing worm and the patient sample (foreign body) were indistinguishable, suggesting that the carbon polymers used to create the two samples were virtually identical (Fig. 3).
Fig 3.

IR spectra of the patient sample compared to the IR spectra of an artificial fishing worm.
At the patient's postoperation follow-up appointment, the nature of the foreign body was discussed. He later admitted to his urologist that he had self-inserted an artificial worm into his urethra approximately 3 years earlier. However, he felt certain that it had been removed at that time and not retained in the bladder.
The presence of foreign bodies within the bladder is well documented in the medical literature (14). They are generally inserted by the patient via the urethra for purposes of erotic stimulation, curiosity, or psychiatric illness; alternatively, the source may be iatrogenic, such as retained or migrating medical devices (5, 9). Infrequently, trauma may also introduce foreign bodies, such as bullets, into the bladder (6, 8). Bladder calculus formation around intravesicular foreign bodies, particularly around migrating intrauterine devices, is well documented (1, 10). Patients with bladder calculi are frequently asymptomatic but may present with urinary retention, renal colic, and recurrent urinary tract infections (7). In a previous retrospective study of patients undergoing surgical therapy for bladder calculi, the most common organisms isolated from preoperative urine cultures were Escherichia soli, Klebsiella, and Streptococcus. Enterococcus faecalis, Pseudomonas aeruginosa, Citrobacter, and Proteus mirabilis were isolated less frequently (7).
In addition to that of foreign bodies, the chief differential diagnosis in this case was the parasitic giant kidney worm, Dioctophyma renale. While primarily a parasite of dogs, infection can occur in humans following ingestion of undercooked fish or frogs (3). The worm usually resides in the right kidney; however, migration to other body sites, such as expulsion of worms through the urethra, presumably through the bladder, has been documented as well (13). Another parasitic consideration is Ascaris lumbricoides, which has been documented to cause infections of the urogenital system, including the kidney (2, 12) and bladder (11). A. lumbricoides has also been reported as the likely nidus for formation of a bladder calculus (4).
The specimen bore a close resemblance to the common earthworm, particularly because it appeared to have similar annular ridges. Earthworms may at times be mistaken for parasites and are frequently submitted to the parasitology laboratory for identification. An earthworm of this size, however, would most likely be mature and feature a clitellum, a distinct band-like structure used in sexual reproduction which is typically located at a point distant from the head by approximately 1/3 of the overall length. While the clitellum is often reproduced in earthworm-shaped commercial fishing lures, it was not present in the patient sample or the artificial fishing worm laboratory sample. There have been no documented cases of earthworms causing parasitic infections in the literature, and those submitted to the laboratory have invariably been recovered from an external source.
In conclusion, we report an unusual case of a foreign body within the urinary bladder which mimicked a parasitic worm. The nature of the foreign body in this case, an artificial fishing worm, presented a unique challenge to the parasitology laboratory. The specimen was not easily identifiable as a foreign object and in fact was manufactured to simulate a living organism. The fortuitous presence of a similar artificial fishing worm in the laboratory allowed a detailed external and internal comparison as well as side-by-side analysis of polymer structures using infrared spectra. The most likely route of entry was self insertion through the urethra into the bladder by the patient.
Footnotes
Published ahead of print 25 April 2012
REFERENCES
- 1. Dar LA, Khan PS, Mushtaque M. 2011. Giant calculus formation after migration of an intrauterine device into the urinary bladder. Int. J. Gynaecol. Obstet. 113:243 doi:10.1016/j.ijgo.2011.01.004 [DOI] [PubMed] [Google Scholar]
- 2. Fagan JJ, Prescott CA. 1993. Ascariasis and acute otitis media. Int. J. Pediatr. Otorhinolaryngol. 26:67–69 [DOI] [PubMed] [Google Scholar]
- 3. Garcia LS. 2007. Dioctophyme renale, p 487–488 In Garcia LS. (ed), Diagnostic medical parasitology, 5th ed ASM Press, Washington, DC [Google Scholar]
- 4. Garyali RK, Gupta TR, Nagar RK. 2005. Ascaris lumbricoides: a nidus for urinary bladder stone (a case report). Rural Surg. 4:8–9 [Google Scholar]
- 5. Johnin K, Kushima M, Koizumi S, Okada Y. 1999. Percutaneous transvesical retrieval of foreign bodies penetrating the urethra. J. Urol. 161:915–916 [PubMed] [Google Scholar]
- 6. Halkic N, Wisard M, Abdelmoumene A, Vuilleumier H. 2001. A large bullet in the bladder. Swiss Surg. 7:139–140 [DOI] [PubMed] [Google Scholar]
- 7. Hammad FT, Kaya M, Kazim E. 2006. Bladder calculi: Did the clinical picture change? Urology 67:1154–1158 [DOI] [PubMed] [Google Scholar]
- 8. Kiliç D, Kilinc F, Ezer A, Guvel S. 2004. Spontaneous expulsion of a bullet via the urethra. Int. J. Urol. 11:576–577 [DOI] [PubMed] [Google Scholar]
- 9. Ko PC, Lin YH, Lo TS. 2011. Intrauterine contraceptive device migration to the lower urinary tract: report of 2 cases. J. Minim. Invasive Gynecol. 18:668–670 [DOI] [PubMed] [Google Scholar]
- 10. Ozçelik B, Serin IS, Basbug M, Aygen E, Ekmekcioglu O. 2003. Differential diagnosis of intra-uterine device migrating to bladder using radiographic image of calculus formation and review of literature. Eur. J. Obstet. Gynecol. Reprod. Biol. 108:94–96 [DOI] [PubMed] [Google Scholar]
- 11. Singh D, Vasudeva P, Dalela D, Sankhwar SN. 2010. Ascaris lumbricoides: a stranger in the urinary bladder causing urinary retention. J. Postgrad. Med. 56:222–223 [DOI] [PubMed] [Google Scholar]
- 12. Taylor KL. 1995. Ascariasis of the kidney. Pediatr. Pathol. Lab. Med. 15:609–615 [DOI] [PubMed] [Google Scholar]
- 13. Tuur SM, et al. 1987. Liesegang rings in tissue. How to distinguish Liesegang rings from the giant kidney worm, Dioctophyma renale. Am. J. Surg. Pathol. 11:598–605 [PubMed] [Google Scholar]
- 14. van Ophoven A, deKernion JB. 2000. Clinical management of foreign bodies of the genitourinary tract. J. Urol. 164:274–287 [DOI] [PubMed] [Google Scholar]