

Abstract
Background:
Early diagnosis and prompt treatment are the basic elements of malaria control. The mother's perceptions about the cause of the fever, duration of sickness, accessibility and the anticipated cost of treatment, frequent use of traditional medicine, and judgement of the severity of the fever are the most important determinants for effective treatment of fever in children.
Subjects and Methods:
This cross-sectional study was conducted in Kassala city, in Eastern Sudan to investigate the caregivers’ care-seeking behaviour related to fever among children < 5 years. Data was collected by trained social workers using a structured questionnaire and was analysed by means of SPSS.
Results:
Three-hundred fifty housewives were interviewed. The majority (85.7%) had had at least basic education and 244 (69.7%) were full-time housewives. A total of 237 (67.7%) mothers were found to have adequate knowledge about malaria. Malaria was perceived by only 143 (40.9%) of the respondents as a cause of low grade fever and this percentage was almost doubled in the case of high fever. There were similar findings with respect to the selection of treatment sources and the use of antimalarial drugs. High fever urged 319 (91.1%) to seek advice from health workers and 281 (80.3%) to take drugs other than chloroquine.
Conclusion:
The intensity of fever (low/ high) governed the respondent's perceived causes of fever, decision about available treatment options and the type of antimalarial drugs they used. Health education programmes should focus on the importance of seeking early advice, compliance with prescribed treatment and awareness and handling of danger signs before presenting at health facility.
Keywords: Malaria, Fever, Treatment-seeking behaviour, Sudan
INTRODUCTION
Health-seeking behaviour refers to the sequence of actions that patients and/or their parents take to solve their problem. The sequence of events begins with the identification of symptoms and then the formulation of a treatment strategy by the head of the household in consultation with other adult family members.1 Health seeking behaviour is not just a one off isolated event. It is an integral part of a person's, a family's or a community's identity, which had evolved from social, personal, cultural and experiential factors.2 A variety of factors have been identified as the leading causes of poor utilization of primary health care services. These include poor socio-economic status, lack of accessibility, cultural beliefs and perceptions, low literacy level of the mothers and large family size.3
Malaria remains a major global problem, taking an enormous toll on the health and economy especially of poor communities. About 60% of malaria cases, more than 80% of malaria deaths and about 18% of deaths in children under 5 years of age occur in Sub-Saharan Africa.4 In Sudan, malaria accounts for 20-40% of all outpatient visits, 30-50% of hospital admission and 15-20% of registered deaths.5
Early diagnosis and prompt treatment are the basic elements of malaria control. They shorten the duration of the disease and prevent the development of complications and a great majority of deaths.6 The mother's knowledge and perceptions about the cause of fever, duration of sickness, accessibility and the anticipated cost of treatment, frequent use of traditional medicine, and the perceived intensity and severity of sickness were the main factors that determined early and effective treatment of children under 5 years.7–10 For instance, in Kenya the above- mentioned determinants made people go through different treatments: self-treatment, public health facilities, private, consultation of herbalists and not doing anything.9 In the Philippines, six treatment categories were identified: self-treatment with western medicine, self-treatment with traditional medicine, presentation at a consultation clinic of traditional healers, coping with the illness without treatment, the use of other methods such as sponging and not doing anything.11 Experience also showed that the majority of mothers managed their child's disease at home and used both traditional and modern treatment,12 after which they took the child to the health facility.13
The present study was conducted in Eastern Sudan to investigate the caregivers’ knowledge and perceived causes of fever. Also the study aimed to explore caregivers’ classification of fever in under 5-year-old children, and describe the sources and types of treatment offered to the children with fever. The results would assist in the reorientation of the ongoing health education programme to improve health-seeking behaviour and practices at home.
