

Abstract
Pdx1 is a key transcription factor involved in the regulation of insulin gene expression that is expressed at high levels in the β-cells of the pancreatic islets. We asked whether Pdx1 is a target of anti-islet autoimmunity in Type 1 diabetes (T1D). Pdx1 autoantibodies (PAA) were detected in non-obese diabetic (NOD) mice using ELISA, Western blotting, and radioimmunoprecipitation of [35S]-labeled insulinoma cell line-derived Pdx1 protein. PAA were detected as early as at 5 weeks of age, and generally peaked before the onset of clinically overt diabetes in diabetes-prone female NOD mice. Levels declined substantially after diabetes onset. PAA were not detected in the sera of NOD-scid, C57BL/6 or BALB/c mice. The titers of PAA in NOD mouse sera were as high as 1/93750 by ELISA. The fine specificity of PAA was determined by Western blotting using a series of truncated recombinant Pdx1 proteins. The immunodominant epitopes were located to the Pdx1 C-terminus (p200-283) in NOD mice. PAA also were detected in sera from human T1D patients, but the major epitopes were localized to amino acids 159-200 as well as the same region (p200-283) recognized by PAA from NOD mice. Using [3H]-thymidine incorporation, the p83 fragment of Pdx1 specifically stimulated proliferation of splenic T-cells from recent-onset diabetic NOD mice. The presence of PAA in prediabetic NOD mice and human T1D patients and Pdx1-specific T-cell proliferation in NOD mice provide a strong rationale for further investigation of the pathogenic role of immune responses against Pdx1 in T1D.
Type 1 diabetes (T1D) is an autoimmune disease characterized by the development of autoantibodies and destructive T cell infiltration of insulin-producing islet β cells (1). Several candidate autoantigens have been identified and autoantibody production may precede disease in family members of T1D patients and other individuals at risk for developing T1D (2-5). The non-obese diabetic (NOD) mouse is an important animal model of autoimmune diabetes (6;7). Disease occurs spontaneously and shares many phenotypic and genetic similarities with T1D in humans (6;7). Lymphocyte infiltration of the islets of Langerhans begins at 4 weeks of age, progressing from periinsulitis to severe insulitis by 10 weeks of age (6;7). Diabetes onset typically ensues at 12–14 weeks in female NOD mice. To date there is no effective immunotherapy to treat or prevent human T1D (5;8-10).
We have previously shown that treatment of streptozotocin (Stz)-induced murine diabetes with recombinant Pdx1 protein (rPdx1) reverses diabetes by stimulating beta cell regeneration and liver cell reprogramming into insulin-producing cells (11). It has been reported that in NOD mice treated with Pdx1 delivered by an adenovirus vector, the autoimmune attack on the pancreatic islets can be downregulated (12). Recently, we found that treatment of prediabetic female NOD mice with rPdx1 or with a non-functional mutant Pdx1 protein prevented the onset of diabetes (unpublished observation). In view of the modulation of diabetes by this mutant protein, in the present study we tested the hypothesis that Pdx1 might be an autoantigen relevant to pathogenesis of T1D in NOD mice. Our data indicate that Pdx1 is a novel β-cell specific autoantigen that stimulates an antigen-specific T-cell response and is recognized by autoantibodies present in serum samples from both prediabetic and diabetic NOD mice and a subset of T1D patients. High levels of Pdx1 autoantibodies (PAA) were detected in young NOD mice and the peak of PAA often occurred prior to the onset of diabetes.
RESEARCH DESIGN AND METHODS
Serum samples and animals
Serum samples were collected from female NOD mice and congenic non-diabetic NOD-scid, BALB/c, and C57BL/6 mice (Jackson Laboratory, Bar Harbor, ME). Mice were housed in an SPF facility at the University of Florida. Serum samples from female NOD mice were tested for PAA at ages ranging from 5-25 weeks. Blood glucose was determined weekly starting at 10 weeks of age. Collection of serum samples from human subjects was approved by the Institutional Review Boards and all animal experiments were approved by the Institutional Animal Care and Use Committee of the University of Florida.
Preparation of recombinant Pdx1, mutant Pdx1, and truncated proteins
Complementary DNA fragments of rat or human Pdx1 were inserted into the expression vector pET28 (Invitrogen, Carlsbad, CA) and 6X histidine-tagged recombinant Pdx1, mutant Pdx1 lacking the protein transduction domain (Pdx1ΔPTD), and truncated Pdx1 proteins were produced, purified, and characterized as previously described (11). In brief, C-terminal Pdx1 truncations were generated by site-directed mutagenesis using a QuikChange kit (Stratagene) by introducing a stop codon (TAG) mutation into rat Pdx1 cDNA at amino acid position 120, 160, or 200. The mutant cDNAs were verified by DNA sequence analysis. Three truncated Pdx1 fragments (1-119, 1-159, and 1-199) were expressed in the pET28 expression vector in E. coli BL21(DE3) cells and purified by Ni-NTA affinity chromatography as described (11).
Expression and purification of GST-p83 and GST-p40
Rat Pdx1, amino acids 200-283 (p83) and Pdx1, amino acids 160-199 (p40) were expressed in E. coli as fusion proteins to glutathione-S-transferase (GST). A fragment of the cDNA encoding the amino acids 200–283 or 160-199 of Pdx1 was amplified by PCR and ligated into the BamHI/XhoI sites of pGEX 5x-1 expression vector (Promega) for generating fusion proteins GST-p83 and GST-p40, respectively. A 6X histidine tag was attached to the N-terminus of GST-p40 to facilitate purification of this insoluble protein. The plasmids were transformed into E. coli BL21 (DE3) cells and the fusion proteins were produced as described (11). GST and GST-p83 fusion proteins were purified using a glutathione-Sepharose affinity purification kit (Pierce, Rockford, IL). Bound protein was eluted with 10 mM reduced glutathione in 50 mM Tris–HCl (pH 8.0) and dialyzed against PBS. GST-p40 was purified by Ni-NTA affinity chromatography under denaturing conditions as described (11). Protein concentration was determined and the purified proteins were snap frozen and stored in aliquots at -80°C as described (11).
SDS-PAGE and Western blot
Pdx1 and its truncated forms were separated by 12% SDS-polyacrylamide gel electrophoresis and transferred onto nitrocellulose membranes (Bio-Rad). Blots were probed with mouse or human sera or with rabbit anti-Pdx1 antibodies (1:1000) as described (11) (13) with slight modifications. The membrane was blocked with 5% nonfat dry milk (Bio-Rad) in Tris buffered saline (TBS) pH 7.5 (Bio-Rad), and then incubated with sera from mice (1:1500 dilution) or human type 1 diabetes patients (1:200 dilution) overnight at 4°C. After washing five times with TBS containing 0.1% Tween-20, the membrane was incubated with horseradish peroxidase (HRP)-conjugated goat anti-mouse-IgG (1:4000, Abcam, Cambridge, MA) or anti-human IgG (1:2000, South Biotech) for 30 min at 22°C. Binding was detected by chemiluminescence (Amersham, Piscataway, NJ).
ELISA for autoantibodies against Pdx1
Autoantibodies against Pdx1 were quantified by ELISA. In brief, a microtiter plate (Nunc MaxiSorp, Fisher) was coated with 100 μl of rPdx1 (10 μg/ml) overnight at 4°C. After washing the plate three times with PBS, the plate was incubated with 200 μl of 5% dry milk in PBS (blocking buffer) for 1 h. Next, mouse sera were added in duplicate at a 1:30 dilution or after serial dilutions in blocking buffer for 1 h. The bound antibodies were incubated with HRP-conjugated goat anti-mouse IgG antibodies (1:4000 in blocking buffer, Abcam) or HRP-goat-anti-mouse IgG isotype-specific antibody kit (IgG1, IgG2a, IgG2b, and IgG3 specific, from Santa Cruz Biotechnology, Inc, Santa Cruz, CA) for 1 h at 22°C. After washing 5 times, the plate was incubated with 100 μl of substrate solution (BD OpfEIA™, BD Biosciences Pharmingen, San Diego, CA) and developed at 22°C for 10 min. The reaction was terminated by adding 50 μl of 4M H2SO4, and absorbance was determined at 450 nm. A positive result was defined as an OD450nm ≥ 0.1 (the mean of BALB/c sera or istotype controls + 3 S.D.). Intra- and inter-assay variation (C.V.%) was determined with the same lot of ELISA plates and the same serum positive and negative samples.
