

Abstract
Background:
Prevalence of malnutrition among the children from developing countries has reached unprecedented level which can be evaluated by body mass index.
Aim:
This study was designed to determine the prevalence of malnutrition among the Mising children of Northeast India using four different sets of Body Mass Index references.
Materials and Methods:
A cross-sectional study was performed on a population representative sample of 511 Mising children. Four different sets of Body Mass Index reference were used to define thinness as well as overweight cases.
Results:
With the use of different references the prevalence of thinness varies from 17.18% to 27.73% among the boys and from 19.21% to 28.23% among the girls. On the other hand the prevalence of overweight varies from 1.95% to 7.81% among the boys and 1.96% to 9.41% among the girls. Reference based on United States (1971-74) survey detects sex difference in overweight. The calculated kappa values indicated a fair to almost perfect agreement between various references.
Conclusion:
Considerable prevalence of overweight despite a persistently high burden of thinness suggests existence of nutrition transition among the Mising population. Prevalence of malnutrition differs with the application of different references which warrants application of international references carefully for any potential misclassification of children.
Keywords: BMI, Northeast India, Nutritional status
Introduction
A trend of developmental transition with varying rates is underway in most of the developing countries including India and its Northeastern parts.[1–3] Transition can be observed in all aspects of human life including disease pattern, demographic and dietary pattern, socioeconomic and ecological conditions.[4] Some of the major consequences of this transition are described to be rapid spread of urbanization, increasing magnitude of socio-economic differences and coexistence of overweight along with thinness.[5] In spite of that research related to the prevalence of malnutrition particularly overweight cases among the children in the light of developmental transition is very meager in India and no such study has been reported from Northeast India. Therefore the present study is undertaken to detect the prevalence of the dual burden of malnutrition i.e. thinness as well as overweight (if present) among the Mising, a Tibeto-Burman tribal population from Northeast India.
Body mass index [weight (kg)/height (m)2] is used extensively to measure malnutrition among adults[6] and a growing interest has developed to use it among the children and adolescents.[7–9] Till date we have various international references available to detect the prevalence of malnutrition particularly overweight and thinness among the children. These include reference based on Childhood Obesity Working Group of the International obesity task force (IOTF),[9] reference prepared on the data from United States Survey conducted in 1971-74,[7,8] reference available from United States Centers for Disease Control and Prevention (CDC, 2000)[10] and the recently developed reference from World Health Organisation-2007[11] and IOTF-2007.[12] Though they were mainly developed to use in the developed countries from where the subjects were originally recruited but we can also find the use of these references in developing countries due to the lack of such national reference.[13,14] With these references various studies projected the dual burden of overweight and thinness in different population groups.[15,16] With this backdrop the present study aims to find out the difference in the prevalence of malnutrition applying different international references as these references are useful to compare between studies and countries.
Materials and Methods
The present study was conducted among the Mising tribal population of Assam and the feasibility as well as ethical issues related to the study was evaluated by the local Department Research Committee, Dibrugarh University. During the study informed consent was taken as per the ethical consideration of Helsinki declaration. The Mising population is a scheduled tribe population of Tibeto-Burman linguistic family which mainly concentrates in Upper Assam, India. They constitute the second largest tribal population of Assam. In the present study the age of the Mising children ranges from 6 to 10 years.
A representative sample of 511 children (256 male and 255 female) was selected using multistage cluster sampling. The study has been conducted in Upper Assam, India from December 2006 to November 2008 at various intervals. Students’ reported age and date of birth were verified against the school records as well as with the help of local event calendar. The minimum sample size needed for the study was calculated following Lwanga and Lemeshow[17] and one earlier study on Mising children.[18] Anthropometric data on height and weight were measured following Weiner and Lourie.[19] Precision of the measurements was assessed by the technical error of measurement (TEM) as suggested by Malina et al.[20] The TEM values were measured using the formula,
![]()
and was found well below the maximum accepted TEM reference values reported by Ulijaszek and Kerr.[21] Depending on the BMI values, thinness and overweight cases were detected on the basis of the following datasets.