SUBJECTS AND METHODS
From January to March 2004, a community-based cross-sectional survey was conducted in Kassala city, Eastern Sudan. Every 8-12 years the area experiences a devastating flood. The last one (August 2002) led to the destruction of 70% of the houses. The area is characterized by variable malaria transmission in two seasons: post-flood in September-October and during the relatively cold period in January-February.14
After taking their consent, the housewives with children under the age of five years were interviewed. The sample size was calculated using the known formula (n=(p*q*Z2)/d2) where (n) is the sample size, (p) is the sample proportion, (q) is equal to (1-p), (Z) is the appropriate cut-off point on the standard normal distribution at 95% confidence and (d) is the degree of precision. Assuming that 70% of the housewives would respond to fever in different ways (p), if (Z) is set as (1.96) at 95% and if the degree of accuracy is taken as 5% (0.05), a total of at least 323 housewives would be needed. The investigators, however, decided to call on 400 households to compensate for refusals, and homes that had no children under five. Using the probability proportion to size, the required sample was obtained from the city's 4 major blocks. Within each block, subjects were obtained by a systematic random allocation.
Data was collected by 4 trained social workers using a structured questionnaire. The questionnaire covered the socio-demographic profile, knowledge about malaria symptoms, the causes of fever from a caregiver's point of view and the treatment options in the case of “mild” and “severe” fever. “Mild/ severe” fever were common terms used by the natives to describe the fever. Knowledge about the symptoms of malaria was considered adequate if the respondent mentioned fever, inadequate if she mentioned other suggestive symptoms but not fever, and considered as lacking knowledge if she mentioned symptoms that bore no relation to malaria.
Data was analysed using SPSS for windows version 10.0. Tables were generated to describe the frequency, percentage and the percentage of differences in relation to the intensity of fever. Cross-tabulation was carried out to test association between caregivers, knowledge about fever and the education level, and occupation separately. Also the association between the level of education and selecting from the available treatment options was tested. Chi-square test was computed and the association was considered as significant at a p-value equal to or less than (0.05).
RESULTS
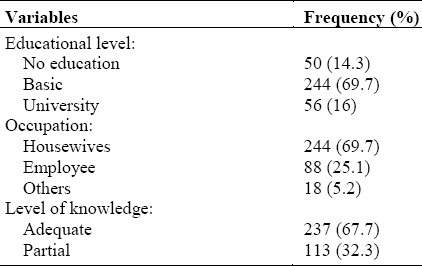
Three hundred and fifty housewives were interviewed with a compliance rate of 87.5%. Their educational level varied from none (14.3%) to that of a university graduate (16%) but the majority had basic education (69.7%). The majority of the respondents were housewives (69.7%) and about one quarter were employed.
A total of 237 (67.7%) mothers were found to have adequate knowledge about malaria and the rest either had inadequate knowledge (28.3%) or lacked the knowledge (4.0%) (Table 1). There was no significant difference between the level of knowledge and level of education (P>0.5) but mothers who were full-time housewives had better knowledge than those who were employed (P=0.00) - data not shown.
Table 1.
Education level, occupation and knowledge about malaria (n=350)
The caregiver's perceived causes of fever varied according to the intensity of the fever (Table 2). Malaria, was perceived as a cause by only 143 (40.9%) if the fever was mild and by 275 (78.6%) respondents if it was severe. This variation was also observed with the reported practices (Table 3) and preferred anti-malarial drugs for treatment (Table 4). Respondents who had any level of education preferred to consult health workers rather than consult other sources (p=0.00) - data not shown.
Table 2.
Caregivers’ perceived cause of low and high fever
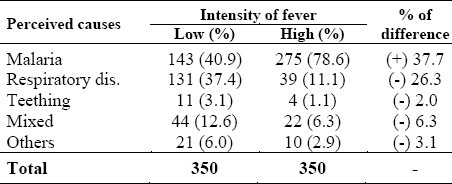
Table 3.
Selection from available treatment options (ATP) in relation to intensity of fever
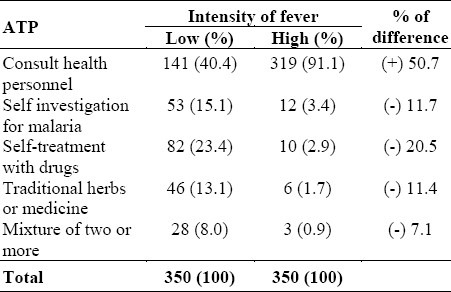
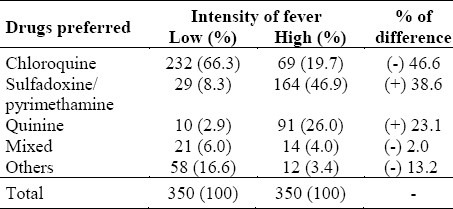
Table 4.