[35S]-labeling and immunoprecipitation
Rat insulinoma INS-1 cells (clone 832/13, a gift from Christopher B. Newgard, Duke University) were metabolically labeled overnight with [35S] methionine plus [35S] cysteine (GE Healthcare, Piscataway, NJ) as described (14). [35S]-labeled INS-1 cell lysate containing rat Pdx1 protein (200 μl volume, 106 cell equivalents) were incubated with preformed complexes of immunoglobulin/protein A/G-Sepharose for 2 h at 4°C. Protein A/G-Sepharose was incubated with 10 μl of mouse sera or Pdx1-treated mouse serum (made in our lab) overnight. After centrifuging, 20 μl of 50% protein A/G Sepharose beads (Pharmacia) was added followed by incubation at 22°C for 60 min. Immune complexes were collected by centrifugation and washed three times. Proteins were freed by boiling in sample buffer and analyzed on 12.5% SDS-polyacrylamide gels. The gels were stained and then fluorographed, followed by exposure to X-ray film for one week as previously described (15). Similar immunoprecipitation was performed using unlabeled INS1 cell lysates, and the immunoprecipitated Pdx1 protein from the cell lysates by the tested mouse sera was probed by Western blotting using polyclonal rabbit Pdx1 antibodies (1:2000 dilution) (11), following separation by SDS-PAGE and transferring onto nitrocellulose membranes.
T-cell proliferation assay
New onset diabetic female NOD mice were sacrificed and splenocytes were harvested. The splenocytes (106 cells/well in triplicate) were incubated for 72 h at 37°C in a humidified atmosphere with 5% CO2 in the absence or presence of various stimuli (see Results). Anti-CD3 antibody treatment was used as positive control. T-cell proliferation was quantified by incorporation of [3H] thymidine (Amersham, 1 μCi/well) for the last 24 hrs of incubation. The stimulation index (SI) was calculated as the ratio of the mean cpm of antigen or mitogen-treated cells divided by the mean cpm of control cells cultured with medium alone (12).
Statistical analysis
Statistical analysis was carried out using the two-sample Student’s t-test assuming unequal variances. A P value < 0.05 was considered significant.
RESULTS
Discovery of anti-Pdx1 autoantibodies (PAA) in NOD mouse sera
As part of a follow up study for our recently published work showing that Pdx1-treatment reverses Stz-induced diabetes in BALB/c mice (16), we investigated the effect of Pdx1 treatment in NOD mice. To examine whether daily Pdx1 treatment of NOD mice could stimulate production of anti-Pdx1 antibodies, we first established and validated an ELISA for detecting anti-Pdx1 antibodies using highly purified rat or human rPdx1 as antigen and rabbit polyclonal antibodies to Pdx1 (11) as positive control. We then tested serum samples collected from pre-treated, post-rPdx1-treated, and saline-treated (control) female NOD mice for the presence of anti-Pdx1 antibodies (Fig.1A). As expected, sera collected from 23-week-old mice treated with Pdx1 protein for 12 weeks displayed strong immunoreactivity to Pdx1 antigen consistent with a humoral immune response to rPdx1. Surprisingly, some sera from prediabetic (pretreatment) and control mice were also strongly positive. This result raised the possibility that Pdx1 might be an islet cell autoantigen in NOD mice, leading to the production of PAA.
Fig. 1. Pdx1 autoantibodies in prediabetic NOD mice.
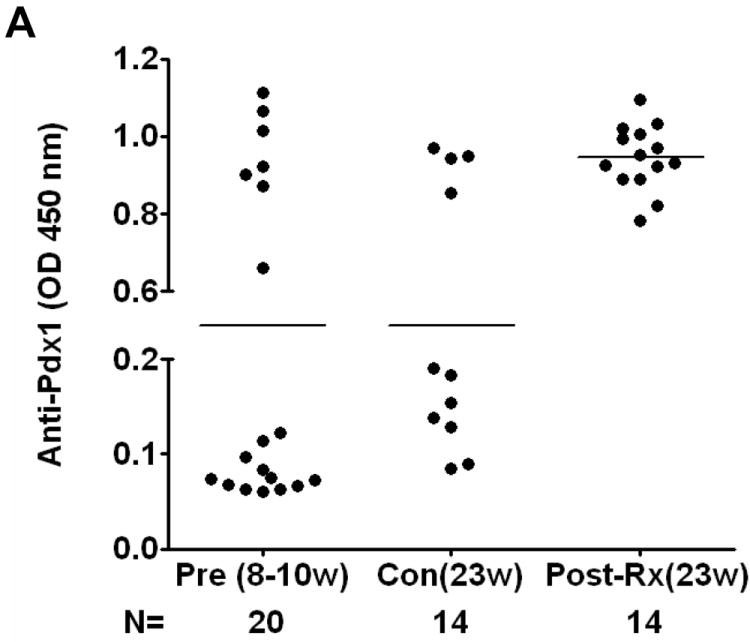
A. Detection of Pdx1 antibodies in NOD mice. Sera were collected from female NOD mice at various ages ranging from 8 to 23 weeks or NOD mice treated with daily injection of rPdx1 for 12 weeks. PAA were assayed using ELISA at a serum dilution of 1:30. Positive value is defined 3 SD above the mean of the BALB/c control sera. (Pre, pre-treatment; Con, PBS-treated controls; Post-Rx, treated with rPdx1).
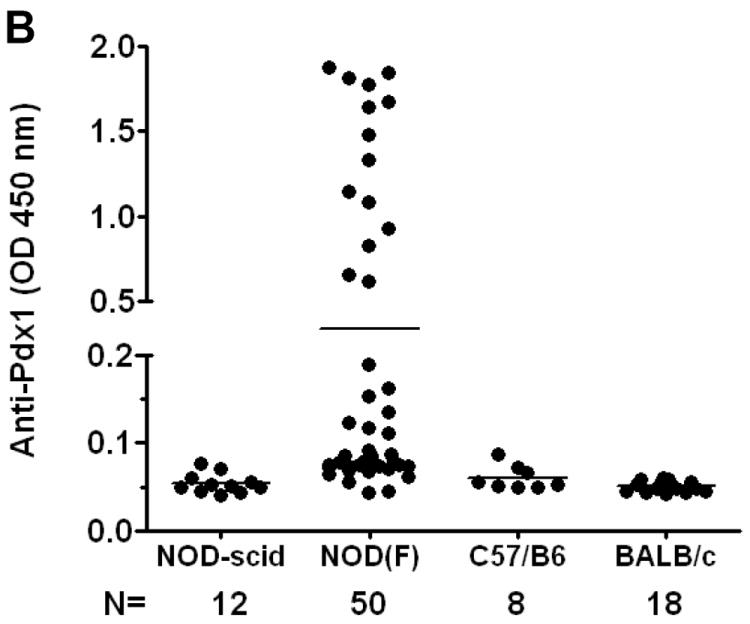
B. Comparison of PAA in various strains of mice. Sera from various mouse strains at different ages were collected and PAA were measured by ELISA and expressed as OD values at 450 nM using the 99th percentile of BALB/c control mice as the threshold definition of positivity.
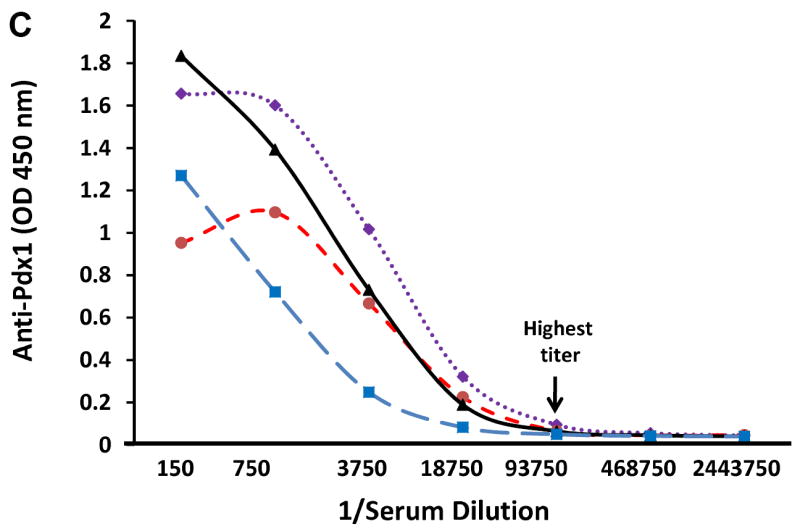
C. PAA titration curve. Selected PAA-positive serum samples at age of 10 weeks were serially diluted as indicated and OD values were determined by ELISA. Titer is defined as the last dilution giving positive OD reading above control.