The World Health Organization (WHO-2007) reference is based on the sample used to construct the original NCHS charts. It relied on GAMLSS with the Box-Cox power exponential developmental distribution and LMS model. It allows unrestricted calculation of BMI percentile and Z-score curves on the continuous age scale from 5 to 19 years.[11] Here a score more than 1 SD cutoff point is regarded as overweight case whereas a score less than -2 SD is regarded as thin.
The IOTF reference[9] has published a series of sex-age-specific BMI cut-off (from 6 to 18 years) and are developed from sex specific BMI-age curves that pass through a BMI of 25 for overweight and 30 for obesity at age 18 based on LMS method. For the detection of thinness IOTF constructed reference cutoffs based on the recommendation of WHO definition of thinness among adults.[12]
The Must, Dallal and Deitz 1991 reference (MUST reference) is based on the data from the US (NHANES I) surveys. It has been recommended to use BMI 85th percentile to classify child overweight.[7,8] The percentile values were evaluated by the curve representing specific percentile variation with age and were smoothed by lowess. Here the 5th and 85th percentiles have been taken as a cut off for thinness and overweight respectively.
The United States Centers for Disease Control and Prevention (CDC 2000) reference is the revised version of the NCHS 1977 growth charts.[10] Here 85th percentile is used to describe the risk of overweight following the advice of the US Expert Committee on childhood obesity. At the lower end of the distribution of BMI-for-age, an analogous chart is used to assess thinness using 5th percentile as a cutoff mark.
Statistical Analysis
Standard statistical analysis has been used in the present study. Sex differences in the prevalence of malnutrition were tested using χ2 test. Kappa coefficient has been considered to see the inter reference variation. This has been calculated by considering kappa = (P0–Pe)/(1–Pe), where Pe = expected probability of agreement by chance and P0 = observed probability of agreement. A kappa with a value of ≥ 0.4 has been taken as a data with moderate agreement, whereas the same with ≥ 0.8 is considered as a good agreement.[22]
Results
Figure 1 describes the mean BMI of the Mising children according to age and sex. The mean BMI increases with age in both sexes. Mean BMI values are found to be higher in boys compared to girls in all age groups however no significant difference has been found in this respect. The age sex standardized prevalence of thinness as well as overweight cases according to various references has been presented in Table 1. The percentage frequency distribution of thin, normal as well as overweight cases with respect to different references has been provided in Figure 2. Table 1 suggests a considerable prevalence of overweight cases along with the persistent occurrence of high thinness among the Mising children. The table suggests that in terms of thinness all the four references show consistently high thinness in all the age groups. In both the sexes CDC reference shows a considerable higher prevalence of thinness (27.73% for boys and 28.23% for the girls) than the other references. With this reference the prevalence of thinness increases with age in both sexes. The new references of WHO and IOTF detect somewhat low prevalence of thinness in comparison to the MUST and the CDC data sets.
Figure 1.

Mean BMI (± S.E.) across ages among the Mising children
Table 1.
Prevalence of thinness and overweight (%) among the mising children

Figure 2.
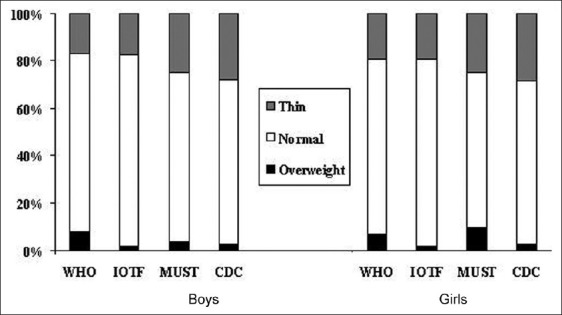
Frequencies of thin, normal and overweight children assessed on the basis of four different sets of criteria
On the other hand the overall prevalence of overweight follows a similar trend in both the sexes. WHO, IOTF and CDC detects 7.81%, 1.95%, 2.73% of the boys and 6.66%, 1.96%, 2.74% of the girls to be overweight. Only MUST reference detects a significantly higher frequency of overweight among the boys (9.41%) than in the girls (3.51%). This is only because MUST reference detects a very high frequency of overweight case among the 6 years age girls (30.1%). Among all the references IOTF reference predicts comparatively low prevalence of overweight case.