Preferred anti-malaria drugs for treatment of fever
DISCUSSION
Malaria was the commonest febrile illness in the study area. This may explain the high level of knowledge reflected by this study as >60% of the respondents had adequate knowledge, while the rest had partial knowledge about the symptoms of malaria. This is in accord with other observations where recognition and classification of clinical features by the caregiver was the key to intervention.10 In contrast to the findings of other investigations,15 the level of education of the caregivers had no significant relation with positive malaria- related knowledge. This may be explained by the fact that malaria is a known problem in the area. What is unique in this study is that being full-time housewives, was found to have a significant relation.
The local understanding of febrile illness and associated treatment was complex.16 Caregivers in the area classified fever according to its intensity (mild/severe). It seemed that the perceived causes, treatment practices and anti-malarial drugs preferred depended largely on that. In this study, malaria was considered a cause, treatment was sought from health personnel, and more potent, drugs such as quinine were used when the fever was classified as severe. Only 40.9% considered malaria the cause of mild fever while the majority of respondents (78.6%) shifted to malaria when the fever was severe. While 232 (66.3%) respondents would give chloroquine for mild fever, only 69 (19.7%) would not give chloroquine for severe fever even if they perceived malaria as a cause.
Treatment practices varied according to the evaluation of the symptoms and perceived treatment effects.16 The initial reaction of most caretakers, was to do something immediately after realizing that the child was sick, irrespective of the illness.16 In our study, this depended on the perceived intensity of fever. Only 141 (40.4%) of caregivers were likely to consult health personnel as their first option for mild fever. This is similar to what has been reported by other investigators.15,17 If the episode evolved into a more serious condition, the need for treatment services changed,9,18 as was found in our situation where 319 (91.1%) reported consulting the health personnel for severe fever. In Kenya, it was reported that patients were more likely to start with self-treatment at home and wait for some time to observe the progress of the illness.9 Self-treatment with drugs reported in this study was less than 25%. That was similar to what was reported in other urban areas of Sudan.19
In conclusion, housewives with children under 5 years had adequate knowledge about malaria. Their decision about selecting from available treatment options as a response to fever depended largely on the intensity of fever as did their choice of antimalarial drugs. This was likely to lead to a delay in the treatment of malaria and unfortunate consequences. Health education programmes should be directed at emphasizing the importance of seeking early treatment, taking drugs as prescribed and promptly, and raising mothers’ awareness of the danger signs.
ACKNOWLEDGEMENT
The authors would like to thank the respondents and the data collectors for their contribution to this study.
REFERENCES
- 1.Shaheen R, Rahman MS. Sociology of Health Care Decision: Exploration at a Public Hospital Dispensing Traditional Medicine in Bangladesh. World Health and population. 2001;4 (available at: http://www.longwoods.com/product.php?productid=17593&cat=389&page=1 . [Google Scholar]
- 2.MacKian S. A review of health seeking behaviour: problems and prospects. HSD/WP/05/03. available at www.hsd.lshtm.ac.uk/publications/hsd_working_papers/05-03_healthseeking_behaviour.pdf .
- 3.Shaikh BT, Hatcher J. Health seeking behaviour and health service utilization in Pakistan: challenging the policy makers. J Public Health. 2005;27:49–54. doi: 10.1093/pubmed/fdh207. [DOI] [PubMed] [Google Scholar]
- 4.WHO/UNICEF. World Malaria Report. 2005. www.rbm.who.int/wmr2005 .
- 5.Malik EM, Khalafalla OM. Malaria in Sudan: past, present and the future. Gazera J of Health Sciences. 2004;1(supp):47–53. [Google Scholar]
- 6.WHO. Roll Back Malaria Strategic Framework for Scaling up Effective Malaria Case Management. 2004. Mar, www.rbm.who.int/partnership/wg/wg_management/docs/framework.pdf .