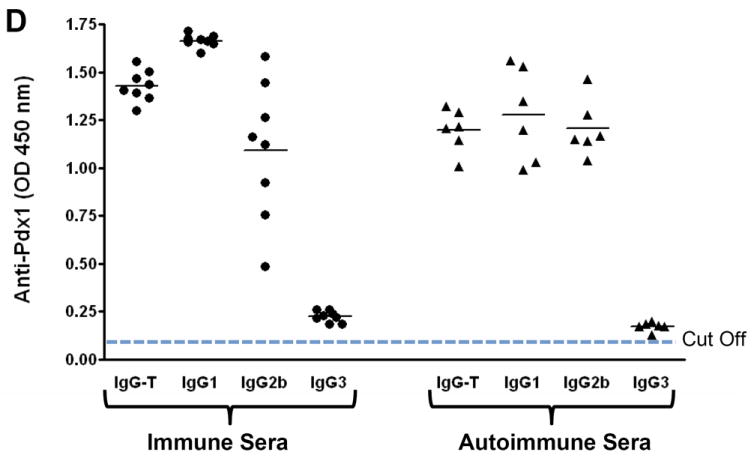
D. Isotypes of anti-Pdx1 antibodies. Total anti-Pdx1 antibody activity (IgG-T) and anti-Pdx1 antibodies of the IgG1, IgG2b, and IgG3 isotypes in sera from NOD mice immunized with Pdx1 (immune sera, solid circles) and selected PAA-positive autoimmune sera (triangle) from NOD mice were assayed by ELISA (1:30 dilution). An OD of 0.10 was used as the positive cut-off value (≥ 3 SD above the mean of the BALB/c control sera).
To test this hypothesis, we examined serum samples from several mouse strains including C57BL/6, BALB/c, and non-diabetic congenic NOD-scid mice for the presence of PAA. Figure 1B shows that 54% of pre-diabetic female NOD mice had PAA detectable at the screening dilution of 1:30, whereas no reactivity was seen in other mouse strains. These results indicated that PAA were produced selectively by prediabetic NOD mice. Serial dilution of selected positive NOD mouse sera at age 10 weeks revealed that the titers of these PAA were as high as 1:93,750 (Fig.1C). Induced anti-Pdx1 antibodies in immunized NOD mice and spontaneous antibodies in un-immunized PAA+ NOD mice consisted of a variety of isotypes (Figure 1D). IgG1 and IgG2b anti-Pdx1 antibodies predominated in the response to immunization as well as in the spontaneous response, whereas IgG3 PAA were less abundant (Fig. 1D). The levels of anti-Pdx1 IgG2b antibodies were considerably more variable in immunized mice than in the mice with spontaneous PAA. Since NOD mice express the Igh1b allele, they express IgG2c instead of IgG2a (17). Thus, anti-Pdx1 IgG2C antibody levels could not be accurately measured using the current commercial kit.
PAA also are detectable by Western blot and immunoprecipitation (IP)
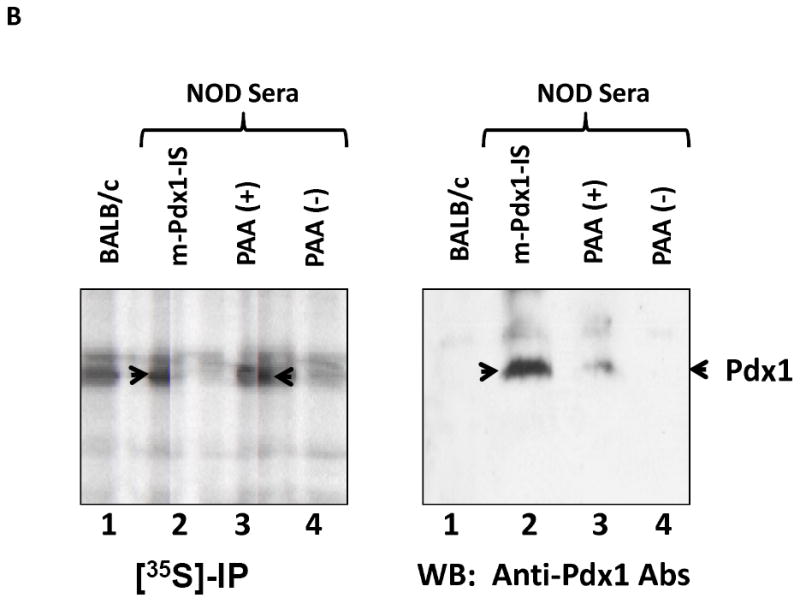
To further establish the existence of PAA in NOD mice, selected PAA-positive or negative NOD sera, negative control (BALB/c) serum, and positive control rabbit polyclonal immune serum (rPdx1-IS) were used for Western blotting using purified rat Pdx1 as antigen (Fig. 2A). ELISA-PAA positive NOD mouse sera detected a single band at 46 KDa (Lane 3), whereas ELISA-negative serum samples from BALB/c (lane 1) or NOD (lane 4) mice did not. In contrast, the immune serum (lane 2) revealed a major band at 46 KDa as well as several minor bands, possibly due to antibodies against minor proteins contaminating the Pdx1 antigen preparation used for immunization and/or degradation fragments of Pdx1. In addition, autoantibody specificity was verified by immunoprecipitating [35S]-labeled native Pdx1 from rat insulinoma INS-1 cell extracts. Figure 2B (left panel) shows a band at 46 KDa that was immunoprecipitated by both NOD-mouse Pdx1-treated serum (m-Pdx1-IS) (lane 2) and the ELISA-positive PAA serum (lane 3), whereas no clear band was detected in PAA-negative or control sera. The identity of this immunoprecipitated protein band was confirmed by Western blotting using rabbit anti-Pdx1 polyclonal antibodies to probe the membrane (Fig. 2B, right panel). Thus, PAA could be detected by Western blotting and IP in addition to ELISA.
Fig. 2. Confirmation of PAA by Western blot (A) and immpreprecipitation (B).
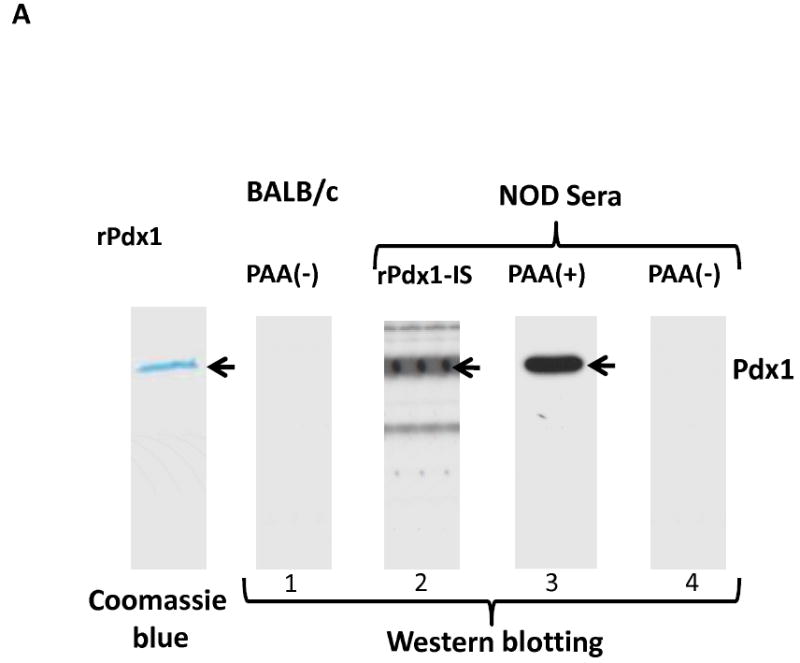
A. Western blotting. Purified recombinant rat Pdx1 protein (1 μg/lane) was separated on a 10% SDS-PAGE and stained with Coomassie blue or transferred to PVDF membrane. The membrane was probed with BALB/c or NOD mouse serum either positive (PAA+) or negative (PAA-) by ELISA, or with rabbit polyclonal anti-Pdx1 immune serum (rPdx1-IS) as positive control.
