

Abstract
Background
Acquired thrombotic thrombocytopenic purpura is still associated with a 10–20% death rate. It has still not been possible to clearly identify early prognostic factors of death. This study involved thrombotic thrombocytopenic purpura patients with acquired severe (<10% of normal activity) ADAMTS13 deficiency and aimed to identify prognostic factors associated with 30-day death.
Design and Methods
The study involved a prospective cohort of patients and was carried out between October 2000 and August 2010. A validation cohort of patients was set up from September 2010 to August 2011. Altogether, 281 (analysis cohort) and 66 (validation cohort) consecutive adult thrombotic thrombocytopenic purpura patients with acquired severe ADAMTS13 deficiency were enrolled. The study evaluated 30-day mortality after treatment initiation according to characteristics at inclusion.
Results
Non-survivors (11%) were older (P=10−6) and more frequently presented arterial hypertension (P=5.10−4) and ischemic heart disease (P=0.013). Prognosis was increasingly poor with age (P=0.004). On presentation, cerebral manifestations were more frequent in non-survivors (P=0.018) and serum creatinine level was higher (P=0.008). The most significant independent variables determining death were age, severe cerebral involvement and LDH level 10 N or over. A 3-level risk score for early death was defined and confirmed in the validation cohort using these variables, with higher values corresponding to increased risk of early death.
Conclusions
A risk score for early death was defined in patients with thrombotic thrombocytopenic purpura and validated on an independent cohort. This score should help to stratify early treatment and identify patients with a worse prognosis.
Keywords: thrombotic thrombocytopenic purpura, ADAMTS13, prognostic factor, plasma exchange, rituximab
Introduction
Thrombotic thrombocytopenic purpura (TTP) is a severe form of thrombotic microangiopathy (TMA) characterized by profound thrombocytopenia, erythrocyte fragmentation and organ failure of variable severity. This rare disease results from an excessive systemic platelet aggregation caused by the accumulation of unfolded high molecular weight von Willebrand factor (VWF) multimers in plasma. This failure to degrade the endothelium-derived hyper-reactive VWF multimers into less adhesive forms is related to a severe deficiency in ADAMTS13 (A Disintegrin And Metalloproteinase with Thrombo -Spondin-1 like motifs), a protease specifically involved in this process.1 Severe ADAMTS13 deficiency results from biallelic mutations of the encoding gene in hereditary forms, or from polyclonal autoantibodies in acquired forms.2 These pathophysiological findings account for the efficiency of plasma-based treatment in TTP, which results in supplying ADAMTS13 deficiency. Immunomodulatory drugs aimed at depleting anti-ADAMTS13 antibody-producing B-lymphocytes are associated to standard treatment in an increasing number of cases.3,4 Such therapeutical strategies greatly improved TTP prognosis, with overall survival rates reaching 80–85%.5 Despite this significant progress, death still occurs in up to 20% of patients according to most large multicenter reports, usually within the first days of management. Interestingly, according to some authors, this incidence has apparently not improved for more than 20 years.6 Therefore, it is becoming essential to understand the factors associated with a fatal outcome at the acute phase of the disease from large series of patients in order to better tailor initial treatment and further improve these results. So far, however, the risk factors associated with death have remained unclear. Severe clinical presentation on diagnosis, including cerebral involvement, renal failure,7 very low platelet count and profound anemia, was variably associated with a higher mortality rate by some authors8,9 but were not confirmed by others.7,10–13 Patients at relapse were also reported as having a better disease prognosis.14 Studies assessed the prognostic value of anti-ADAMTS13 antibodies, and inhibitory anti-ADAMTS13 antibodies were associated with a more severe thrombocytopenia,15 a delayed response to standard treatment16,17 or an increased mortality rate.5,6,18
So far, identification of accurate prognostic factors in TTP has been hampered by the limited series of homogeneous patients. However, the increasing number of patients included prospectively in national registries should now help address this question. We, therefore, conducted a study from a large, homogeneous group of patients included in our registry. We report original independent risk factors associated with 30-day death, and provide a prognostic score aimed at identifying at diagnosis patients at risk of fatal outcome who could possibly benefit from more intensive first-line therapies.
Design and Methods
Study design
To assess prognostic factors associated with early death at the acute phase of TTP, we studied the characteristics of adult (≥ 18 year-old) patients who died during the 30-day period starting from treatment initiation (non-survivors group). These features were compared to those of patients who survived this phase (survivors group). Patients of both groups were included during the same period of time from October 2000 (date at which our registry was set up)19 to the date of the study design (August 2010). All patients were studied until death or durable remission. From this study group (learning group), we established a prognostic score to identify patients at risk of death during the episode of TTP using information at diagnosis. To validate our results on a prospective series of patients, a second group of patients (validation group) managed with the same conditions was set up from the same centers during the analysis period of the study group, i.e. from September 2010 to August 2011. All patients of the whole study were included non-selectively from intensive care units and departments of internal medicine, hematology and nephrology in 39 French centers. The study protocol was reviewed and approved by the institutional review board and ethical committee. Informed consent was obtained from all patients.
