

Abstract
Acute appendicitis is a common cause of acute abdomen. However, it is a rare cause of pneumoperitonium. In this report the surgical diagnoses and management will be discussed in detail.
Keywords: Acute abdomen, peritoneum
INTRODUCTION
Acute appendicitis is one of the most common surgical diagnoses in acute abdomen.1 Although, its clinical features are straight forward, sometimes they could be confused, particularly, if history taking was difficult or plain X-ray of the abdomen showed rare relevant findings such as pneumoperitonium.
CASE REPORT
A 30-year-old Indian male was brought to the Accident and Emergency Department of King Khalid Hospital in Al-Kharj with a history of abdominal pain which was steadily increasing with nausea but there was neither vomiting nor fever. There were no previous abdominal symptoms and no history of drug use. Initial examination showed normal vital signs as follows: temperature 37°C, pulse 80/min, blood pressure 120/80mmHg.
Physical examination revealed the following: The patient was ill and mildly dehydrated. There was generalized abdominal tenderness and guarding, bowel sounds were absent, but per-rectal examination was normal. Chest and heart were unremarkable.
On admission, investigations revealed the following results: CBC showed mild leukocytosis 14.300, serum bilirubin was 1.5mg/dl. X-ray chest showed gas under the right diaphragm (Figure 1). Based on this data, the diagnosis of perforated peptic ulcer was made.
Figure 1.
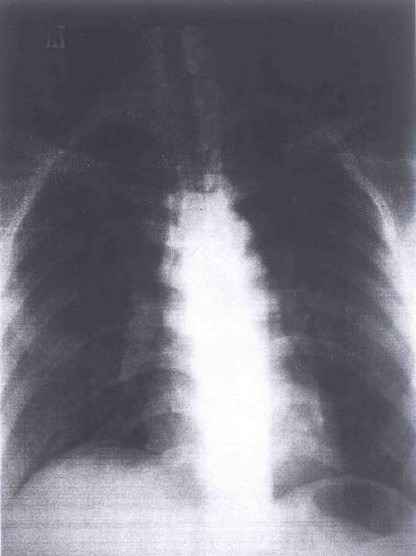
Chest X-ray
Management of the case started with the correction of dehydration with crystalloid solution, and patient was moved to the operating room for exploratory laparotomy. The abdomen was opened by an upper mid line incision. Turbid foul-smelling fluid in the pelvis was noted. Swab was taken for culture and sensitivity. The appendix was found to be gangrenous and perforated at its tip and adherent to the sigmoid colon and ileum. The stomach, duodenum and all other structures were normal. Appendicectomy was done, peritoneal toilet was carried out and the abdomen was closed. Postoperative period was uneventful.
The pelvic fluid swab for culture and sensitivity showed E. Coli. Histopathology confirmed gangrenous perforated appendix. Patient was discharged from the hospital on 6th postoperative day.
DISCUSSION
Perforated appendix is a common complication of acute appendicitis with an estimated incidence of 20%.1 However, pneumoperitoneum is rarely found in association with perforated appendicitis. Few articles have been published in medical literature about this subject since first case was reported by Gulleurin in 1923 quoted by Sabeo.2 A study conducted in Portland to find the reasons for pneumoperitonium among patients with intrabdominal ruptured or perforated viscus did not reveal a single case caused by perforated appendicitis.3 The reason for the low incidence includes inadequate reporting and the absence of X-ray studies as emphasized by Farman et al and Harned.4,5
Although most pneumoperitoneum occur as perforated peptic ulcer, it is important not to miss the perforated appendix as a cause for this condition, particularly if exploratory laparotomy shows normal stomach and duodenum as seen in this case. The site of perforation of the appendix in this case was at the tip. This finding was similar to that mentioned by Cannova et al.6
The culture of peritoneal fluid revealed E.Coli, whereas Katz et al mentioned a mixed growth of streptococcus bovi, type II, bacteroides species.7 To our best knowledge, this is the first case of appendicitis with pneumoperitoneum reported in the Kingdom of Saudi Arabia.
ACKNOWLEDGMENT
My appreciation goes to Dr. Mohammed Ashfaque Khan for his help in typing the draft of this report.
REFERENCES
- 1.Tierney LM, McPhee SJ, Papadakis MA. Current Medical Diagnosis & Treatment. 37th edition. Stamford (UK): Appleton & Lange; 1998. pp. 600–601. [Google Scholar]
- 2.Saebo A. pneumoperitonium associated with perforated appendicitis. Acta Chir Scand. 1978;144(2):115–7. [PubMed] [Google Scholar]
- 3.Winek TG, Mosely HS, Grout G, Luallin D. Pneumoperitoneum and its association with ruptured abdominal viscus. Arch Surg. 1988;123(6):709–12. doi: 10.1001/archsurg.1988.01400300051008. [DOI] [PubMed] [Google Scholar]
- 4.Farman J, Kassner EG, Dallemand S, Stein HD. Pneumoperitoneum and appendicitis. Gastrointest Radiol. 1976;1(3):277–9. doi: 10.1007/BF02256380. [DOI] [PubMed] [Google Scholar]
- 5.Harned RK. Retrocecal appendicitis presenting with air in the subhepatic space. Am J Roentgenol. 1976;126(2):416–8. doi: 10.2214/ajr.126.2.416. [DOI] [PubMed] [Google Scholar]
- 6.Cannova JV, Krummen DM, Nicholson OO. Pneumoperitoneum in association with perforated appendicitis. Am Surg. 1995;61(4):324–5. [PubMed] [Google Scholar]
- 7.Katz E, Engelhard D, Kerem E, Eid A, Berlatzki Y. Coma in an unusual case of perforated appendicitis with pneumoperitoneum. J Pediatr Surg. 1987;22(11):1017–8. doi: 10.1016/s0022-3468(87)80503-1. [DOI] [PubMed] [Google Scholar]