B. Immunoprecipitation and Western blotting. Rat insulinoma cells (INS-1) were labeled with [35S]-methionine overnight and cell lysate (0.5 mg) was incubated for 1 hr at 4°C with preformed immune complexes by incubating 10 μl mouse serum with 50 μl protein A/G overnight at 4°C. 35S-labelled proteins were separated by SDS-PAGE, fluorographed, and the dried gel was exposed to X-ray film at -80°C for 7 days. In parallel, unlabeled INS-1 cell lysate was subjected to immunoprecipitation with the same mouse sera. The immune complexes were separated by SDS-PAGE, transferred to PVDF membrane, and probed with rabbit anti-Pdx1 polyclonal antibodies (1:2000). Lanes 1-BALB/c, 2- Pdx1-treated NOD mouse immune serum (m-Pdx1-IS), 3-PAA(+), and 4-PAA(-) NOD serum samples. Arrow indicates position of Pdx1 protein.
PAA emerge before the onset of diabetes
To determine whether the PAA can predict disease onset, the relationship between PAA and hyperglycemia was explored (Fig. 3). Five-week-old female NOD mice (n = 20) were studied longitudinally and blood samples were taken biweekly until the onset of diabetes. Blood glucose levels were monitored weekly beginning at 10 weeks of age. PAA were first detected at 5-15 weeks of age, and their levels gradually increased, peaked, and then declined over the next 8-12 weeks. PAA often decreased to lower positive levels or disappeared completely after the onset of diabetes and the peak levels often preceded disease onset. In general, there was an inverse correlation over time between PAA levels and blood glucose levels in individual mice. However, some mice maintained high levels of the PAA after onset of diabetes. Figure 3 illustrates the relationship between levels of PAA and blood glucose in four mice. In three mice PAA peaked prior to the onset of diabetes. In the fourth mouse (m19L), low levels of PAA were seen consistently without an apparent peak; this mouse remained normoglycemic at 25 weeks. These results suggest that PAA predict the onset of type 1 diabetes in NOD mice.
Fig. 3. Relationship between PAA levels and onset of diabetes.
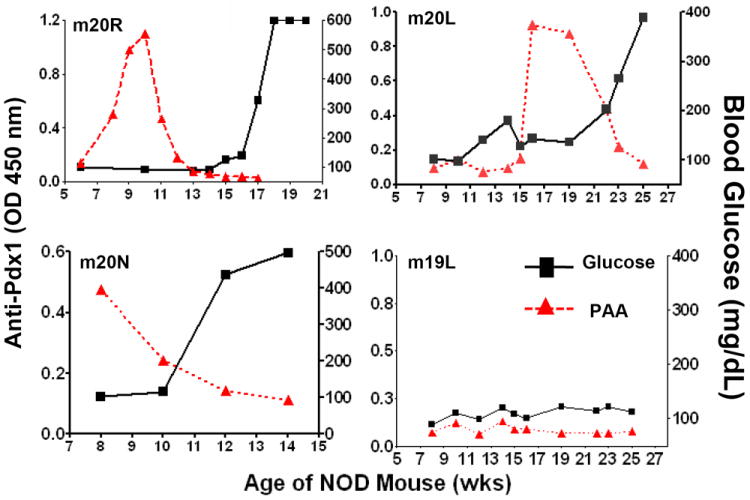
Serum samples were collected biweekly from 5 week-old NOD mice (n = 20). PAA were detected by ELISA and expressed as OD values at 450 nM. Blood glucose levels were monitored weekly via tail vein snipping. Four representative mice (m20R, m20L, m20N, and m19L) are shown here.
B-cell autoepitopes are sensitive for partial trypsin treatment
Since Western blot analysis revealed that ELISA-positive NOD mouse sera recognized primarily the full length Pdx1, we examined whether these sera might recognize a common epitope. We first partially digested the full-length rPdx1 by incubating with trypsin. As shown in Figure 4A, 10-minute digestion of Pdx1 generated multiple fragments that were stained by Coomassie blue (left panel). Interestingly, two NOD mouse samples (m2L and m7R) recognized the slowest migrating tryptic fragment of Pdx1 as well as full length Pdx1.
Fig. 4. Identification of immunodominant B-cell autoepitopes of Pdx1.
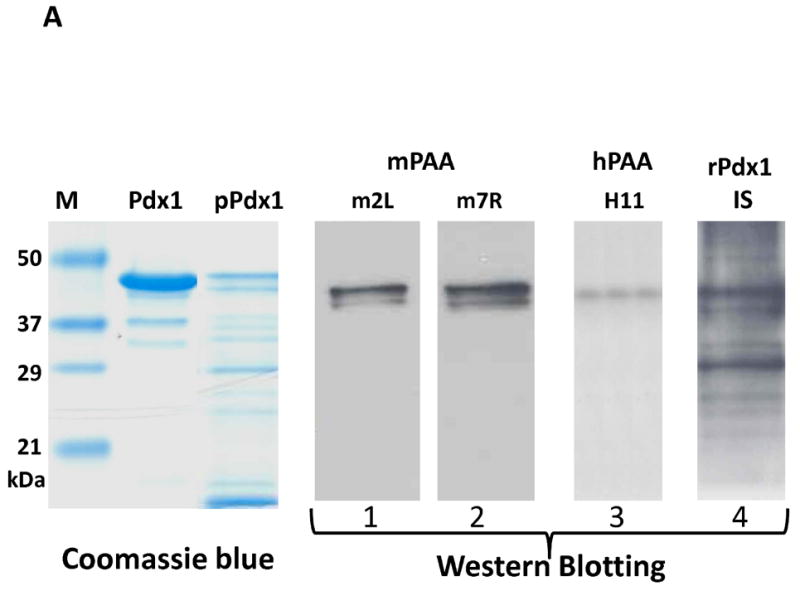
A. Partial digestion of Pdx1 and Western blotting. Pdx1 protein was partially digested with trypsin at pH 7.6 25°C for 10 min, and the digested products were separated and stained with Coomassie blue (left panel) or transferred to the membrane for blotting with two PAA(+) mouse sera (m2L & m7R, Lanes 1, 2), human PAA+ serum (h11, lane 3), or rabbit polyclonal anti-Pdx1 immune serum (lane 4).
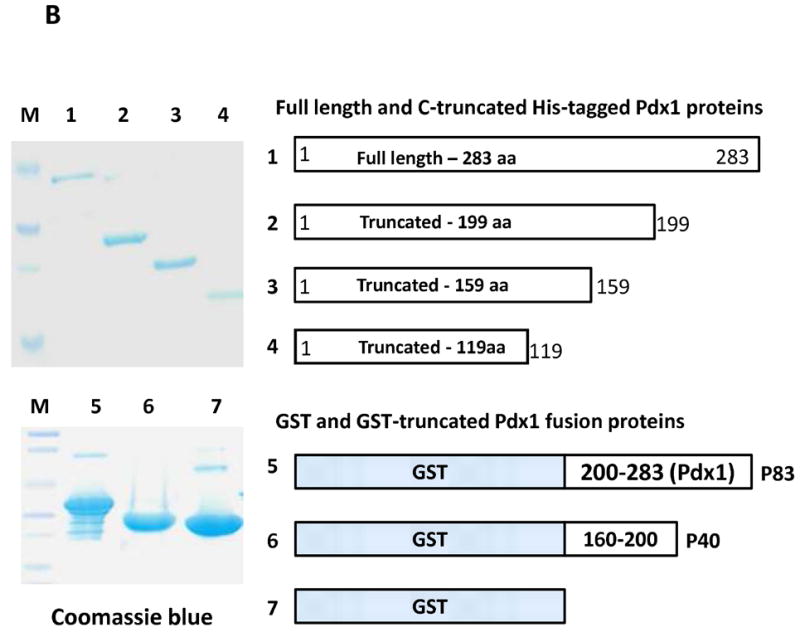
B. Expression and purification of truncated Pdx1 proteins. Full length or truncated Pdx1 proteins with an N-terminal histidine-tag were prepared as described in Methods, separated by SDS-PAGE, and stained with Coomassie blue dye (upper panel). Lanes 1-full length, 2-Pdx1 (1-199), 3-Pdx1 (1-159), and 4-Pdx1 (1-119). Lower panel shows three purified proteins GST-Pdx1 (200-283) “p83”, GST-Pdx1 (160-200) “p40”, and GST that were separated by SDS-PAGE and stained with Coomassie blue. Lanes 5-p83, 6-p40, and 7-GST.