Patients and treatment
All adult patients with a first episode of TTP associated with a severe acquired ADAMTS13 deficiency (< 10% of normal activity) were enrolled in the study6,19 Details of inclusion criteria and treatment are available in the Online Supplementary Appendix. To avoid the influence of inadequate plasma volumes in survival and to focus on the prognostic value of patients’ characteristics on diagnosis, we excluded patients who were not managed according to standard recommendations.4,6
Data analysis
Data were collected from diagnosis and before treatment,19 with particular attention to any past history of cardiovascular risk factors (including arterial hypertension and diabetes) and a pre-existing history of ischemic heart disease and ischemic stroke. Cerebral involvement assessment on diagnosis included headache, stupor, seizure and/or focal deficiency. Renal involvement was assessed by serum creatinine level and the estimated glomerular filtration rate (eGFR) by the Modification of the Diet in Renal Disease (MDRD) method. Measurement of ADAMTS13 activity, ADAMTS13 plasma inhibitor and anti-ADAMTS13 antibodies were performed as previously described (Online Supplementary Appendix).20
Statistical analysis
Quantitative variables were summarized by mean (standard deviation) and compared by the Wilcoxon’s rank-sum test; categorical data were summarized as count (%) and compared by the χ2 or Fisher’s exact test. Risk factors of early mortality were investigated by logistical regression. First, a univariable analysis was carried out and variables associated with mortality at P<0.20 were included in a backward multivariable analysis. Only variables at P=0.05 were kept in the final model. Multiple imputation was used for missing values. Using rounded coefficients from the linear predictor of the multivariable analysis, we designed a score for early death taking discrete values from 0 to 4. The score was validated by testing association of score with early death by TTP in a logistical regression. A cut-off value was obtained by maximizing the Youden score (sensitivity + specificity − 1), and the sensitivity, specificity, positive and negative predictive values and their respective 95% confidence intervals (95% CI) were determined. The area under the ROC (Receiver Operating Characteristic) curve was used to evaluate the discriminating power of our score. The difference in discriminating power between tests was evaluated using deLong procedure.21 Data were analyzed using the R software version 2.9.
