

Abstract
Objective:
To assess the quality of diabetic care in Al-Asyah primary health care (PHC) center, Qassim region, KSA , through an auditing of structure, process, and outcome.
Methodology:
The files of all registered diabetic patients in this PHC center were reviewed. The indicators for structure were evaluated according to the National Quality Assurance protocol and manual of chronic diseases, and those for process were assessed by a modified scoring system. The outcome indicators were evaluated using the recommendations of American Diabetic Association (ADA) 2002.
Result:
Dietician, diabetic educator and Hb A1C, HDL level, LDL level were the most common non available resources. Out of 4628 patients registered in this PHC center, only 159 patients had diabetes. The prevalence of diabetes among registered adults aged 15 years and above was 5.8% and this increased with age. The patients were mostly Saudi (96.2%) and married (75.5%). They included 83 females (52.2%). The mean age was 56 years. Most of the patients were Type 2 (95.6%) and most were diagnosed at the PHC center (94.3%). The mean duration of the diabetes since diagnosis was 6.4 years. All checked process items showed high percentages of coverage (73% and above) except for the examination of the fundus, and the measurement of the triglyceride levels. Results showed that most of the samples were obese or overweight (49.7% and 32.7% respectively). While 21.4% had good diabetic control, 42.8% had poor diabetic control. Patient compliance to appointment was good (98.1%), and 13% of the diabetic patients had at least one reported complication.
Conclusion:
This study proves that some essential resources needed for diabetic care were inadequate. Provision of these resources is essential for the improvement of the quality of health care for diabetic patients. Also, there is a need to improve the referral system and establish an appropriate health education program to encourage patients, their families and the community to follow a more healthy life-style.
Keywords: Diabetic care, Audit, process, outcome, Qassim, PHC, Al Asyah
INTRODUCTION
Diabetes mellitus (DM) is a worldwide major public health problem.1 Approximately 150 million people worldwide have DM and that number may be doubled by the year 2025. Much of this increase will occur in developing countries and will be due to population growth, aging, unhealthy diet, obesity and a sedentary life style.2
DM has become a major health problem in Saudi Arabia and other Gulf countries as a result of the rapidly developing economy, high per capita income and evolving western life-style. Diabetes mellitus is the price for urbanization, and the modern life-style.3,4
The true prevalence of DM in Saudi Arabia is unknown but according to some studies carried out in the Kingdom, it has been found to affect 11.8 % of the male population and 12 % of females.5 Another study in Al-Baha reported a prevalence rate of 10.6% in adult males more than 14 years of age and 13.5% in adult females more than 14 years old.6
Recent researches provide clear evidence of the potential for the adequate treatment of diabetes to delay or even prevent such long-term complications as blindness, renal failure, heart attack and even gangrene and amputation of the limbs.7,8 In the UK, since 1970, general practitioners (GPs) have assumed responsibility for the care of diabetics.9 Their vital involvement is recognized and is based on the fact that diabetic control could be as good as that found in hospital clinics. Studies from the central and southern regions of Saudi Arabia have shown that diabetic care could be given at the primary health care (PHC) setting when there is adequate structure in place and the main obstacles are removed.10–12
The objective of this study is to assess the quality of diabetic care in Al-Asyah PHC center, Al Qassim region, Saudi Arabia through the auditing of structure, process, and outcome.
METHODOLOGY
Al-Asyah is a small town in the Al Qassim region served by Al Asyah primary health care (PHC) center, the only PHC center in Al-Asyah. The registered population was 4628 (4414 Saudi and 214 non-Saudi). One of the clinics in this PHC center selected and equipped as a chronic disease clinic, started operating in October 1999. This mini-clinic cares for diabetic, hypertensive and asthmatic patients. The indicators for structures were evaluated according to National Quality Assurance Protocol and manual of chronic diseases.13,14 The indicators for the process of diabetic care were assessed using the Chesover Modified Scoring System.15 The outcome indicators were evaluated based on the recommendations of American Diabetic Association (ADA) 2002.16
The files of all diabetic patients registered in the PHC center were reviewed. Data were collected by the authors during the period of February to May 2003, using pre designed forms consisting of two parts. Part I included the degree of availability of essential resources for the care of diabetes (manpower, chronic diseases register, files, ECG machine, blood pressure apparatus, ophthalmoscope, stethoscope, weighing scale, important laboratory investigations, health education materials, protocol for the management of DM, diabetic cards, medications and appointment system). Part II included the process and outcome measures. The process included; patient characteristics such as age, sex, nationality, marital status, education, and occupation. Besides relevant history such as duration, type, severity of DM, type of treatment, referral to the hospital, risk factors namely hypertension, family history of DM, smoking, obesity, hypercholesterolemia, hypertriglyceridemia, sedentary life style were asked for.