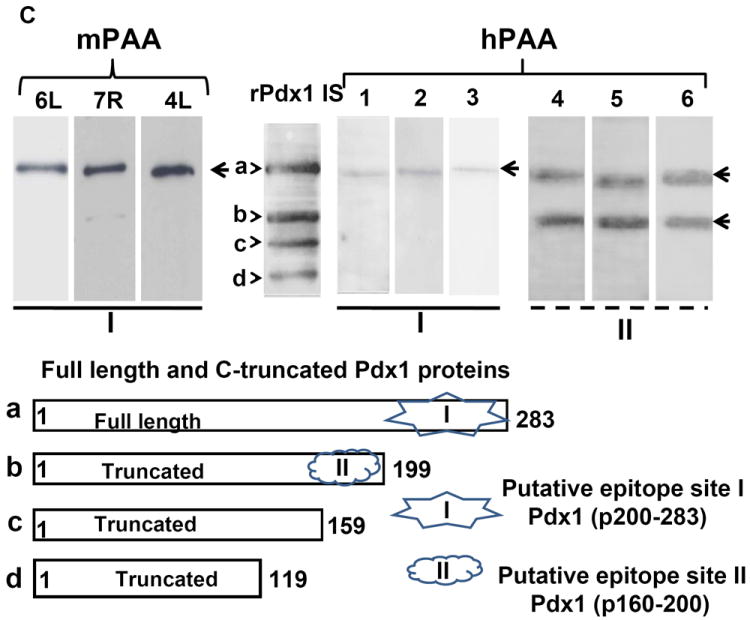
C. Identification of two dominant epitope regions using a mixture of Pdx1 proteins. Four purified proteins, Pdx1 (a) and its truncated forms (b, c, & d), were mixed at equal concentrations and used for Western blotting to detect autoantibodies. Each lane was loaded with 5 μg of mixed proteins, resolved by SDS-PAGE, transferred to PVDF membrane, and probed using three mouse PAA (+) sera (6L, 7R, and 4L) at a dilution of 1:1500, or six human PAA (+) sera (Lanes 1-6) at a dilution of 1:200. Rabbit polyclonal anti-Pdx1 immune serum (rPdx1 IS) was used as positive control at a dilution of 1:2000. Arrows indicate full length Pdx1 (a) and truncated proteins (b, c, and d). Lower panel shows the structure of Pdx1 and its truncated forms and potential autoepitope regions I & II for mouse and human PAA.
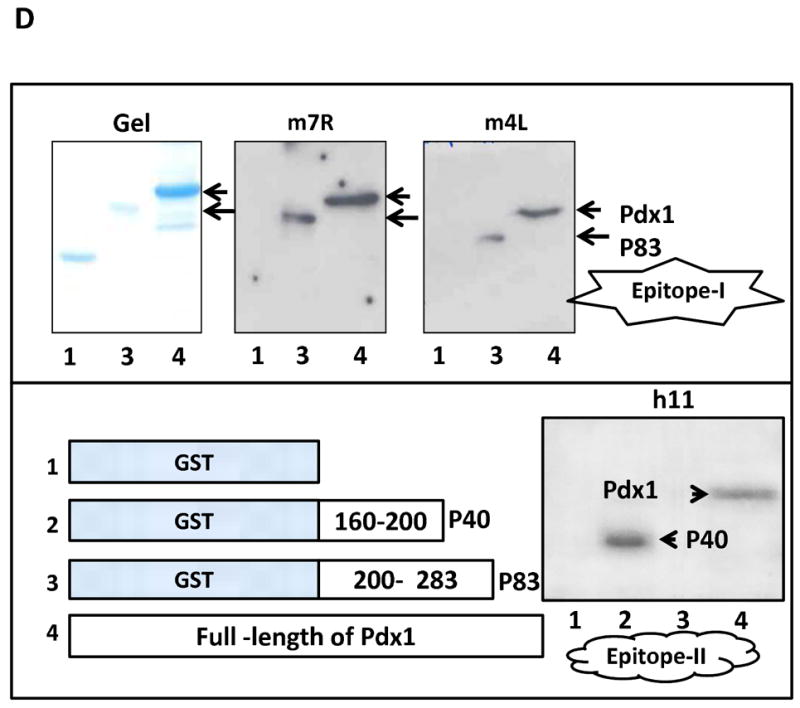
D. Confirmation of immunodominant autoepitopes. Upper left panel shows Coomassie blue staining of GST (lane 1), p83 (lane 2), and Pdx1 (lane 3). Right two panels are immunoblots using the same amount of proteins and blotted with two NOD mouse PAA (+) sera. Arrows indicate the positions of Pdx1 and p83. Lower left panel is a diagram of the four proteins (1-GST, 2-GST-p40, 3-GST-p83, and 4-Pdx1) used in this study. The lower right panel depicts an immunoblot using human h11 PAA (+) serum. Arrows indicate positions of corresponding proteins as indicated.
In addition, we also screened 37 sera from patients (n = 25) with well-established T1D or anti-insulin autoantibodies (IAA) positive individuals (n = 12) for the presence of anti-Pdx1 antibodies by Western blotting using purified full length rat Pdx1 protein. Six sera were immunoreactive with Pdx1 protein: two samples (2/25) were from patients with longstanding T1D and four samples (4/12) from individuals with a positive test for IAA. To localize the immunodominant epitopes, partially trypsin-digested Pdx1 protein was used as antigen. As shown in Figure 4A, human serum (H11) from a T1D patient recognized only full-length Pdx1 (more details below), whereas rabbit polyclonal anti-Pdx1 immune serum was immunoreactive with nearly all of the fragments. Thus the major autoepitope(s) recognized by NOD and human type 1 diabetes sera are likely to be located near the C-terminus of Pdx1 since 19 out of 29 of the trypsin-cleavage sites (arginine or lysine) are located within amino acids 160-283.
B-cell autoepitopes are located on the C-terminal portion of Pdx1
To map the B-cell autoepitopes, we constructed, expressed, and purified histidine-tagged C-terminal truncated Pdx1 proteins consisting of amino acids 1-119, 1-159, and 1-199 (Fig. 4B, upper panel). These truncated proteins were mixed with full-length rPdx1 for Western blotting using three NOD-PAA-positive mouse sera (Fig. 4C, left panel) and six human PAA-positive sera (Fig. 4C, right panel, described below). NOD mouse sera recognized primarily full length rPdx1 protein (a), with weaker binding (7R) to the truncated Pdx1 protein (b, 1-199), but not the two shorter truncated Pdx1 proteins c (1-159) and d (1-119). In contrast, the rabbit polyclonal anti-Pdx1 immune serum (rPdx1 IS) recognized all four proteins. Serum from a negative NOD mouse did not react with any of the proteins (data not shown), suggesting that the PAA in mouse sera reacted with a major epitope (I) located within the C-terminal 84 amino acid residues and a minor epitope (II) located within Pdx1 (160-199).
To exclude reactivity with the His-Tag or the possibility that amino acids 1-199 participate in forming a discontinuous epitope, we inserted a cDNA fragment encoding the C-terminal 84 amino acids (200-283) into the pGRx5.1 GST expression system. Using this protein without cleavage from GST, we performed Western blots, revealing that autoimmune NOD sera bind strongly to the GST-Pdx1/200-283 or p83 protein but not GST (Fig. 4D, upper panel), indicating that the major autoepitope indeed is located on the C-terminal portion of Pdx1 (amino acids 200-283).
Identification of epitope(s) for human PAA
To determine if PAA from human sera recognize the same epitope bound by NOD mouse PAA, a mixture of Pdx1 and its truncated forms was used for Western blotting using PAA-positive human sera of T1D patients and IAA-positive individuals. Figure 4C (top right panel) shows two patterns among the six serum samples tested. Similar to mouse autoimmune sera, the human sera in lanes 1, 2, and 3 recognized only full-length Pdx1 indicating that they bind to an epitope or epitopes within the C-terminal 84 amino acids. Interestingly human sera in lanes 4, 5, and 6 reacted equally with the top two bands, consistent with the existence of another epitope (II) located within amino acids 160-199. Figure 4C (lower panel) illustrates the two putative Pdx1 autoepitopes recognized by human sera. To confirm the locations of these epitopes, we inserted cDNA encoding Pdx1 amino acids 160-199 (as p40) into the pGRx5.1 GST expression system. Using this fusion protein, we performed Western blots, revealing that human sera (Fig. 4C, lanes 4, 5, and 6) bind strongly to the GST-p40 protein and full-length Pdx1, but not GST-p83 or GST alone, indicating that autoepitope II indeed is located within amino acids 160-199 of Pdx1 (Fig. 4D, lower panel).