Results
Study group
From October 2000 to August 2010, the registry included 944 adult patients with a diagnosis of TMA and available data. Among them, 281 were considered as having TTP with an acquired severe ADAMTS13 deficiency fulfilling all study inclusion criteria (Online Supplementary Figure S1). All were followed for at least 30 days after treatment initiation. Thirty-three patients died during the 30-day period of observation, corresponding to a 12% (95% CI: 8–15%) death rate. The other patients were discharged.
Univariable analysis for prognostic factors
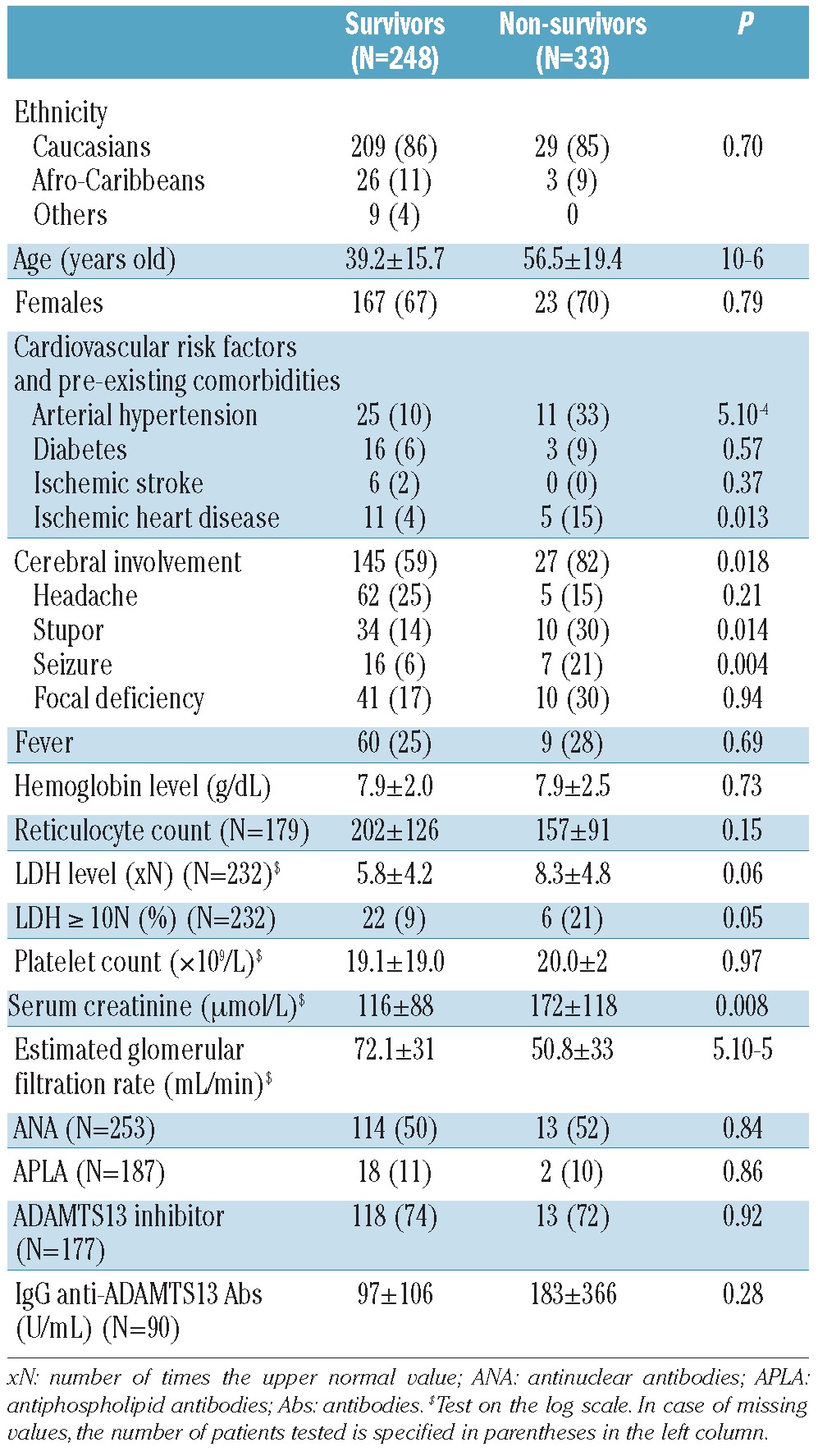
Table 1 shows the clinical features of patients of the learning cohort on diagnosis according to outcome. Non-survivors were older (P=10−6) and more frequently presented arterial hypertension (P=5.10−4) and ischemic heart disease (P=0.013). On presentation, cerebral involvement, including stupor and seizure, were more frequently observed in non-survivors (P=0.018, P=0.014 and P=0.004, respectively). Serum creatinine level was higher (P=0.008) and eGFR was lower (P=5.10−5) in non-survivors. The incidence of inhibitory anti-ADAMTS13 antibodies and the titers for IgG anti-ADAMTS13 antibodies were comparable between survivors and non-survivors.
Table 1.
Clinical characteristics of patients on diagnosis according to outcome.
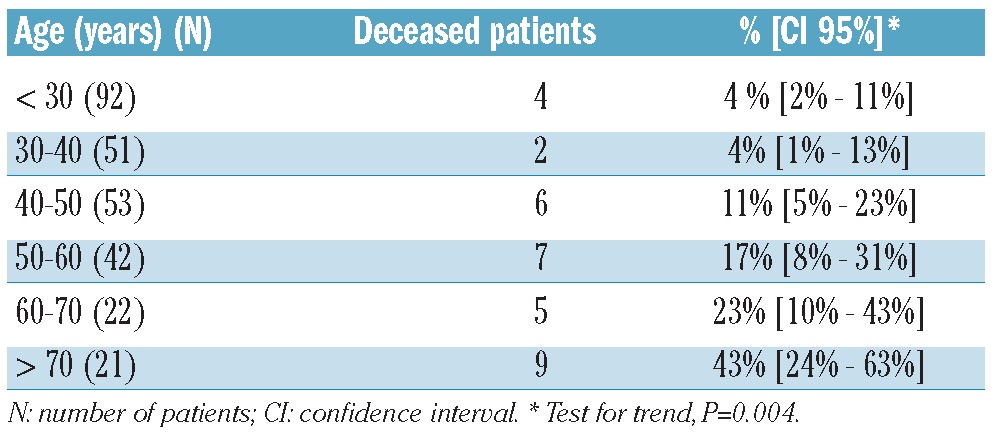
Age clearly showed the greatest impact on survival in our series. To further investigate this, we analyzed the number of non-survivors according to age group (Table 2). We found that the older the patients were, the poorer the prognosis, with a particularly poor prognosis for patients over 60 years of age (test for trend P=0.004). By comparing patients over 60 years of age with younger patients we confirmed that older patients had distinct characteristics at presentation with more frequent cardiovascular risk factors and pre-existing comorbidities; organ injury was predominant (i.e. cerebral manifestations were more frequent and renal involvement was more severe), whereas anemia was less profound (Online Supplementary Table S1).
Table 2.
Mortality rate in patients according to age class.