Information on regular health measurements such as blood pressure, body mass index, urine dipstick, fundus examination, FBS, creatinine, cholesterol and triglyceride levels, ECG and chest X-ray was elicited. Outcome measures also included the degree of patient control, creatinine level, and compliance with appointment to the diabetic mini-clinic. Information on the presence of complications such as diabetic foot, diabetic retinopathy, diabetic nephropathy, diabetic neuropathy, impotence, cardiovascular diseases and diabetic coma were recorded.
Exercise is perhaps the single most important lifestyle intervention in diabetes as it is associated with improved glycaemic control, insulin sensitivity, cardiovascular fitness and remodeling. In this study, it is defined as aerobic exercise such as a brisk walk of at least 20 minutes every 48 hours (three times per week).17 In contrast, sedentary lifestyle is defined 20 minute sessions of pleasure time physical activity less than three times per week.18
Hemoglobin A1C is very important in the evaluation of patient control, but it was not available at the PHC center, so the average fasting blood glucose over the last three months was used to assess the degree of diabetic control using the same level of fasting blood sugar reported in the criteria of ADA 2002.16 Statistical package for the Social Science program (SPSS) was used to analyze the data collected.
RESULTS
Essential resources needed for diabetic care except a dietician, diabetic educator and some facilities for investigations such as Hb A1C, HDL level, LDL level and urine micro albumin were available.
Of the 4628 people registered in this PHC center, only 159 patients had diabetes. The prevalence of diabetes among registered adults aged 15years and above was 5.8% and this increased with age.
Table 1 shows demographic characteristics of the studied group. The patients who were mostly Saudis (96.2 %), married (75.5 %), and illiterate (62.9 %), included 76 males (47.8 %) and 83 females (52.2 %). The mean age was 56 years. Seventy seven (48.4 %) were housewives, 24 (15. 0 %) were professionals, 9 (5.7 %) were semi-professionals, 10 (6.3 %) were non skilled workers and 37(23.3 %) were unemployed. About 68% had a positive family history of diabetes, 134 (84.3 %) were non smokers and 110 (69.2%) had a sedentary lifestyle.
Table 1.
Demographic characteristics of diabetic patients in Al Asyah PHC center, 2003
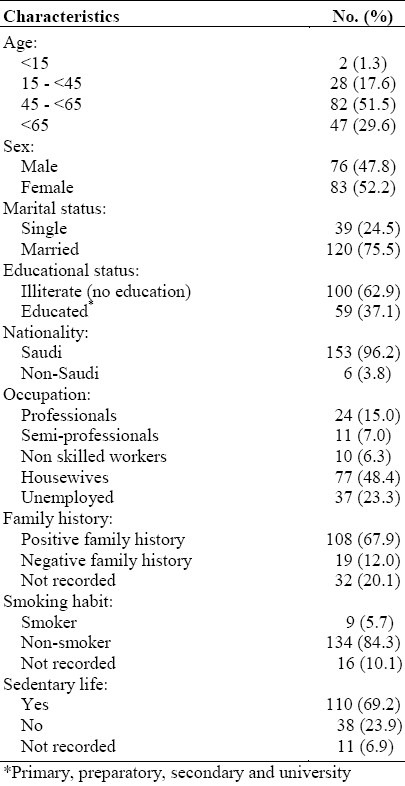
Table 2 shows the distribution of registered diabetic patients according to age group and sex. About 81% of the registered diabetic patients were 45 years of age and above.
Table 2.
Distribution of registered diabetic patients according to age group and sex in Al Asyah PHC center, 2003
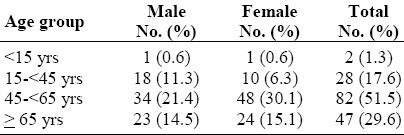
Table 3 shows that most of the patients were diagnosed as Type2 diabetes (95.6%), and most had been diagnosed at Al Asyah PHC center (94.3%). Duration of the diabetes since diagnosis was < 5 years (in 47.8 %), 5–10 years (in 32.7 %), >10years (in 19.5 %), and the mean duration was 6.4 ± 5 years. One hundred twenty six patients (79.2 %) were managed by diet, exercise and oral hypoglycemic drugs, and eighty seven cases (54.7%) had regular follow-ups in the PHC center, while 70 cases (44 %) had regular follow-ups in both PHC and hospital.