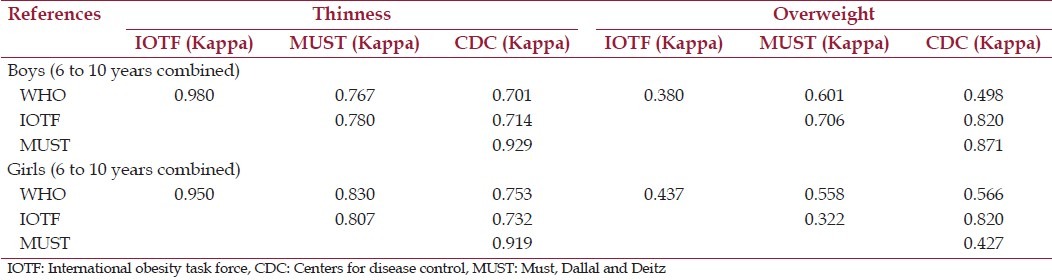
The calculated kappa coefficients with regard to the comparative analysis of malnutrition between different references have been presented in Table 2. With regard to the detection of thinness the Kappa coefficient values (boys = 0.98 and girls = 0.95) suggest an excellent agreement between WHO and IOTF references in both sexes. Whereas in terms of overweight cases IOTF reference shows an excellent agreement with CDC reference in both the sexes (kappa = 0.82 in boys and kappa = 0.82 in girls). The Kappa values also show very low agreement between WHO and IOTF among the boys (0.380) and between IOTF and MUST among girls (0.322).
Table 2.
Kappa values: Agreement of different references for thinness and overwe
Discussion
Extensive data are available on the frequencies of child undernutrition particularly thinness but very few publications report the frequencies of overweight among the tribal children of developing countries like India particularly from Northeast India. Perhaps, the prevalence of overweight in our study can be explained by the recent trend of socio-economic transition coupled with nutrition transition in Northeast India.[2] The existence of this double burden of malnutrition poses a challenge for public health intervention at population level as the overweight children are at the higher risk of non-communicable and degenerative diseases at adulthood.[23] Various socio-economic factors play a role in the phenomena of such nutrition transition. It is not only availability and household level access to food that determines nutritional status of children. Factors like education, sanitation, access to water, accessibility and quality of health services, cultural attitudes and beliefs are also equally important in this aspect.
Except MUST criteria all the references detect higher prevalence of overweight among the boys than the girls. Higher prevalence of overweight among boys has also been observed in other studies.[24]
In terms of the estimate rate of overweight, IOTF reference predicts the lowest prevalence of overweight in both the sexes. Other studies also suggest lower estimate of overweight with the use of IOTF reference.[25] It gives us an idea that age specific cut-off values like IOTF are more rigid to detect the overweight cases than the BMI centile based standards like WHO, MUST and CDC. However there are studies where IOTF standard produces higher estimates of overweight and obesity than the BMI centile based MUST reference.[26]
The prevalence of thinness is found to be higher among the girls than in the boys. It is somewhat inconsistent to the general trend found in most of the studies from other countries. It has already been reported that vulnerability to poor environmental conditions like infections and nutritional deprivation towards thinness is greater in boys than in girls.[27] Our study shows the trend of higher thinness among girls in the early childhood period and here age sex grouping may be an important factor for such outcome. Similar findings of higher thinness among girls than boys are available in some other studies.[28,29] CDC reference estimates higher prevalence of thinness than any other references. The WHO and IOTF references detect almost similar prevalence of thinness in both sexes which is consistent with a recent finding.[14]
The differences in the estimated prevalence of thinness and overweight with the application of different references can be explained by the difference of cut-offs that can be explained by the factors like period and country of source for the reference, the design of the study and the smoothing procedure applied to construct the references. Where, MUST reference applied a locally weighted regression scatter-plot smoothing procedure, WHO, IOTF and CDC reference used the LMS method for smoothing their data. Therefore it will be prudent to understand the nature of any international reference before applying it to any population based study.