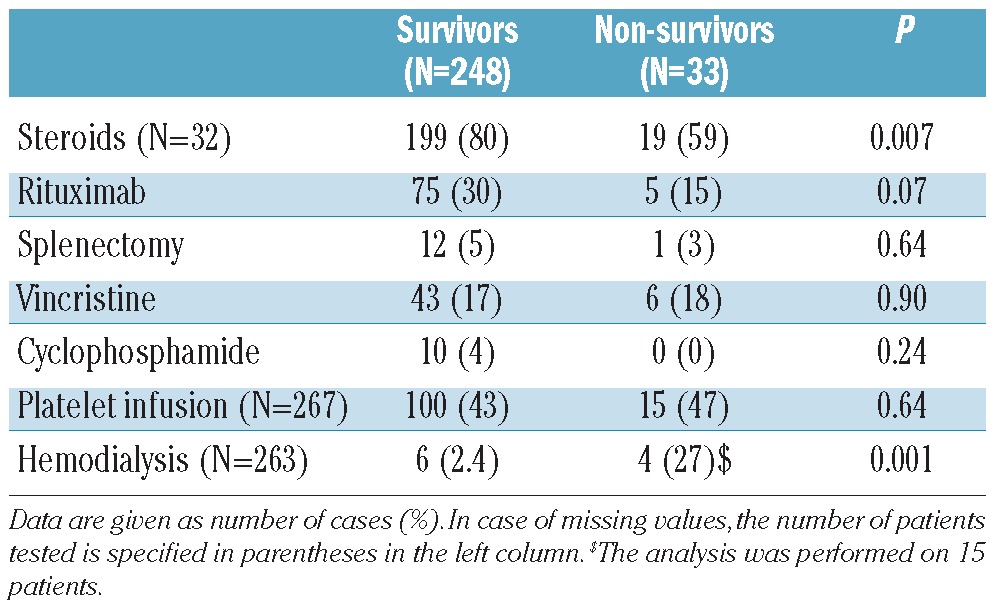
Most deaths (77%) occurred in the first two weeks after diagnosis (mean time from admission to death 9.1±8.1 days). Patients who died had received a plasma volume of 346±303 mL/kg. Death occurred in a context of one or multiple organ failure in relation with uncontrolled TTP. There was no significant increase in platelet count between diagnosis and death (20±24×109/L vs. 25±40×109/L, respectively, P=0.97). Non-survivors received steroids less frequently than survivors (P=0.007). There was no difference in the use of salvage therapies (i.e. rituximab, vincristine, cyclophosphamide and splenectomy) between survivors and non-survivors (P=NS for all). To assess whether rituximab could have influenced TTP prognosis in more recent years, we compared the number of deceased patients before and after the rituximab era. We found that between those two periods (from 2001 to 2004 and from 2005 to 2010, respectively), the number of deceased patients was comparable: 15 of 112 (13.4%) and 18 of 169 (10.7%) patients, respectively (P=0.57), which apparently does not support a major role for rituximab in the improvement of TTP survival. Survivors achieved a durable complete remission within 23.7±23 days, and required a plasma volume of 787±670 mL/kg. Platelets were infused in patients of both groups mainly for severe thrombocytopenia soon after plasma therapy had been started, without any apparent worsening of their clinical condition. Dialysis was more frequently performed in non-survivors than in survivors (P=0.001) (Table 3).
Table 3.
Patient management according to outcome.
Multivariable analysis
Variables tested for inclusion in the model were age, arterial hypertension, cerebral involvement, LDH, serum creatinine and eGFR. Arterial hypertension was not retained in the model as it was strongly correlated with increasing age. Finally, increasing age, cerebral involvement and LDH level of 10 N or over were retained as risk factors in the multivariable model (Online Supplementary Table S2 and Table 4). On the basis of the coefficients of the multivariable regression, the following score was developed: cerebral involvement or LDH level 10 N or over scored 1 point, age between 41–60 years scored 1 point and age over 60 years scored 2 points (Table 4). Table 5 reports mortality for patients according to increasing score groups. The cut off maximizing the Youden score was 3. Using this threshold, the sensitivity (% score ≥ 3 among non-survivors) was 52% (95% CI: 35%, 67%) and specificity (score < 3 among survivors) 90% (95% CI: 86%, 93%). The positive predictive value (mortality among those with a score ≥ 3) was 41% (95% CI: 28%, 57%) and negative predictive value (survival among patients with a score < 3) was 93% (95% CI: 89%, 96%). The AUC was 0.77, showing that the score had discriminating ability (P<0.0001) (Figure 1).
Table 4.
Association between patients’ characteristics and outcome by multivariable analysis.
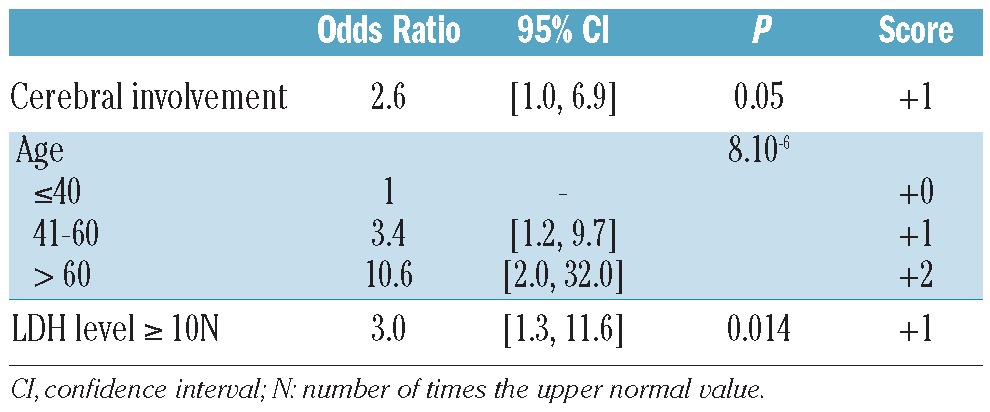
Table 5.