Table 3.
Disease characteristics of diabetic patients in Al Asyah PHC center, 2003
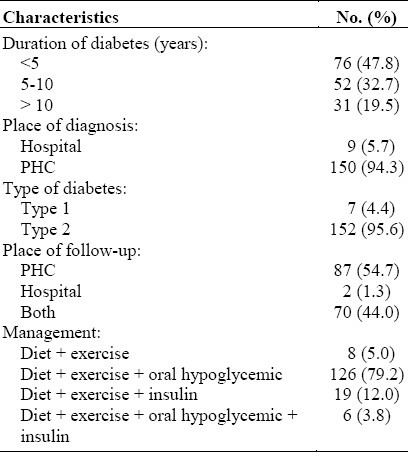
Table 4 shows the results of the completed process measures. All the items of the process showed higher percentages of coverage, except fundus examination (17.6%).
Table 4.
Process measures completed for diabetic patients in Al-Asyah PHC center, 2003
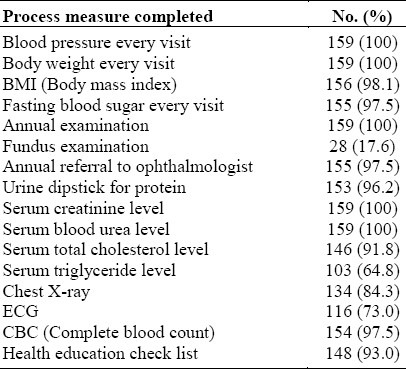
Table 5 shows the results of health outcome measures. Serum urea and creatinine level were normal in most patients, while serum cholesterol and triglyceride level were high in 44% and 21.4% respectively. Moreover, most patients were obese or overweight 49.7% and 32.7% respectively, and 58 patients (35.2%) had hypertension. ECG, Chest X- Ray and fundus examination showed variable levels of abnormality. Patient compliance to appointment was good (98.1%). However, only 21.4% of the patients had excellent diabetic control.
Table 5.
Health outcome measures among diabetic patients in Al-Asyah PHC center, 2003
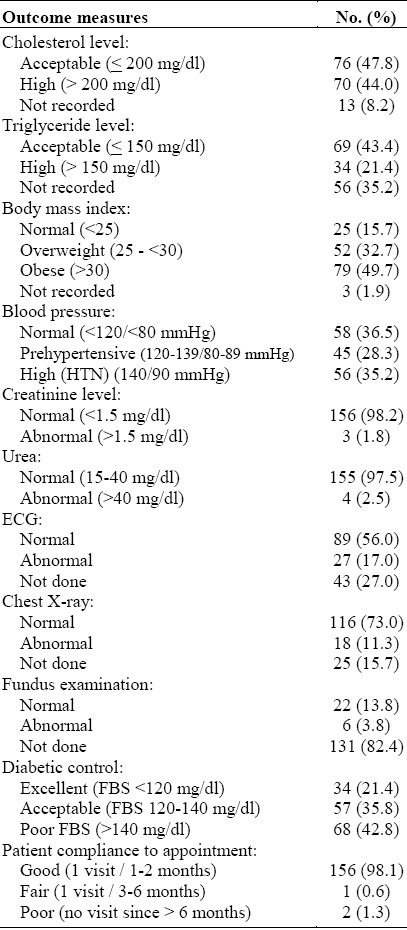
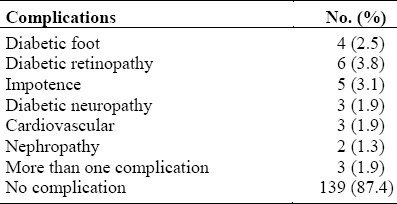
Table 6 shows that approximately 13% of the diabetic patients had at least one reported complication. The most commonly recorded one was diabetic retinopathy.
Table 6.
