

Abstract
Objective:
To determine the incidence, characteristics and the different factors associated with diarrhea events reported at the Primary Health Care (PHC) level in children under five years of age.
Material and methods:
All reported cases of diarrhea in children under 5 in the primary health care (PHC) center of Wasat Abha, Abha city during the year 2002. The medical records of patients were reviewed for name, sex, date, duration of diarrhea and character of stool, type of feeding, degree of dehydration, the treatment received and the outcome.
Results:
The overall incidence /child/year 2002 was 1.2 episodes. The total number of diarrhea episodes in that age group was 573 cases giving an incidence rate of 9.9% for the year 2002.
Two thirds of the episodes of diarrhea (64.6%) occurred in females, and 60.9% of the episodes affected 7-12-month olds. The majority of diarrhea episodes (89.4%) lasted less than 7 days and only 3.7% of cases were moderately dehydrated. Ninety four percent of the cases improved and only 1.7 % were admitted to the hospital.
Conclusion:
The incidence of diarrhea episodes in the under fives in the year 2002 was lower than the national rate reported in 1993. Female children had about twice the incidence of diarrhea in male children and the highest incidence was observed in the 7-12-month olds. The majority of cases were acute. It is recommended that studies on the incidence of diarrhea in all PHC centers be done in order to monitor the progress of diarrhea in children and implement suitable preventive measures.
Keywords: Incidence, diarrhea, Primary Health Care, Children
INTRODUCTION
Diarrhea remains a major cause of mortality and morbidity in children up to 5 years of age in developing countries, where it ranks the first or second most common cause of death.1,2 Preschool children in these countries have diarrhea for about 35 – 70 days each year3 and some studies4 have shown that they may have up to 3 to 10 episodes of diarrhea each year during the first 5 years of life. Moreover, the consequences of diarrhea in terms of childhood nutrition, development, overall health and survival are substantial.
Some studies done in Saudi Arabia,5,6 to examine the epidemiology of diarrhea in referral hospitals in Jeddah, Taif and Riyadh showed that the prevalence in some cases amounted to 25%, with up to 6 episodes/child/year. A good proportion (41.3%) of cases was due to Rotavirus with a peak incidence in the age of 6-14 months of bottle-fed babies. However, another study7 demonstrated various pathogens among young children with different stool characteristics such as E. coli (13%), Gardia (3.1%), Salmonella (3%) and Shigella (2.6%). The study concluded that this type of infection denotes that diarrhea in children is still a significant public health problem in Saudi Arabia.
In 1980, WHO started the Diarrhea Disease Control Program with the objective of decreasing diarrhea mortality and morbidity among young children in developing countries.8,9 The strategies of the program to prevent diarrhea morbidity, rely on factors believed to be peculiar to the cultural and economic conditions prevailing in the community. These include the promotion of breast feeding and weaning practices, the use of safe water, good personal and domestic hygiene and complete immunization schedule.
The aim of this study was to depict the incidence, characteristics and the different factors associated with diarrhea events reported at the Primary Health Care (PHC) level in children under the age of five years.
METHODOLOGY
The National Program of Control of Diarrheal Diseases in Saudi Arabia gets its first information flow from the Primary Health Care (PHC) centers. The PHC physician upon encountering a case of diarrhea has to fill a diarrhea case report which contains the following items: date, registration number, name and sex of the case. The age is categorized into less than 7 months, 7-12 months, 1-5 years and above 5 years. The duration of the diarrhea is defined into less than 7 days, 7-14 days and more than 14 days. The feeding of the child is specified as breast, bottle, mixed feeding or regular food. The stool character is described as watery, mucoid or bloody is recorded. In cases with dehydration, its degree is described as mild, moderate or severe according to WHO guidelines.10 The treatment received is specified: oral rehydration solution (ORS), IV fluids or others such as, antibiotics or antidiarrheal drugs. Finally, the outcome is mentioned: death, hospitalized, unknown or improved.
This study included all reported cases of diarrhea in children under 5 years in the PHC center of Wasat Abha, Abha, during the year 2002. This center serves a population of 13798 inhabitants that included 2330 families. The number of male children under 5 years were 2997 while female children under 5 years was 2782. All the reports of diarrhea events in this age group (573 cases) during the year 2002 were collected and the different items in the reports were retained and analyzed using the Chi square test at 5% level of significance by the Epi info 2000 statistics program. The study relied solely on the information recorded in the diarrhea reports and the definition of diarrhea adopted in recording the cases, either the mother's or the physician's, could not be verified. Each diarrhea episode was individually considered whether from the same or a different child.
The overall incidence per child per year was counted and the incidence of diarrhea events was calculated for males, females and the different age subgroups. Besides, the percentages of diarrhea events were indicated for the duration of diarrhea, type of feeding, character of the stool, state of dehydration, treatment and prognosis.
