

Abstract
We present a rare case of a symptomatic acquired large coronary fistula and aneurysm secondary to chest trauma that was successfully closed using stent graft. This case is followed by review of the literature.
Keywords: coronary artery fistula

Case Report
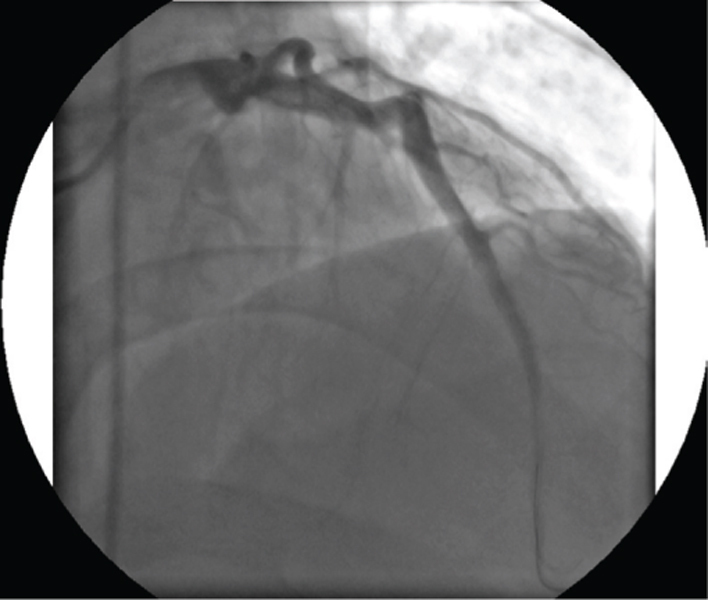
A 30-year-old man suffering from a penetrating stab wound to his mid-left-anterior chest wall underwent left lateral thoracotomy at the fourth intercostal space to repair his chest wall injury. No clear cardiac injury was identified at that time. After surgery, the patient developed increasing exertional angina that limited his activities. He was referred for further evaluation 5 months after his trauma due to persistent symptom. His physical exam was remarkable for a loud grade III/IV continuous murmur that was heard at left sternal border. ECG was normal. Chest X-ray showed mild cardiac enlargement. Coronary angiography revealed a large coronary pseudoaneurysm and fistula originating from mid left anterior descending artery (LAD) connecting to the right ventricular cavity (Figures 1 and 2). Distal LAD after the fistula was very small due to poor distal flow. The decision was made to close the fistula using a stent graft.
Figure 1.
Large fistula and pseudoaneurysm can be seen in mid left anterior ascending artery.

Figure 2.
Large fistula can be seen orginating from mid left anterior ascending artery.

The left main coronary artery was engaged using a JL3.5 guiding catheter. After wiring the LAD, a 3-mm x 20-mm compliant balloon was inflated at the side of the fistula to determine successful closure with contrast injection during balloon inflation. Next, a 3-mm x 26-mm coronary GraftMaster stent was implanted at the aneurysm neck level, followed by balloon dilatation using a 3-mm x 18-mm Sapphire balloon. The aneurysm was completely sealed after stenting, with restoration of normal flow into the distal LAD (Figure 3). The patient tolerated the procedure and remains asymptomatic during follow-up visits.
Figure 3.
Succesfull closure of the fistula and pseudoaneurysm after stent graft deployment in mid LAD.
Discussion
Large coronary artery fistulas are rare, and the true incidence is difficult to discern as a great number of them are asymptomatic. At least 75% of coronary artery fistulas are small and clinically silent. Most are congenital while some are acquired, as was the case presented herein. Coronary fistulas cause blood flow to be shunted into cardiac chambers, great vessels, or other structures, bypassing the myocardial capillary network. Symptoms may be caused by either coronary steal or a high left to right shunt flow. In symptomatic patients, closure of the fistula should be considered.1
Physical examination is normal in typical patients. In the case of a very large fistula, a widened pulse pressure may be detected, and a continuous murmur may be heard similar to our case. On rare occasions, thoracic trauma can lead to coronary artery fistula. In our case, coronary fistula occurred in the setting of a stab wound penetrating the chest. Trauma-related coronary fistulas usually are connected to right-sided heart structures. In large fistulas similar to our case, coronary steal is the presumed cause of symptoms.
The best management of a coronary artery fistula secondary to penetrating trauma is not known. Therapeutic options consist of surgical or endovascular repair. Although surgical approach has been described as a gold standard for coronary artery fistula closure, endovascular treatment has recently been advocated as a less invasive procedure and is more acceptable to patients.2, 3 Various percutaneous devices are available including detachable balloon, coil embolization, and graft stents.2, 4-6 Due to the presence of a large pseudoaneurysm, the use of a stent graft appeared to be the best approach in this patient.
Conflict of Interest Disclosure: All authors have completed and submitted the Methodist DeBakey Cardiovascular Journal Conflict of Interest Statement and none were reported.
Funding/Support: The authors have no funding disclosures.
References
- 1.Estep JD, Shah DJ, Nagueh SF, Mahmarian JJ, Torre-Amione López -Candales A, Kumar V. Coronary artery to left ventricle fistula. Cardiovasc Ultrasound. 2005;3:35.. doi: 10.1186/1476-7120-3-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kassaian SE, Mahmoodian M, Salarifar M, Alidoosti M, Abbasi SH, Rasekh A. Stent-graft exclusion of multiple symptomatic coronary artery fistulae. Tex Heart Inst J. 2007;34(2):199–202. [PMC free article] [PubMed] [Google Scholar]
- 3.Mudawi TO, Morrison L. Percutaneous closure of a traumatic fistula between the right coronary artery and the right atrium in a young adult: a new covered stent strategy. J Invasive Cardiol. 2009 Aug;21(8):E161–163. [PubMed] [Google Scholar]
- 4.Dorros G, Thota V, Ramireddy K, Joseph G. Catheter-based techniques for closure of coronary fistulae. Catheter Cardiovasc Interv. 1999 Feb;46(2):143–50. doi: 10.1002/(SICI)1522-726X(199902)46:2<143::AID-CCD6>3.0.CO;2-E. [DOI] [PubMed] [Google Scholar]
- 5.Goldberg SL, Makkar R, Duckwiler G. New strategies in the percutaneous management of coronary artery fistulae: A case report. Catheter Cardiovasc Interv. 2004 Feb;61(2):227–232. doi: 10.1002/ccd.10758. [DOI] [PubMed] [Google Scholar]
- 6.Latson LA. Coronary artery fistulas: how to manage them. Catheter Cardiovasc Interv. 2007 Jul 1;70(1):110–6. doi: 10.1002/ccd.21125. [DOI] [PubMed] [Google Scholar]