Distributions of complications in diabetic patients attending Al-Asyah PHC center, 2003
DISCUSSION
The care of diabetic patients at PHC centers should be appropriate, achievable and relevant. Early diagnosis of diabetes, patient education and regular follow-ups through a structured system of surveillance are better carried out in primary health care clinics.13
Audits of structure, process, and outcome of diabetic care at PHC centers are necessary and the most essential resources required for the follow-up of chronic diseases at PHC level should be available in order to provide good health care for these patients.14 In our study, we found that some essential resources required for diabetic care were inadequate at Al-Asyah PHC center. For example, there was no dietician, diabetic educator, and important laboratory investigations such as Hb A1C, HDL level, and LDL level and urine micro albumin were unavailable. Prevalence of diabetes among registered adults aged 15 years and over was 5.8% and this increased with age. It was 19% in males and 21% in females aged 45 - <65 years, reaching 35.4% in males and 38.1% in females aged ≥ 65years. This in accord with the results of previous studies done in Saudi Arabia.6,15
Our study revealed that the data base information namely demographic and diabetes-related was available in most of the files of diabetic patients (97 %). This was in accord with the Al-Khaldi study in Abha.21 One hundred patients (62.9 %) were illiterate. This may relate to the fact that 81% of diabetics 45 years of age and above, (52.2 %) were female, most of whom were housewives. Well-organized diabetic clinics together with the availability of diabetic registers, management protocols, and diagnostic instruments would result in good diabetic care.22 This study revealed that all the items of the process showed high percentages of coverage with a mean of 88%, which was higher than the result of Al- Khaldi and Al- Khattab studies .21,23
Obesity is one of the most prevalent nutritional disorders in Saudi Arabia.21 Overweight and obesity are risk factors that coexist amongst diabetics and hypertensive patients, and form an important focus for the treatment and prevention of DM and hypertension.5,24–27 Our study showed high percentages of overweight and obesity among the diabetic patients (32.7%) and (49.7%) respectively. This agreed with the previous studies done by El Hazmi, Al Nuaim, Al Humaidi and Al Turki.28,31 Diabetic patients should be educated on the role of weight reduction and role of exercises as important determinants of well-being and good diabetic control. This study showed that 36.5% of the patients had normal blood pressure, 28.3% were prehypertensive and (35.2%) had hypertension. This agrees with the results of the Elzubier study which found that 19.9% of diabetic patients had high normal blood pressure and 35% had hypertension.32
It is now widely accepted that the burden of caring for diabetics should be shared between the PHC and tertiary health care through a good referral system. Referral of all diabetic patients to the hospital for annual follow-ups in an ophthalmology clinic and other clinics as indicated is mandatory. Fundus examination is an easy procedure which can give an early diagnosis of diabetic retinopathy, thus averting blindness. In this study, the percentage of annual referrals was 97.5%. In spite of this, the percentage of available data about fundus examination in diabetic files is only 17.6%. This result matches the Lafita study which reported an absence of exploration of lesions of the fundus of the eye in more than 50 % of type2 diabetics.33 However, our results were low in comparison with those of Khattab, Al Khaldi and Qureshi studies.11,21,23 Variation between the number of referrals and the availability of fundoscopy reports in patients’ files may be attributed to poor coordination between referral hospital and PHC center, and poor compliance of patients with the referral system.10
Compliance with follow-up appointments in Al Asyah PHC diabetic clinic was high (98.1%). This is higher than the results of Al-Khaldi and Al-Khattab studies.16,17 This may be due to the fact that diabetic drugs prescribed to the patients from the PHC or the hospital in Al Qassim region were given to the patients through the PHC centers only. Good diabetic control is the main objective of care. Our results show that excellent diabetic control was 21.8% and poor diabetic control was 42.8%. However, these figures are below the national standard (>40% should have good glycemic control and <10% have poor control).13 In comparison, the good glycemic control of diabetes was higher than what was reported in the Al–Khaldi and Asser studies.21,22 Diabetic control may be improved through the education of the diabetic patients on the importance of diet, drugs, exercise, and importance of compliance with treatment and appointments.
Allocation of time or protected time is the cornerstone of the organization of the mini clinic. This enables the PHC center physician to make an early diagnosis and effectively manage any complications. Approximately, 13 % of the diabetic patients had at least one reported complication. Diabetic retinopathy was the most common reported complication (3.8 %), which is lower than what was reported by the Al Owayyed, Al Khaldi and Khattab studies.12,21,23 This could be attributed to the low rate of fundoscopy performed. Only 2.5% of the registered diabetic patients had reported a diabetic foot. This was still higher than the results reported by Khattab, Al Owayyed, Al Khaldi studies.13,21,23 The rates of neuropathy (1.9%), cardiovascular diseases (1.9%), and nephropathy (1.3%) were lower than those reported by Al Owayyed and Al Khaldi studies.12,21 Diabetes mellitus is the main risk factor for impotence in Saudi patients.34 It was reported in 3.1% of diabetic patients, a result that is comparatively lower than those of the Kattan and Al Khaldi studies.34,21 The reason for low prevalence of impotence in our study could be the lack of reporting because of the social stigma (feeling of shame or embarrassment on part of patient) attached to this condition.