Prognostic score of thrombotic thrombocytopenic purpura mortality in the learning cohort and in the validation cohort according to increasing score groups.
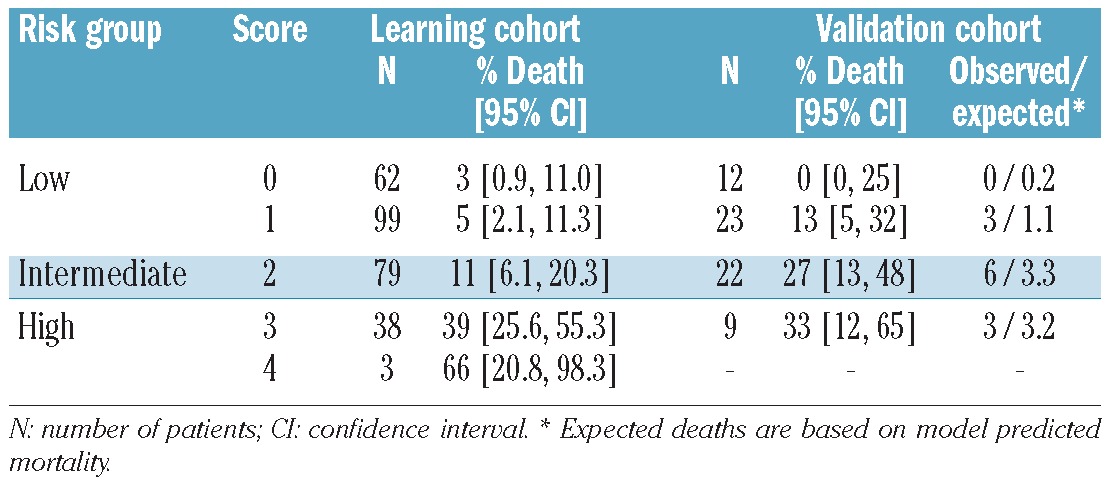
Figure 1.
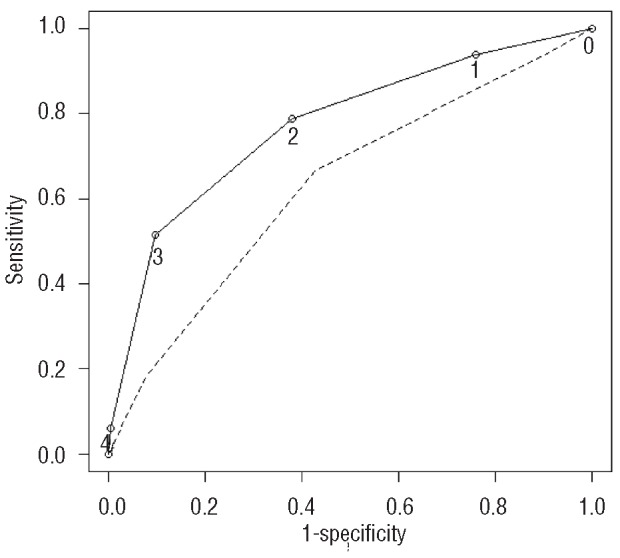
ROC (Receiver Operating Characteristic) curve. The AUC (area under the curve) was 0.77, showing that the score had discriminating ability (P<0.0001). The present score (full line) had better discriminating ability than the Wyllie score (broken line) (deLong test, P<0.0035).
Accuracy and validation of the prognostic score
Of the 66 patients included for validation (clinical features at diagnosis are shown in Online Supplementary Table S3), 12 died in the 30 days after initial diagnosis. The scores calculated for this sample ranged from 0 to 3. There was increasing mortality with increasing score in the validation cohort (P<0.025). The calibration of the model was also reasonable, as the observed number of deaths in each risk group was comparable with the expected number of deaths calculated using the predicted mortality from the model (Table 5). Mortality in the 9 patients with a score of 3 or over in the validation sample was 33%, no different from the PPV calculated above (P=0.36). Survival in the validation sample patients with score below 3 was 84%, a little smaller than the 93% expected according to PNV (P=0.01).
Discussion
We report a simple and reliable prognostic score for TTP based on critical factors related to clinical presentation in a large group of homogeneous patients on diagnosis. Our findings emphasized that categorizing according to age is important in order to evaluate survival. Indeed, this study provides strong evidence that TTP in older patients has a more aggressive presentation, with a more severe organ dysfunction (as illustrated here by a higher incidence of cerebral involvement and a more severe renal involvement, with more stupor and seizure and a higher serum creatinine level, respectively) and, consequently, a higher death rate. Previous retrospective studies with a more limited number of patients also emphasized that non-survivors were older than survivors.13,22–24 A more severe neurological and/or renal involvement was also reported in non-survivors, in agreement with our findings.7,8,13,22,24,25 By contrast, we were unable to correlate the severity of cytopenias and the presence of fever with prognosis.13,25 Despite those inconsistencies, which may be due to differences in inclusion criteria and in the size of the cohorts, our results add to those of an increasing number of studies in providing clear evidence that age has a strong impact on TTP prognosis.