Pdx1-stimulated in vitro T-cell proliferation
To determine whether Pdx1 can stimulate antigen-specific T-cell proliferation, freshly isolated splenocytes from new-onset diabetic NOD mice were stimulated with various forms of Pdx1 protein including full length Pdx1 and different truncated forms. Anti-CD3 antibodies were used as a positive control for T-cell proliferation, and as negative control we used either untreated or GST-treated (unrelated protein) T cells. Figure 5A shows that full length as well as truncated forms of Pdx1 can stimulate T-lymphocyte proliferation. However, the C-terminus of Pdx1 (200-283, or p83) had the most potent T-cell stimulatory effect (almost 7 fold increase over control GST, P<0.001 by Student’s t-test), suggesting that the major T cell epitope(s) are located in close proximity to the major B-cell autoepitope. Interestingly, a significant T-cell stimulatory effect also was observed in the wells containing p200 (4 times over control, P<0.001 by Student’s t-test), supporting the possible presence of minor autoepitopes within the region of p160-200.
Fig. 5. Antigen-specific T-cell proliferation to Pdx1 and its truncated forms.
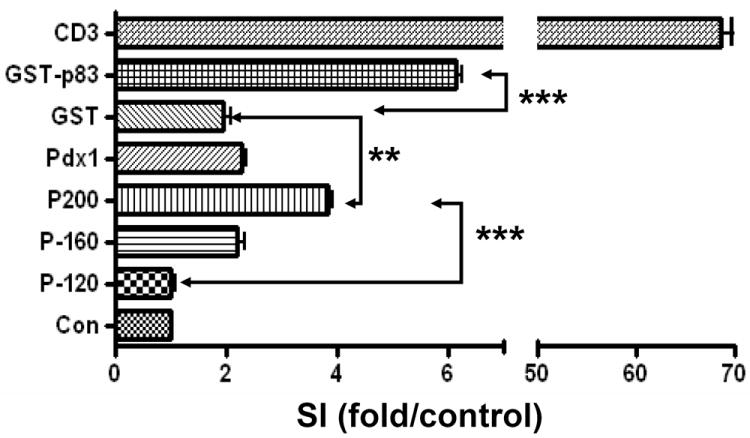
Splenocytes (106 cells/well) isolated from a NOD mouse with new onset diabetes were incubated in a 96-well plate. Pdx1 and various truncated proteins were added into the wells at a final concentration of 1 μg/ml for 48 hrs, following by adding [3H]-thymidine for an additional 24 hrs. Cells were captured on filter paper, washed 5 times, and [3H]-thymidine incorporation was determined by scintillation counting. Background count is without [3H]-thymidine. ** p <0.01, *** p < 0.001 (Student’s t-test). SI = Stimulation Index.
DISCUSSION
Autoantibodies to islet cell antigens and autoantigen-reactive T-cells are hallmarks of type 1 diabetes (1;18;19). We report here that Pdx1 is a novel pancreatic beta cell-specific autoantigen recognized by both B- and T-cells in NOD mice. Through unknown mechanisms Pdx1 protein from the pancreatic islet beta cells may stimulate the generation of the Pdx1-epitope-specific autoantibodies that can be detected by ELISA, Western blotting, and immunoprecipitation assays. Although PAA are found in both prediabetic and diabetic NOD mouse sera, the levels generally peak before the onset of diabetes. PAA were only found in NOD mice, and were not present in congenic NOD-scid mice or non-autoimmune strains such as C57BL/6 and BALB/c. The frequency of PAA in 5 to 25-week-old prediabetic mice was over 50%. Using ELISA, PAA were detectable in 5-week-old NOD mice, indicating that these antibodies are an early disease marker. Although variable, the onset of PAA production was generally before the onset of diabetes. Interestingly, autoantibody levels declined substantially or even disappeared with the onset of diabetes. The peak titers are relatively high, up to 1/20,000 or more by ELISA, suggesting that PAA may be useful for predicting the onset of diabetes in NOD mice.
Currently insulin autoantibodies (IAA) are the most specific predictor of the onset of diabetes (20-23). However, these autoantibodies generally are found at very low levels. In contrast, the titers of PAA were considerably higher than those reported previously for IAA (20), suggesting that for diabetes susceptibility screening, assays for PAA may afford an improved signal:noise ratio over assays for IAA at least in mice. Consistent with the onset of IAA (20), we detected PAA at five weeks of age. The prevalence of PAA in prediabetic NOD mice was comparable to that of IAA (23). In a collaborative international workshop study, IAA were detected by ELISA in NOD mice at frequencies of 0% at 4 weeks, 14% at 8 weeks, 19% at 12 weeks, and 42% at diabetes onset (23). Using a more sensitive radiobinding assay (RBA), IAA were detected at the onset of diabetes in 15 to 75% of NOD mice (23). In the current study, PAA were detected at disease onset in 52% of NOD mice, a figure that may improve further if larger numbers of mice are studied and a more sensitive and optimized assay is used. It will be of interest in the future to determine whether the mice exhibiting PAA and IAA are the same or overlapping sets and whether measuring both specificities enhances the predictive value of autoantibody testing in NOD mice and for T1D patients.
Analysis of the fine specificities of murine PAA revealed the presence of an immunodominant epitope or epitopes on the C-terminal 83 amino acids of the Pdx1 protein. The NOD mouse sera react strongly with GST-p83 (Pdx1 AA 200-283), indicating that sequences outside this region are not required for epitope folding. Pdx1, a highly conserved protein of 283 amino acids, contains a transactivation domain at the N-terminus (amino acids 1-79), a homeodomain in the central region (amino acids 146-206), and an evolutionarily conserved, C-terminal domain of unknown function (24). The latter region, which contains the major autoepitope(s) recognized by NOD mouse sera, notably contains 19 trypsin sensitive (arginine or lysine) sites between amino acids 160 and 283, and cleavage at these sites abolishes immunoreactivity of the C-terminal domain (Fig. 4A). Ten of these sites are located on amino acids 160-199 within the homeodomain of Pdx1 containing an antennapedia-like protein transduction domain, DNA binding domain (AA 191-196), and nuclear localization signal (AA 197-203) (16;25). However, this region is dispensable for immunogenicity, suggesting that some or all of the remaining 9 trypsin-sensitive arginine or lysine residues located on amino acids 200-280 are important in forming the immunodominant epitope.
In contrast to NOD mice, T1D patients’ sera recognize two epitopes, one of which (Epitope I) appears similar if not identical to the immunodominant epitope in NOD mice. The second autoepitope, located within the homeodomain of Pdx1 (p160-199), is recognized by a subset of human autoimmune sera (Fig. 4C) but also weakly by some murine sera (see Fig.4C, mouse #7R). This region contains 10 lysine/arginine residues, but the importance of these charged sites for antigenicity remains to be determined. Trypsin-sensitive lysine/arginine residues also are critical for the antigenicity of epitopes recognized by anti-histone antibodies (26) and basic amino acids are thought to be important for autoantibody recognition of the U1-70K component of U1 small nuclear ribonucleoproteins (27). In this regard, it is interesting to note that NOD mice also produce autoantibodies against U1 small nuclear ribonucleoproteins (28). The relationship, if any, between these autoantibodies and anti-Pdx1 autoantibodies remains to be determined. However, it has been proposed that long runs of charged amino acids may render certain self-antigens immunogenic (29). In addition, autoantibodies frequently recognize epitopes located on the N- and C- termini of proteins (30), as was the case here.
In addition to the strong humoral autoimmune response, we found that Pdx1 also is a target of cellular immunity. In T1D and other disorders, autoreactive B-cell epitopes and T-cell epitopes frequently overlap (21;31). Indeed, full-length Pdx1, its C-terminal 83 amino acids (p83), as well as homeodomain-containing truncated Pdx1 protein (p200) stimulated proliferation of splenic T cells from NOD mice (Fig. 5), suggesting that T and B cell epitopes may lie in close proximity within this region. Interestingly, the proliferative response to full-length Pdx1 was less than that to the p83 or p200 fragments (Fig. 5). This might be due to differences in the relative efficiency of antigen processing/presentation by antigen presenting cells, e.g. because of differences in protein folding and protease cleavage in endosomes. Further mapping of the locations of the T- and B- cell epitopes is in progress.