Conclusion
Considerable prevalence of overweight despite a persistently high burden of thinness among Mising children may suggest existence of nutrition transition in Northeast India and calls for detection of overweight cases in other nearby population groups. Searching for the determinants of overweight in these population groups will be a promising field for future study. Prevalence of malnutrition differs with the application of different references which warrants application of international references carefully for any potential misclassification of children. The differences obtained by applying different cutoff points at individual as well as population level are important for further studies that seek to answer certain questions that whether certain cutoff points are linked with morbidity or mortality endpoints or not. There is no local standard or reference available to define overweight and thinness among the children from Northeast Indian region. It may be possible that the population groups from Northeast Indian region have different growth characteristics from the populations that were selected to develop the international references. Thus a local age-specific BMI references and cut-offs for children and adolescents are of an urgent need which may accurately provide predictive risks of significant metabolic morbidity and disease burden throughout the lifecycle. In this respect consideration of the molecular mechanism related to the different form of malnutrition will be an additional input to come to a final conclusion.
Acknowledgments
This research was supported by doctoral fellowship grants from Indian Council of Social Science Research, New Delhi (F.No.9-5/NE/09-09/F). All the subjects who participated in the study are gratefully acknowledged.
Footnotes
Source of Support: Doctoral fellowship grants from Indian Council of Social Science Research, New Delhi (F.No.9-5/NE/09-09/F).
Conflict of Interest: None declared.
References
- 1.Amuna P, Zotor FB. Epidemiological and nutrition transition in developing countries: Impact on human health and development. Proc Nutr Soc. 2008;67:82–90. doi: 10.1017/S0029665108006058. [DOI] [PubMed] [Google Scholar]
- 2.Sikdar M. Influence of socioeconomic transition on genetic structure: A case study in Upper Assam, India. Ann Hum Biol. 2008;35:112–20. doi: 10.1080/03014460701822011. [DOI] [PubMed] [Google Scholar]
- 3.Sikdar M. Socioeconomic covariates and their impact on the opportunity for natural selection in a riparian tribe of Northeast India. Anthropol Anz. 2012;69:273–87. doi: 10.1127/0003-5548/2012/0195. [DOI] [PubMed] [Google Scholar]
- 4.Dasgupta P, Saha R, Nube M. Changes in body size, shape and nutritional status of middle-class Bengali boys of Kolkata, India, 1982-2002. Econ Hum Biol. 2008;6:75–94. doi: 10.1016/j.ehb.2007.05.001. [DOI] [PubMed] [Google Scholar]
- 5.Gillespie S, Haddad LJ. Causes, Consequences and Solutions. New Delhi: Sage Publications; 2003. The double burden of Malnutrition in Asia. [Google Scholar]
- 6.WHO. Physical status: The use and interpretation of anthropometry. World Health Organ Tech Rep Ser. 1995;854:161–262. [PubMed] [Google Scholar]
- 7.Must A, Dallal GE, Dietz WH. Reference data for obesity: 85th and 95th percentiles of body mass index (wt/ht2)- a correction. Am J Clin Nutr. 1991a:839–46. doi: 10.1093/ajcn/53.4.839. [DOI] [PubMed] [Google Scholar]
- 8.Must A, Dallal GE, Dietz WH. Reference data for obesity: 85th and 95th percentiles of body mass index (wt/ht2) - a correction. Am J Clin Nutr. 1991;; 54:773. doi: 10.1093/ajcn/53.4.839. [DOI] [PubMed] [Google Scholar]
- 9.Cole TJ, Bellizzi MC, Flegal KM. Establishing standard definition for child overweight and obesity worldwide: International survey. BMJ. 2000;320:1240–3. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Kuczmarski RJ, Ogden CL, Grummer-Strawn LM, Flegal KM, Guo SS, Wei R, et al. CDC growth charts: United States. Adv Data. 2000;8:1–27. [PubMed] [Google Scholar]