REFERENCES
- 1.Al – Lwaiti JA. Diabetes in Oman. Annals of Saudi Medicine. 2000;20(1):12–5. doi: 10.5144/0256-4947.2000.12. [DOI] [PubMed] [Google Scholar]
- 2.WHO Fact sheet. Diabetes mellitus. Saudi Med J. 2000;21(1):118–23. [Google Scholar]
- 3.Mahfouz AAR, Al Aakija W, Al Erian RA, Al Khzayem AM. Diabetes Mellitus in the Asir region, Saudi Arabia; prevalence at primary health care level. Health Services Journal of Eastern Mediterranean Region. 1993;l7(2):15–8. [Google Scholar]
- 4.Famuyiwa OO, Sulimani RA, Laajam MA, Al- Jasser SJ, Mekki MO. Diabetes Mellitus in Saudi Arabia, the clinical pattern and complications in 1,000 patients. Annal of Saudi Medicine. 1992;12(2):140–51. doi: 10.5144/0256-4947.1992.140. [DOI] [PubMed] [Google Scholar]
- 5.Al-Nuaim AR, Al-Mazrou Y, Al- Atass O, Al Rubean K, Khoja TA, Al Dhaghari N. Ministry of Health and King Saud University; 1995. National chronic metabolic disease survey part I. Prevalence of diabetes mellitus, obesity and hypercholesterolemia in Saudi Arabia in Riyadh (K.S.A) pp. 1–68. [Google Scholar]
- 6.El–Hazmi MAF, Warsy AS, Barimah NA, Al–Swailem AR, Al–Swailem A, Sulaimani R, Al–Meshari A. The prevalence of Diabetes Mellitus and Impaired glucose tolerance in population of Al Baha, Saudi Arabia. Saudi Med J. 1996;17(5):591–6. [Google Scholar]
- 7.WHO Fact sheet. Diabetes mellitus. Saudi Med J. 2002;23(5):612–5. [Google Scholar]
- 8.Charles M, Clark JR, Anthony LD. Prevention and treatment of complication of diabetes. N Engl J Med. 1995;332:1210–7. doi: 10.1056/NEJM199505043321807. [DOI] [PubMed] [Google Scholar]
- 9.Thorn PA, Russell RG. Diabetic clinics today and tomorrow: Mini clinics in general practice. BMJ. 1973;2:534–6. doi: 10.1136/bmj.2.5865.534. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Khattab M, Alakija W, Abolftouh M, Humaidi M, Al-Tokhy M, Al-Khaldi Y. Obstacles to and solutions for optimal implementation of primary care for diabetes in Abha, Asir Region.Saudi Arabia. Saudi Med J. 1997;18:236–9. [Google Scholar]
- 11.Qureshi RH, Al-Owayyed A. An Audit of the process of diabetic care in a large family practice in Riyadh. Saudi Med J. 1995;16:494–7. [Google Scholar]
- 12.Al- Owayyed A, Al- Shikh A, Taha S. A survey and audit of diabetic care in alarge family practice in Riyadh. Saudi Med J. 1997;18:175–9. [Google Scholar]
- 13.Riyadh, Saudi Arabia: 1994. Quality Assurance in Primary Health Care Manual. MOH G.D. of health centers, WHO / EMRO; pp. 199–233. [Google Scholar]
- 14.Khoja TA. Manual of care of chronic diseases patients at PHCC (Specialized clinics) First Edition. Riyadh, K.S.A: 2001. Apr, Scientific Committee. [ Arabic Edition ] [Google Scholar]
- 15.Chesover D, Tudor Miles P, Hilton S. Survey and Audit of diabetic care in general practice in South London. Br J Gen pract. 1991;41:282–5. [PMC free article] [PubMed] [Google Scholar]
- 16.Sandards of medical care patients with diabetes mellitus. American Diabetes Association. Diabetic Care. 2002;(suppl 1):S33–S49. doi: 10.2337/diacare.26.2007.s33. [DOI] [PubMed] [Google Scholar]
- 17.Buse Johb B, Polonsky Kenneth S, Burant Charles F. Williams Textbook of Endocrinology. Tenth Edition. Saunders Company Philadelphia, Pensylvania: 2003. Type 2 Diabetes Mellitus; p. 1459. [Google Scholar]
- 18.Robert FA, Michael MSN, Waller KG, Wooten EEM, Luis GE, Lee MS. Behavioral Risk factor surveillance. Surveillance Summaries, CDC. 1990 Jun 01;39(SS-2):1–6. [PubMed] [Google Scholar]