We previously showed that treatment of Stz-induced diabetic mice with full-length rPdx1 reverses diabetes by stimulating pancreatic islet β-cell regeneration and reprogramming liver cells into insulin-producing cells (11). Our recent studies indicate that daily treatment of pre-diabetic female NOD mice with rPdx1 prevents the onset of diabetes in 85% of mice at 40 weeks, whereas 95% of controls became diabetic by 25 weeks (manuscript in preparation). Interestingly, when an inactive form of Pdx1 lacking the protein translocation domain (11;16;25) was administered to NOD mice, it also protected against the development of diabetes (manuscript in preparation). Western blotting verified that the mutant Pdx1ΔPTD protein retained immunoreactivity with PAA (data not shown) and protein (p83) lacking the PTD also was capable of stimulating T cell proliferation in vitro. These findings from in vivo animal studies are consistent with the notion of Pdx1 being an autoantigen that may be related to the pathogenesis of T1D in NOD mice. Consistent with that notion, diabetes onset in NOD-scid mice was delayed following passive transfer of splenocytes from Pdx1-treated NOD mice in comparison with splenocytes from PBS-treated controls (unpublished data), suggesting that rPdx1 may exert an immunomodulatory effect by suppressing autoreactive diabetogenic T-cells, as previously shown by Ferber’s group (12). The immunologic mechanism for the phenomenon of Pdx1-treatment preventing diabetes is now under active investigation.
The presence of PAA in sera from patients with T1D suggests that our observations in the NOD mouse model have relevance to human T1D. Among the six PAA positive T1D or IAA positive patient sera identified in preliminary screening studies, we discovered two distinct patterns by Western blotting, suggesting the autoepitopes to human PAA can be located either exclusively within the C-terminus or in both the C-terminus and the homeodomain of Pdx1. It will be of interest to examine both the role of immune responses to Pdx1 in the pathogenesis of human T1D and the clinical value of testing for these autoantibodies in children at risk for developing autoimmune diabetes.
T1D is caused by autoimmune islet beta cell destruction and islet beta cell antigens are the targets of this autoimmune disorder. Self-antigens specific to islet beta cells stimulate the production of autoantibodies and the generation of antigen-specific autoreactive T-cells. These autoantigens include insulin, glutamic acid decarboxylase (GAD65), insulinoma associated-2 antigen (IA-2), Slc30A8 (32), Pdx1, and others (8) (33). Although immunotherapy can prevent T1D in the NOD mouse model, we have yet to find a safe and effective way to prevent or ameliorate T1D in humans (34;35). A recent randomized trial of GAD vaccination in new-onset of T1D patients shows very limited improvement in preserving the pancreatic beta-cell function (10) raising the possibility that it may be necessary to tolerize against multiple autoantigens in order to suppress immune attack (36) (34). Along with these previous reports regarding other beta-cell specific autoantigens, the present data suggest that combined antigen-specific immunotherapy plus beta-cell regeneration therapy may be a feasible therapeutic approach in T1D (21;37). From our current knowledge of Pdx1 and its critical roles in pancreatic development and maintenance of beta cell function (38;39), the promotion of beta-cell regeneration (11), prevention of beta-cell apoptosis (40), and reprogramming of non-pancreatic cells to become insulin-producing cells (41-43), Pdx1 might be a useful therapeutic agent for treating T1D.
Acknowledgments
This work was supported by grants from the National Institutes of Health, NIAMS AR44731 (W Reeves), and NIDDK DK071831 and DK64054 (LJ Yang).
Abbreviation
- Pdx1
Pancreatic duodenal hemeodomain protein 1
- NOD
non-obese diabetic
- NOD-scid
NOD-severe combined immunodeficient mouse
- PAA
Pdx1 autoantibodies
- SDS-PAGE
sodium dodecyl sulfate polyacrylamide gel electrophoresis
Reference List
- 1.Atkinson MA, Eisenbarth GS. Type 1 diabetes: new perspectives on disease pathogenesis and treatment. Lancet. 2001;358:221–229. doi: 10.1016/S0140-6736(01)05415-0. [DOI] [PubMed] [Google Scholar]
- 2.Wasserfall CH, Atkinson MA. Autoantibody markers for the diagnosis and prediction of type 1 diabetes. Autoimmun Rev. 2006;5:424–428. doi: 10.1016/j.autrev.2005.12.002. [DOI] [PubMed] [Google Scholar]
- 3.Miao D, Yu L, Eisenbarth GS. Role of autoantibodies in type 1 diabetes. Front Biosci. 2007;12:1889–1898. doi: 10.2741/2195. [DOI] [PubMed] [Google Scholar]
- 4.Pihoker C, Gilliam LK, Hampe CS, Lernmark A. Autoantibodies in diabetes. Diabetes. 2005;54(Suppl 2):S52–S61. doi: 10.2337/diabetes.54.suppl_2.s52. [DOI] [PubMed] [Google Scholar]
- 5.Skyler JS. Prediction and prevention of type 1 diabetes: progress, problems, and prospects. Clin Pharmacol Ther. 2007;81:768–771. doi: 10.1038/sj.clpt.6100179. [DOI] [PubMed] [Google Scholar]
- 6.Giarratana N, Penna G, Adorini L. Animal models of spontaneous autoimmune disease: type 1 diabetes in the nonobese diabetic mouse. Methods Mol Biol. 2007;380:285–311. doi: 10.1007/978-1-59745-395-0_17. [DOI] [PubMed] [Google Scholar]
- 7.Liu E, Yu L, Moriyama H, Eisenbarth GS. Animal models of insulin-dependent diabetes. Methods Mol Med. 2004;102:195–212. doi: 10.1385/1-59259-805-6:195. [DOI] [PubMed] [Google Scholar]
- 8.Aly T, Devendra D, Eisenbarth GS. Immunotherapeutic approaches to prevent, ameliorate, and cure type 1 diabetes. Am J Ther. 2005;12:481–490. doi: 10.1097/01.mjt.0000178782.97413.79. [DOI] [PubMed] [Google Scholar]
- 9.Cernea S, Pozzilli P. New potential treatments for protection of pancreatic B-cell function in Type 1 diabetes. Diabet Med. 2008;25:1259–1267. doi: 10.1111/j.1464-5491.2008.02556.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ludvigsson J, Faresjo M, Hjorth M, Axelsson S, Cheramy M, Pihl M, Vaarala O, Forsander G, Ivarsson S, Johansson C, Lindh A, Nilsson NO, Aman J, Ortqvist E, Zerhouni P, Casas R. GAD treatment and insulin secretion in recent-onset type 1 diabetes. N Engl J Med. 2008;359:1909–1920. doi: 10.1056/NEJMoa0804328. [DOI] [PubMed] [Google Scholar]
- 11.Koya V, Lu S, Sun YP, Purich DL, Atkinson MA, Li SW, Yang LJ. Reversal of streptozotocin-induced diabetes in mice by cellular transduction with recombinant pancreatic transcription factor pancreatic duodenal homeobox-1: a novel protein transduction domain-based therapy. Diabetes. 2008;57:757–769. doi: 10.2337/db07-1441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Shternhall-Ron K, Quintana FJ, Perl S, Meivar-Levy I, Barshack I, Cohen IR, Ferber S. Ectopic PDX-1 expression in liver ameliorates type 1 diabetes. J Autoimmun. 2007 doi: 10.1016/j.jaut.2007.02.010. [DOI] [PubMed] [Google Scholar]