- 11.De Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85:660–7. doi: 10.2471/BLT.07.043497. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Cole TJ, Flegal KM, Nicholls D, Jacjson AA. Body mass index cutoffs to define thinness in children and adolescents: International survey. BMJ. 2007;335:194–7. doi: 10.1136/bmj.39238.399444.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Maiti S, Ghosh D, Paul S. Prevalence of thinness among early adolescent in rural school girls of Paschim Medinipur, West Bengal, India. J Trop Pediatr. 2011;57:496–7. doi: 10.1093/tropej/fmr005. [DOI] [PubMed] [Google Scholar]
- 14.Bovet P, Kizirian N, Madeleine G, Blossner M, Chiolero A. Prevalence of thinness in children and adolescents in the Seychelles: Comparison of two international growth references. Nutr J. 2011;10:65. doi: 10.1186/1475-2891-10-65. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Oulamara H, Agli AN, Frelut ML. Changes in the prevalence of overweight, obesity and thinness in Algerian children between 2001 and 2006. Int J Pediatr Obes. 2009;4:411–3. doi: 10.3109/17477160802596163. [DOI] [PubMed] [Google Scholar]
- 16.Jafar TH, Qadri Z, Islam M, Hatcher J, Bhutta ZA, Chaturvedi N. Rise in childhood obesity with persistently high rates of undernutrition among urban school-aged Indo-Asian children. Arch Dis child. 2008;93:373–8. doi: 10.1136/adc.2007.125641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Boruah A. Department of Anthropology, Dibrugarh University; 2008. Growth and nutritional surveillance among the Misings and Kaibarta children of Dhakuakhana subdivision, Lakhimpur District, Assam. Unpublished M.Sc dissertation. [Google Scholar]
- 18.Lwanga SK, Lemeshow S. Geneva: WHO publication; 1991. Sample size determination in health studies: A practical manual. [Google Scholar]
- 19.Weiner JS, Lourie JA. London: Academic Press; 1981. Practical human biology. [Google Scholar]
- 20.Malina RM, Hamill PV, Lemeshow S. Selected measurements of children 6-11 years.United States. Vital Stat. 1973;11:123. [Google Scholar]
- 21.Ulijaszek SJ, Kerr DA. Anthropometric measurements error and the assessment of nutritional status. Br J Nutr. 1999;82:165–77. doi: 10.1017/s0007114599001348. [DOI] [PubMed] [Google Scholar]
- 22.Landis JR, Koch GC. The measurement of observer agreement for categorical data. Biometrics. 1977;33:159–74. [PubMed] [Google Scholar]
- 23.Reilly J, Kelly J. Long term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. Int J Obes. 2011;35:891–8. doi: 10.1038/ijo.2010.222. [DOI] [PubMed] [Google Scholar]
- 24.Kaur N, Sidhu SK, Sidhu S. Prevalence of overweight and obesity in preschool children of Amritsar, Punjab. Anthropologist. 2010;12:221–4. [Google Scholar]
- 25.Jinabhai CC, Taylor M, Sullivan KR. Implications of the prevalence of stunting, overweight and obesity amongst South African primary school children: A possible nutritional transition? Eur J Clin Nutr. 2003;57:358–65. doi: 10.1038/sj.ejcn.1601534. [DOI] [PubMed] [Google Scholar]
- 26.Flegal KM, Ogden CL, Wei R, Kuczmarski RL, Johnson CL. Prevalence of overweight in US children: Comparison of US growth charts from the Centers for Disease Control and Prevention with other reference values for body mass index. Am J Clin Nutr. 2001;73:1086–93. doi: 10.1093/ajcn/73.6.1086. [DOI] [PubMed] [Google Scholar]
- 27.Khongsdier R, Varte T, Mukherjee N. Excess male chronic energy deficiency among adolescents: A cross-sectional study in the context of patrilineal and matrilineal societies in Northeast India. Eur J Clin Nutr. 2005;59:1007–14. doi: 10.1038/sj.ejcn.1602205. [DOI] [PubMed] [Google Scholar]
- 28.Deshmukh PR, Gupta SS, Bharambe MS, Dongre AR, Maliye C, Kaur S, et al. Nutritional status of Adolescents in Rural Wardha. Indian J Pediatr. 2006;73:139–41. doi: 10.1007/BF02820204. [DOI] [PubMed] [Google Scholar]
- 29.Bose K, Das S. Thinness among the Hill Kharia children and adolescents of Purulia using Body Mass Index cut-off points. Res Rev. 2011:2–3. [Google Scholar]