RESULTS
Table 1 describes the incidence of diarrhea in the population aged up to 5 years in the PHC center catchment area. It shows that the overall incidence/child/year 2002 was 1.2 episodes while the total number of diarrhea reports in that age group is 573 cases (incidence rate for the year 2002 = 9.9%). The incidence in males was 6.8%, but in females, it was almost twice as much (13.3%), a difference that was statistically significant at p< 0.001. The highest incidence of reported episodes (23.3%) was seen in infants 7-12 months age, while the lowest (3.8%) was in the 1-5 years age group. Again, this difference was statistically significant at p< 0.001.
Table 1.
Incidence of diarrhea episodes in children 5 years and under, according to sex and age during the year 2002 in the PHC center
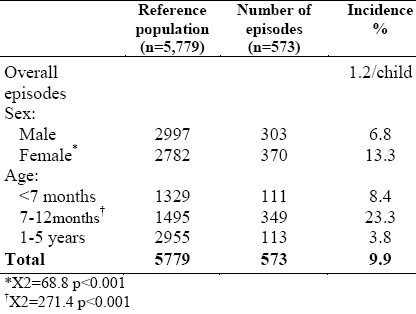
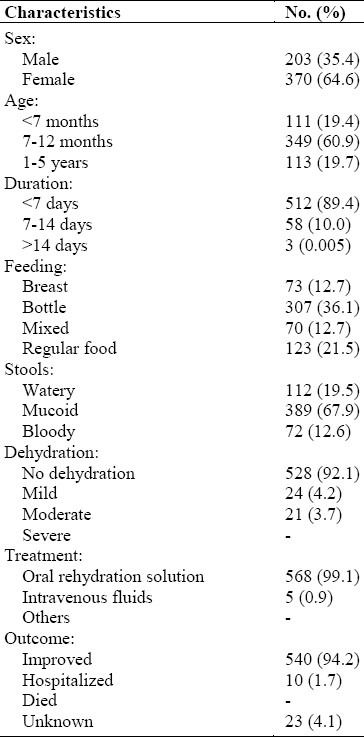
Table 2 shows the percentage of reported episodes of diarrhea for the different items of the report. Thus, two thirds of the episodes (64.6%) occurred in females, and 60.9% of the episodes affected the 7-12 months age group. The majority of diarrhea episodes (89.4%) lasted less than 7days and only 3.7% of the cases were moderately dehydrated. However, 94.2% of the cases improved, and only 1.7% of the cases needed hospitalization. About one third of the cases (36.1%) were bottle-fed, while 12.7% were breast-fed. In 67.9% of the cases, the stools were mucoid; they were watery or bloody in 19.5% and 12.6% of the cases respectively. Only 5 cases (0.9%) needed IV fluids, while all other cases were treated with the ORS treatment.
Table 2.
Description of diarrhea episodes reported in the PHC center during the year 2002 (n=573)
DISCUSSION
The incidence of diarrhea episodes reported in the PHC center in the under 5 age group in the year 2002 was lower (9.9%) than the national rate (18.2%) reported in 1993.11 However, this last figure was based on a questionnaire study eliciting information on diarrhea episodes in children under 5 in a 2-week period prior to the enquiry. Moreover, the incidence per child/year 2002 calculated in the present study was also lower (1.2 episodes/child) compared to this same national study (3.8 episodes/child).12 The Southern region reported rates as high as 15% and 13.7% in both urban and rural areas respectively. The discrepancy between these figures and those of our study might be due to an improvement of the general condition of health in the Kingdom during this last decade on the one hand and underreporting to the PHC center of the mild cases, those treated at home or privately, as well as some severe cases that went directly to the higher levels of care. It is worth noting here that contrary to the national rates, female children have about twice the incidence of diarrhea (13.3%) than male children (6.8%). This might point to a possible cultural influence in this region by which the nutrition of female children is neglected or the restriction of their access to health care. Indeed, studies relying on cases referred to hospitals have shown a higher proportion of males than females.5,13 The highest incidence of diarrhea was observed in the 7-12 months age group pointing to 2 main probable factors; the improper weaning14 of the child. This calls for intensive health education of parents and proper immunization of the child.15 Indeed, at that age, the naturally acquired immunity derived from the mother is waning and infections, viral or bacterial tend to increase especially if the child's immunity is weakened, if he is malnourished or not properly immunized.16
The majority of episodes were acute (89.4%) lasting for less than 7 days, with no dehydration in 92% and were treated by ORS (99.1%). It is expected that patients who report to PHC centers would be those with the type of diarrhea described above, for the more serious cases would probably go to the emergency service in hospitals or to other levels of health care. As several causative agents are implicated in children diarrhea, the stool character was variable ranging from watery (19.5%) to bloody stools (12.6%). Since there is a high incidence of diarrhea in bottle-fed children(36.1%), this might indicate unhygienic methods of food preparation. Besides, 21.5% of the episodes of diarrhea occurred in children on regular food, indicating the need to stress the importance of sound weaning as well as proper hygienic food preparation.17
CONCLUSION AND RECOMMENDATION
The study showed that the incidence of diarrhea in this urban PHC center is lower than the national rate. This latter relies on a study done 10 years ago that is yet to be revised. Health education on food hygiene, proper weaning and some cultural beliefs and practices are to be strengthened. It is recommended that studies on the incidence of diarrhea reported in all PHC centers be done in order to monitor the progress of diarrhea in children and implement the suitable preventive measures.17
ACKNOWLEDGMENT
The authors would like to thank the medical faculty at Wasat Abha Primary Care Centre and the staff at the Department of Medical Records for their valuable help. We also express our gratitude to Mr. Mohammed Alasmi and Mr. Allan I. Agaton for their secretarial assistance.