- 13.Cao LZ, Tang DQ, Horb ME, Li SW, Yang LJ. High glucose is necessary for complete maturation of pdx-1-vp16-expressing hepatic cells into functional insulin-producing cells. Diabetes. 2004;53:3168–3178. doi: 10.2337/diabetes.53.12.3168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Satoh M, Reeves WH. Induction of lupus-associated autoantibodies in BALB/c mice by intraperitoneal injection of pristane. J Exp Med. 1994;180:2341–2346. doi: 10.1084/jem.180.6.2341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Satoh M, Reeves WH. Induction of lupus-associated autoantibodies in BALB/c mice by intraperitoneal injection of pristane. J Exp Med. 1994;180:2341–2346. doi: 10.1084/jem.180.6.2341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Noguchi H, Kaneto H, Weir GC, Bonner-Weir S. PDX-1 protein containing its own antennapedia-like protein transduction domain can transduce pancreatic duct and islet cells. Diabetes. 2003;52:1732–1737. doi: 10.2337/diabetes.52.7.1732. [DOI] [PubMed] [Google Scholar]
- 17.Martin RM, Brady JL, Lew AM. The need for IgG2c specific antiserum when isotyping antibodies from C57BL/6 and NOD mice. J Immunol Methods. 1998;212:187–192. doi: 10.1016/s0022-1759(98)00015-5. [DOI] [PubMed] [Google Scholar]
- 18.Gillespie KM. Type 1 diabetes: pathogenesis and prevention. CMAJ. 2006;175:165–170. doi: 10.1503/cmaj.060244. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jasinski JM, Eisenbarth GS. Insulin as a primary autoantigen for type 1A diabetes. Clin Dev Immunol. 2005;12:181–186. doi: 10.1080/17402520500078204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Michel C, Boitard C, Bach JF. Insulin autoantibodies in non-obese diabetic (NOD) mice. Clin Exp Immunol. 1989;75:457–460. [PMC free article] [PubMed] [Google Scholar]
- 21.Zhang L, Nakayama M, Eisenbarth GS. Insulin as an autoantigen in NOD/human diabetes. Curr Opin Immunol. 2008;20:111–118. doi: 10.1016/j.coi.2007.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Yu L, Robles DT, Abiru N, Kaur P, Rewers M, Kelemen K, Eisenbarth GS. Early expression of antiinsulin autoantibodies of humans and the NOD mouse: evidence for early determination of subsequent diabetes. Proc Natl Acad Sci U S A. 2000;97:1701–1706. doi: 10.1073/pnas.040556697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Bonifacio E, Atkinson M, Eisenbarth G, Serreze D, Kay TW, Lee-Chan E, Singh B. International Workshop on Lessons From Animal Models for Human Type 1 Diabetes: identification of insulin but not glutamic acid decarboxylase or IA-2 as specific autoantigens of humoral autoimmunity in nonobese diabetic mice. Diabetes. 2001;50:2451–2458. doi: 10.2337/diabetes.50.11.2451. [DOI] [PubMed] [Google Scholar]
- 24.Al Quobaili F, Montenarh M. Pancreatic duodenal homeobox factor-1 and diabetes mellitus type 2 (review) Int J Mol Med. 2008;21:399–404. [PubMed] [Google Scholar]
- 25.Noguchi H, Matsushita M, Matsumoto S, Lu YF, Matsui H, Bonner-Weir S. Mechanism of PDX-1 protein transduction. Biochem Biophys Res Commun. 2005;332:68–74. doi: 10.1016/j.bbrc.2005.04.092. [DOI] [PubMed] [Google Scholar]
- 26.Thomas JO, Wilson CM, Hardin JA. The major core histone antigenic determinants in systemic lupus erythematosus are in the trypsin-sensitive regions. FEBS Lett. 1984;169:90–96. doi: 10.1016/0014-5793(84)80295-1. [DOI] [PubMed] [Google Scholar]
- 27.James JA, Scofield RH, Harley JB. Basic amino acids predominate in the sequential autoantigenic determinants of the small nuclear 70K ribonucleoprotein. Scand J Immunol. 1994;39:557–566. doi: 10.1111/j.1365-3083.1994.tb03413.x. [DOI] [PubMed] [Google Scholar]
- 28.Baxter AG, Horsfall AC, Healey D, Ozegbe P, Day S, Williams DG, Cooke A. Mycobacteria precipitate an SLE-like syndrome in diabetes-prone NOD mice. Immunology. 1994;83:227–231. [PMC free article] [PubMed] [Google Scholar]
- 29.Brendel V, Dohlman J, Blaisdell BE, Karlin S. Very long charge runs in systemic lupus erythematosus-associated autoantigens. Proc Natl Acad Sci U S A. 1991;88:1536–1540. doi: 10.1073/pnas.88.4.1536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Pollard KM, Cohen MG. Predicting antigenic determinants of autoantigens. Autoimmunity. 1990;5:265–275. doi: 10.3109/08916939009014711. [DOI] [PubMed] [Google Scholar]
- 31.Di Lorenzo TP, Peakman M, Roep BO. Translational mini-review series on type 1 diabetes: Systematic analysis of T cell epitopes in autoimmune diabetes. Clin Exp Immunol. 2007;148:1–16. doi: 10.1111/j.1365-2249.2006.03244.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wenzlau JM, Moua O, Sarkar SA, Yu L, Rewers M, Eisenbarth GS, Davidson HW, Hutton JC. SlC30A8 is a major target of humoral autoimmunity in type 1 diabetes and a predictive marker in prediabetes. Ann N Y Acad Sci. 2008;1150:256–259. doi: 10.1196/annals.1447.029. [DOI] [PubMed] [Google Scholar]
- 33.Devendra D, Yu L, Eisenbarth GS. Endocrine autoantibodies. Clin Lab Med. 2004;24:275–303. doi: 10.1016/j.cll.2004.01.012. [DOI] [PubMed] [Google Scholar]
- 34.Cernea S, Herold KC. Drug insight: New immunomodulatory therapies in type 1 diabetes. Nat Clin Pract Endocrinol Metab. 2006;2:89–98. doi: 10.1038/ncpendmet0082. [DOI] [PubMed] [Google Scholar]
- 35.Harrison LC. The prospect of vaccination to prevent type 1 diabetes. Hum Vaccin. 2005;1:143–150. doi: 10.4161/hv.1.4.1923. [DOI] [PubMed] [Google Scholar]
- 36.Faustman DL. Immunotherapy on trial for new-onset type 1 diabetes. N Engl J Med. 2008;359:1956–1958. doi: 10.1056/NEJMe0807425. [DOI] [PubMed] [Google Scholar]
- 37.Mukherjee R, Wagar D, Stephens TA, Lee-Chan E, Singh B. Identification of CD4+ T cell-specific epitopes of islet-specific glucose-6-phosphatase catalytic subunit-related protein: a novel beta cell autoantigen in type 1 diabetes. J Immunol. 2005;174:5306–5315. doi: 10.4049/jimmunol.174.9.5306. [DOI] [PubMed] [Google Scholar]
- 38.Offield MF, Jetton TL, Labosky PA, Ray M, Stein RW, Magnuson MA, Hogan BL, Wright CV. PDX-1 is required for pancreatic outgrowth and differentiation of the rostral duodenum. Development. 1996;122:983–995. doi: 10.1242/dev.122.3.983. [DOI] [PubMed] [Google Scholar]
- 39.Kushner JA, Ye J, Schubert M, Burks DJ, Dow MA, Flint CL, Dutta S, Wright CV, Montminy MR, White MF. Pdx1 restores beta cell function in Irs2 knockout mice. J Clin Invest. 2002;109:1193–1201. doi: 10.1172/JCI14439. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Johnson JD, Ahmed NT, Luciani DS, Han Z, Tran H, Fujita J, Misler S, Edlund H, Polonsky KS. Increased islet apoptosis in Pdx1+/- mice. J Clin Invest. 2003;111:1147–1160. doi: 10.1172/JCI16537. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Ferber S, Halkin A, Cohen H, Ber I, Einav Y, Goldberg I, Barshack I, Seijffers R, Kopolovic J, Kaiser N, Karasik A. Pancreatic and duodenal homeobox gene 1 induces expression of insulin genes in liver and ameliorates streptozotocin-induced hyperglycemia. Nat Med. 2000;6:568–572. doi: 10.1038/75050. [DOI] [PubMed] [Google Scholar]
- 42.Tang DQ, Cao LZ, Chou W, Shun L, Farag C, Atkinson MA, Li SW, Chang LJ, Yang LJ. Role of Pax4 in Pdx1-VP16-mediated liver-to-endocrine pancreas transdifferentiation. Lab Invest. 2006;86:829–841. doi: 10.1038/labinvest.3700434. [DOI] [PubMed] [Google Scholar]
- 43.Kojima H, Fujimiya M, Matsumura K, Younan P, Imaeda H, Maeda M, Chan L. NeuroD-betacellulin gene therapy induces islet neogenesis in the liver and reverses diabetes in mice. Nat Med. 2003;9:596–603. doi: 10.1038/nm867. [DOI] [PubMed] [Google Scholar]