- 19.Al-Sharif Al, Al-Khaldi YM. Resource availability for care of hypertensives at primary health settings in Southwestern Saudi Arabia. Saudi Med J. 2003;24(5):466–71. [PubMed] [Google Scholar]
- 20.Khoja TA, Farid SM. Riyadh: Ministry of Health; 2000. Saudi Arabia Family health survey 1996: principal Report. [Google Scholar]
- 21.Al-Khaldi YM, Khan MY. Impact of a mini – clinic on diabetic care at a primary health care center in southern Saudi Arabia. Saudi Med J. 2002;23(1):51–5. [PubMed] [Google Scholar]
- 22.Khattab M, Abolfotouh M, Alakija W, Humaidi M, Al-Tokhy M, Al-Khaldi Y. Audit of diabetic care in an Academic family practice center in Asir Region Saudi Arabia. Diabetes Res. 1996;31:243–54. [Google Scholar]
- 23.Khattab M, Al-Khaldi, Abolfotouh M, Khan MY, Humaidi M, Alakija W, Al-Tokhy M. Impact of a diabetic program in a family practice center in Asir Region Saudi Arabia. Diabetic Res. 1998;33:115–27. [Google Scholar]
- 24.Anderson KM, Wilson PW, Odell PM, Kannel WB. An updated coronary risk profile: A statement for health professionals. Circulation. 1991;83:356–62. doi: 10.1161/01.cir.83.1.356. [DOI] [PubMed] [Google Scholar]
- 25.National Cholesterol Education Program (NCEP1) The Expert panel. Second report of the Expert Panel on detection, evaluation and treatment of high blood cholesterol in adults. Circulation. 2002;106(25):3140–1. [PubMed] [Google Scholar]
- 26.Manson JE, Colditz GA, Stampfer MJ, Willett WC, Rosner B, Monson RR, et al. A prospective study of the obesity and risk of coronary heart disease in women. N Engl J Med. 1990;322:882–9. doi: 10.1056/NEJM199003293221303. [DOI] [PubMed] [Google Scholar]
- 27.Pi Sunyer FX. Medical hazards of obesity. Ann Intern Med. 1993;119:655–60. doi: 10.7326/0003-4819-119-7_part_2-199310011-00006. [DOI] [PubMed] [Google Scholar]
- 28.EL Hazmi MAF, Warsy AS. Prevalence of obesity in Saudi population. Annals of Saudi Medicine. 1997;17:302–6. doi: 10.5144/0256-4947.1997.302. [DOI] [PubMed] [Google Scholar]
- 29.Al–Nuaim AR. High prevalence of metabolic risk factor for cardiovascular diseases among Saudi population aged 30-64 years. Int J Cardiol. 1997;62:227–35. doi: 10.1016/s0167-5273(97)00268-4. [DOI] [PubMed] [Google Scholar]
- 30.Al Humaidi MA. Obesity and associated risk of coronary artery disease among patients of primary health care centers, in Abha, Saudi Arabia. Journal of Family and Community Medicine. 2000;7(1):25–30. [PMC free article] [PubMed] [Google Scholar]
- 31.Al Turki YA. The prevalence of overweight and obesity amongst hypertensive and diabetic adult patients in primary health care. Saudi Med J. 2000;21(4):340–3. [PubMed] [Google Scholar]
- 32.Elzubier AG. Hypertension in Diabetics registered in primary health care center in Makkah district, Saudi Arabia. Journal of Family & community Medicine. 2000;7(3):23–8. [PMC free article] [PubMed] [Google Scholar]
- 33.Lafita J, Aragon L, Berraondo C, Diez J, Garcia Del Rio J, Rodriguez C, et al. Continuous quality improvement in the control of the type 2 diabetes in Navarra. Bedpans Study, 1996. An Sist Sanit Navar. 1999;22(1):59–70. doi: 10.23938/ASSN.0694. [Spanish] [DOI] [PubMed] [Google Scholar]
- 34.Kattan SA. Impotence in Saudi males – etiology and risk factors. Saudi Med J. 1996;17:350–65. [Google Scholar]