The more severe prognosis of TTP in older patients can be explained in different ways. First, most patients in our study had a history of arterial hypertension which results in chronic endothelial and vascular dysfunction that worsens with ageing.26 In line with this, patients in the non-survivors group, which included a large number of older patients, more frequently had a history of ischemic heart disease. Second, ageing is physiologically associated with vascular senescence and loss of vascular compliance27 that may result in a higher shear stress and to more severe vascular wall constraints and organ injury during TTP. Furthermore, the very high LDH level we identified as a factor of worse prognosis reflects a severe multiple organ involvement28 which may include not only brain and kidney, but also heart, digestive tract, adrenal glands, pancreas and liver.29 In particular, cardiac involvement was associated with a high incidence of morbidity and mortality,30–32 and it is likely that the evaluation of this latter should improve the accuracy of our prognostic score.
Despite standard treatment, the mortality of TTP in high-risk categories may range from 30% to 60%. Therefore, our score should help in the early management of these patients to decide whether or not additional therapies should be added to standard treatment soon after diagnosis. Among these, rituximab could be a promising strategic therapy in this context, though its efficiency is not immediate.4 Some reports have suggested that the administration of very high volumes of plasma could improve the prognosis of the more severe cases.33 Older patients with a diagnosis of TTP should have the benefit of greater supportive intensive care and should receive careful monitoring, with more careful attention to cardiac and renal function, in intensive care units. Also, forthcoming studies should evaluate the role of promising adjunctive therapies in these patients,34 and our score should help to identify accurately the patients most suitable for such studies.
One limitation of our study is some variation in the treatment of patients during the inclusion period. In particular, in more recent years, there have been an increasing number of patients with a suboptimal response to standard treatment with rituximab and this may have influenced TTP prognosis. However, the number of patients who died was comparable throughout the inclusion period, and particularly before and after the rituximab era. Similarly, steroids were administered more frequently in survivors, though this difference was not significant by multivariable analysis. Therefore, we cannot determine whether in our study steroids had an impact on prognosis. It is also likely that steroids were less frequently administrated in non-survivors because this group included a large number of older patients for whom prescription of steroids is not considered optimal.
In conclusion, we provide a reliable score predictive of death in TTP with acquired severe ADAMTS13 deficiency that should help to tailor treatment on admission. We provide strong evidence that age is an important prognostic factor. In patients with a higher score, more intensive therapies should be considered and these should be evaluated in prospective trials.
Acknowledgments
Patients were recruited with the help of the members of the Reference Center for Thrombotic Microangiopathies (CNR-MAT) (listed in the appendix). We thank S. Thouzeau, S. Savigny (Laboratoire d’Hématologie, Hôpital Antoine Béclère, AP-HP, Clamart), A. de Labarthe (Laboratoire d’Hématologie, Hôpital Saint-Louis, AP-HP, Paris), I. Hauchard (Service de Réanimation, Hôpital de Rouen), M. Baragay (Laboratoire d’Immunologie, Hôpital Saint-Louis, AP-HP, Paris) for technical assistance. This work was funded by grants from the Etablissement Français du Sang (CS/2002/009) and the GIS-Institut des Maladies Rares (GIS MR0428).
Footnotes
The online version of this article has a Supplementary Appendix.
Authorship and Disclosures
The information provided by the authors about contributions from persons listed as authors and in acknowledgments is available with the full text of this paper at www.haematologica.org.
Financial and other disclosures provided by the authors using the ICMJE (www.icmje.org) Uniform Format for Disclosure of Competing Interests are also available at www.haematologica.org.