REFERENCES
- 1.Glass IR, Lew JF, Gangarosa RE, LeBaron CW, Ho MC. Estimates of morbidity and mortality rates for diarrheal diseases in American children. J Pediatr. 1991;118(4):S27–33. doi: 10.1016/s0022-3476(05)81422-2. [DOI] [PubMed] [Google Scholar]
- 2.Jones G, Steketee RW, Black RE, Bhutta ZA, Morris SS. How many child deaths can we prevent this year? Lancet. 2003 Jul 5;362(9377):65–71. doi: 10.1016/S0140-6736(03)13811-1. [DOI] [PubMed] [Google Scholar]
- 3.Mirza MN, Caulfield LE, Black RE, Macharia WM. Risk factors for diarrheal duration. Am J Epidemiol. 1997;146(9):776–85. doi: 10.1093/oxfordjournals.aje.a009354. [DOI] [PubMed] [Google Scholar]
- 4.Kirkwood BR. Diarrhea. In: Feachem RG, Jamison DT, editors. Diseases and mortality in sub-Saharan Africa. Oxford: Oxford University Press; 1990. p. 27. [Google Scholar]
- 5.Milaat WA, Elassouli SM. Epidemiology of diarrhea in two major cities in Saudi Arabia. J Commun Dis. 1995;27(2):84–91. [PubMed] [Google Scholar]
- 6.Bani IA, Saeed AA, Othman AA. Diarrhea and child feeding practice in Saudi Arabia. Public Health Nutr. 2002;5(6):727–31. doi: 10.1079/PHN2002354. [DOI] [PubMed] [Google Scholar]
- 7.El Sheikh SM, Elassoulli SM. Prevalence of viral, bacterial and parasitic enteropathogens among young children with acute diarrhea in Jeddah, Saudi Arabia. J Health Popul Nutr. 2001;19(1):25–30. [PubMed] [Google Scholar]
- 8.Bern C, Martines J, de Zoysa I, Glass RI. The magnitude of the global problem of diarrheal disease: a ten years update. Bull WHO. 1992;70(6):705–14. [PMC free article] [PubMed] [Google Scholar]
- 9.Programme for control of diarrheal diseases: 8th programme report. World Health Organization. 1991 WHO/CDD/92.38. [Google Scholar]
- 10.A manual for the treatment of diarrhea for use by physicians and other senior health workers. World Health Organization. 1990 WHO/CDD/SER/80.2,Rev 2. [Google Scholar]
- 11.Al Mazrou Y, Al Shehry S, Al Jeffri M, Farag MK, Baldo MH, Khan MU, editors. Saudi Maternal and Child survey. Kingdom of Saudi Arabia: Ministry of Health; 1991. pp. 142–162. [Google Scholar]
- 12.Mazrou Y, Farid, editors. Reproductive pattern and Child Survival in Saudi Arabia. Kingdom of Saudi Arabia: Ministry of Health; 1993. pp. 179–207. [Google Scholar]
- 13.Sheth M, Patel J, Sharma S, Seshadri S. Health hazards and critical points of weaning foods. Indian J Pediatr. 2000;67(6):405–10. doi: 10.1007/BF02859455. [DOI] [PubMed] [Google Scholar]
- 14.Ahmed M, Billo AG, Murtaza G. Risk factors of persistent diarrhea in children below five years of age. J Pak Med Assoc. 1995;45(11):290–2. [PubMed] [Google Scholar]
- 15.Scrinshaw NS. Historical concepts of interactions, synergism and antagonism between nutrition and infection. J Nutr. 2003;133:316S–321S. doi: 10.1093/jn/133.1.316S. [DOI] [PubMed] [Google Scholar]
- 16.Moawed SA, Saeed AA. knowledge and practices of mothers about infants’ diarrheal episodes. Saudi Med J. 2000;21(12):1147–51. [PubMed] [Google Scholar]
- 17.Etiler N, Velipasaoglu S, Aktekin M. Risk factors for overall and persistent diarrhea in infancy in Antalya, Turkey: a cohort study. Public Health. 2004;118(1):62–9. doi: 10.1016/S0033-3506(03)00132-X. [DOI] [PubMed] [Google Scholar]