References
- 1.Sadler JE. Von Willebrand factor, ADAMTS13, and thrombotic thrombocytopenic purpura. Blood. 2008;112(1):11–8. doi: 10.1182/blood-2008-02-078170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Klaus C, Plaimauer B, Studt JD, Dorner F, Lammle B, Mannucci PM, et al. Epitope mapping of ADAMTS13 autoantibodies in acquired thrombotic thrombocytopenic purpura. Blood. 2004;103(12):4514–9. doi: 10.1182/blood-2003-12-4165. [DOI] [PubMed] [Google Scholar]
- 3.Scully M, McDonald V, Cavenagh J, Hunt BJ, Longair I, Cohen H, et al. A phase II study of the safety and efficacy of rituximab with plasma exchange in acute acquired thrombotic thrombocytopenic purpura. Blood. 2011;118(7):1746–53. doi: 10.1182/blood-2011-03-341131. [DOI] [PubMed] [Google Scholar]
- 4.Froissart A, Buffet M, Veyradier A, Poullin P, Provot F, Malot S, et al. Efficacy and safety of first-line rituximab in severe, acquired thrombotic thrombocytopenic purpura with a suboptimal response to plasma exchange. Experience of the French Thrombotic Microangiopathies Reference Center. Crit Care Med. 2012;40(1):104–11. doi: 10.1097/CCM.0b013e31822e9d66. [DOI] [PubMed] [Google Scholar]
- 5.Franchini M, Mannucci PM. Advantages and limits of ADAMTS13 testing in thrombotic thrombocytopenic purpura. Blood Transfus. 2008;6(3):127–35. doi: 10.2450/2008.0056-07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hovinga JA, Vesely SK, Terrell DR, Lammle B, George JN. Survival and relapse in patients with thrombotic thrombocytopenic purpura. Blood. 2010;115(8):1500–11. doi: 10.1182/blood-2009-09-243790. quiz 662. [DOI] [PubMed] [Google Scholar]
- 7.Pereira A, Mazzara R, Monteagudo J, Sanz C, Puig L, Martinez A, et al. Thrombotic thrombocytopenic purpura/hemolytic uremic syndrome: a multivariate analysis of factors predicting the response to plasma exchange. Ann Hematol. 1995;70(6):319–23. doi: 10.1007/BF01696619. [DOI] [PubMed] [Google Scholar]
- 8.Rose M, Eldor A. High incidence of relapses in thrombotic thrombocytopenic purpura. Clinical study of 38 patients. Am J Med. 1987;83(3):437–44. doi: 10.1016/0002-9343(87)90753-4. [DOI] [PubMed] [Google Scholar]
- 9.Rock G, Kelton JG, Shumak KH, Buskard NA, Sutton DM, Benny WB. Laboratory abnormalities in thrombotic thrombocytopenic purpura. Canadian Apheresis Group. Br J Haematol. 1998;103(4):1031–6. doi: 10.1046/j.1365-2141.1998.01080.x. [DOI] [PubMed] [Google Scholar]
- 10.Patton JF, Manning KR, Case D, Owen J. Serum lactate dehydrogenase and platelet count predict survival in thrombotic thrombocytopenic purpura. Am J Hematol. 1994;47(2):94–9. doi: 10.1002/ajh.2830470206. [DOI] [PubMed] [Google Scholar]
- 11.Rock GA, Shumak KH, Buskard NA, Blanchette VS, Kelton JG, Nair RC, et al. Comparison of plasma exchange with plasma infusion in the treatment of thrombotic thrombocytopenic purpura. Canadian Apheresis Study Group. N Engl J Med. 1991;325(6):393–7. doi: 10.1056/NEJM199108083250604. [DOI] [PubMed] [Google Scholar]
- 12.Bobbio-Pallavicini E, Gugliotta L, Centurioni R, Porta C, Vianelli N, Billio A, et al. Antiplatelet agents in thrombotic thrombocytopenic purpura (TTP). Results of a randomized multicenter trial by the Italian Cooperative Group for TTP. Haematologica. 1997;82(4):429–35. [PubMed] [Google Scholar]
- 13.Wyllie BF, Garg AX, Macnab J, Rock GA, Clark WF. Thrombotic thrombocytopenic purpura/haemolytic uraemic syndrome: a new index predicting response to plasma exchange. Br J Haematol. 2006;132(2):204–9. doi: 10.1111/j.1365-2141.2005.05857.x. [DOI] [PubMed] [Google Scholar]
- 14.Lotta LA, Mariani M, Consonni D, Mancini I, Palla R, Maino A, et al. Different clinical severity of first episodes and recurrences of thrombotic thrombocytopenic purpura. Br J Haematol. 2010;151(5):488–94. doi: 10.1111/j.1365-2141.2010.08385.x. [DOI] [PubMed] [Google Scholar]
- 15.Zheng XL, Wu HM, Shang D, Falls E, Skipwith CG, Cataland SR, et al. Multiple domains of ADAMTS13 are targeted by autoantibodies against ADAMTS13 in patients with acquired idiopathic thrombotic thrombocytopenic purpura. Haematologica. 2010;95(9):1555–62. doi: 10.3324/haematol.2009.019299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zheng XL, Kaufman RM, Goodnough LT, Sadler JE. Effect of plasma exchange on plasma ADAMTS13 metalloprotease activity, inhibitor level, and clinical outcome in patients with idiopathic and nonidiopathic thrombotic thrombocytopenic purpura. Blood. 2004;103(11):4043–9. doi: 10.1182/blood-2003-11-4035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Coppo P, Wolf M, Veyradier A, Bussel A, Malot S, Millot GA, et al. Prognostic value of inhibitory anti-ADAMTS13 antibodies in adult-acquired thrombotic thrombocytopenic purpura. Br J Haematol. 2006;132(1):66–74. doi: 10.1111/j.1365-2141.2005.05837.x. [DOI] [PubMed] [Google Scholar]
- 18.Tsai HM. High titers of inhibitors of von Willebrand factor-cleaving metalloproteinase in a fatal case of acute thrombotic thrombocytopenic purpura. Am J Hematol. 2000;65(3):251–5. doi: 10.1002/1096-8652(200011)65:3<251::aid-ajh13>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 19.Coppo P, Schwarzinger M, Buffet M, Wynckel A, Clabault K, Presne C, et al. Predictive features of severe acquired ADAMTS13 deficiency in idiopathic thrombotic microangiopathies: the French TMA reference center experience. PLoS One. 2010;5(4):e10208. doi: 10.1371/journal.pone.0010208. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Ferrari S, Scheiflinger F, Rieger M, Mudde G, Wolf M, Coppo P, et al. Prognostic value of anti-ADAMTS 13 antibody features (Ig isotype, titer, and inhibitory effect) in a cohort of 35 adult French patients undergoing a first episode of thrombotic microangiopathy with undetectable ADAMTS 13 activity. Blood. 2007;109(7):2815–22. doi: 10.1182/blood-2006-02-006064. [DOI] [PubMed] [Google Scholar]
- 21.DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics. 1988;44(3):837–45. [PubMed] [Google Scholar]
- 22.Dervenoulas J, Tsirigotis P, Bollas G, Pappa V, Xiros N, Economopoulos T, et al. Thrombotic thrombocytopenic purpura/ hemolytic uremic syndrome (TTP/HUS): treatment outcome, relapses, prognostic factors. A single-center experience of 48 cases. Ann Hematol. 2000;79(2):66–72. doi: 10.1007/s002770050012. [DOI] [PubMed] [Google Scholar]
- 23.Scheiflinger F, Knobl P, Trattner B, Plaimauer B, Mohr G, Dockal M, et al. Nonneutralizing IgM and IgG antibodies to von Willebrand factor-cleaving protease (ADAMTS-13) in a patient with thrombotic thrombocytopenic purpura. Blood. 2003;102(9):3241–3. doi: 10.1182/blood-2003-05-1616. [DOI] [PubMed] [Google Scholar]
- 24.Eymin G, Andrade M, Andresen M, Pereira J. Thrombotic thrombocytopenic purpura: experience in 18 cases and literature review. Rev Med Chil. 2008;136(12):1518–27. [PubMed] [Google Scholar]
- 25.Lara PN, Jr, Coe TL, Zhou H, Fernando L, Holland PV, Wun T. Improved survival with plasma exchange in patients with thrombotic thrombocytopenic purpura-hemolytic uremic syndrome. Am J Med. 1999;107(6):573–9. doi: 10.1016/s0002-9343(99)00286-7. [DOI] [PubMed] [Google Scholar]
- 26.Thorin E, Thorin-Trescases N. Vascular endothelial ageing, heartbeat after heartbeat. Cardiovasc Res. 2009;84(1):24–32. doi: 10.1093/cvr/cvp236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.O’Rourke MF. Arterial aging: pathophysiological principles. Vasc Med. 2007;12(4):329–41. doi: 10.1177/1358863X07083392. [DOI] [PubMed] [Google Scholar]
- 28.Cohen JA, Brecher ME, Bandarenko N. Cellular source of serum lactate dehydrogenase elevation in patients with thrombotic thrombocytopenic purpura. J Clin Apher. 1998;13(1):16–9. doi: 10.1002/(sici)1098-1101(1998)13:1<16::aid-jca3>3.0.co;2-c. [DOI] [PubMed] [Google Scholar]
- 29.Berkowitz LR, Dalldorf FG, Blatt PM. Thrombotic thrombocytopenic purpura: a pathology review. JAMA. 1979;241(16):1709–10. [PubMed] [Google Scholar]
- 30.Patschan D, Witzke O, Duhrsen U, Erbel R, Philipp T, Herget-Rosenthal S. Acute myocardial infarction in thrombotic microangiopathies--clinical characteristics, risk factors and outcome. Nephrol Dial Transplant. 2006;21(6):1549–54. doi: 10.1093/ndt/gfl127. [DOI] [PubMed] [Google Scholar]
- 31.Hawkins BM, Abu-Fadel M, Vesely SK, George JN. Clinical cardiac involvement in thrombotic thrombocytopenic purpura: a systematic review. Transfusion. 2008;48(2):382–92. doi: 10.1111/j.1537-2995.2007.01534.x. [DOI] [PubMed] [Google Scholar]
- 32.Hughes C, McEwan JR, Longair I, Hughes S, Cohen H, Machin S, et al. Cardiac involvement in acute thrombotic thrombocytopenic purpura: association with troponin T and IgG antibodies to ADAMTS 13. J Thromb Haemost. 2009;7(4):529–36. doi: 10.1111/j.1538-7836.2009.03285.x. [DOI] [PubMed] [Google Scholar]
- 33.Clark WF, Forzley BR, Sontrop JM, Kadri A, Moist LM, Suri RS, et al. TTP/HUS: observational studies generate hypotheses that lead to randomized controlled trials. Kidney Int Suppl. 2009;112:S50–1. doi: 10.1038/ki.2008.621. [DOI] [PubMed] [Google Scholar]
- 34.Noris P, Balduini CL. Investigational drugs in thrombotic thrombocytopenic purpura. Expert Opin Investig Drugs. 2011;20(8):1087–98. doi: 10.1517/13543784.2011.588599. [DOI] [PubMed] [Google Scholar]