- 7.Muller O, Traore C, Becher H, Kouyate B. Malaria morbidity, treatment-seeking behaviour, and mortality in a cohort of young children in rural Burkina Faso. Trop Med Int Health. 2003;8:290–296. doi: 10.1046/j.1365-3156.2003.01030.x. [DOI] [PubMed] [Google Scholar]
- 8.Comoro C, Nsimba SED, Warsame M, Tomson G. Local understanding, perception and reported practices of mothers/guardians ad health workers on childhood malaria in Tanzania district-implications for malaria control. Acta Tropica. 2003;87:305–13. doi: 10.1016/s0001-706x(03)00113-x. [DOI] [PubMed] [Google Scholar]
- 9.Nyamongo IK. Health care switching behaviour of malaria patients in a Kenyan rural community. Soc Sci Med. 2002;54:377–86. doi: 10.1016/s0277-9536(01)00036-3. [DOI] [PubMed] [Google Scholar]
- 10.Hill Z, Kendali C, Arthur P, Kirkwood B, Adjei E. Recognizing childhood illnesses and their traditional explanations: exploring options for care-seeking interventions in the context of the IMCI strategy in rural Ghana. Trop Med Int Health. 2003;8:668–76. doi: 10.1046/j.1365-3156.2003.01058.x. [DOI] [PubMed] [Google Scholar]
- 11.Espino F, Manderson L. Treatment seeking for malaria in Morong, Bataan, the Philippines. Soc Sci Med. 2000;50:1309–16. doi: 10.1016/s0277-9536(99)00379-2. [DOI] [PubMed] [Google Scholar]
- 12.Thera MA, D’Alessandro U, Thiero M, Ouedraogo A, Packou J, Souleymane OA, et al. Child malaria treatment practices among mothers in the districts of Yanfolila, Sikasso region, Mali. Trop Med Int Health. 2000;5:876–81. doi: 10.1046/j.1365-3156.2000.00652.x. [DOI] [PubMed] [Google Scholar]
- 13.Tarimo DS, Lwihula GK, Minjas JN, Bygbjerg IC. Mother's perceptions and knowledge on childhood malaria in the holoendemic Kibaha district, Tanzania: implications for malaria control and the IMCI strategy. Trop Med Int Health. 2000;5:179–84. doi: 10.1046/j.1365-3156.2000.00537.x. [DOI] [PubMed] [Google Scholar]
- 14.Al Gadal AA. Malaria in the Sudan.In Proceedings of the conference on malaria in Africa. In: Buck AA, editor. Washington DC: American Institute of Biological Sciences; 1986. pp. 156–159. [Google Scholar]
- 15.Njama D, Dorsey G, Guwatudde D, Kigonya K, Greenhouse B, Musisi S, et al. Urban malaria: primary caregivers, knowledge, attitudes, practices and predictors of malaria incidence in a cohort of Ugandian children. Trop Med Int Health. 2000;8:685–92. doi: 10.1046/j.1365-3156.2003.01060.x. [DOI] [PubMed] [Google Scholar]
- 16.Nsungwa-Sabiiti J, Kallander K, Nsabagasani X, Namusisi K, Pariyo G, Johansson A, Tomson G, Peterson S. Local fever illness classifications: implications for home management of malaria strategies. Trop Med Int Health. 2004;9:1191–9. doi: 10.1111/j.1365-3156.2004.01319.x. [DOI] [PubMed] [Google Scholar]
- 17.Nuwaha F. people's perception of malaria in mbarara, Uganda. Trop Med Int Health. 2002;7:462–70. doi: 10.1046/j.1365-3156.2002.00877.x. [DOI] [PubMed] [Google Scholar]
- 18.Konradsen F, Amerasinghe PH, Perera D, Van der Hoek W, Amerasinghe FP. A village treatment center for malaria: community response in Sri Lanka. Soc Sci Med Mar. 2000;50(6):879–89. doi: 10.1016/s0277-9536(99)00378-0. [DOI] [PubMed] [Google Scholar]
- 19.Abdel-Hameed AA. Malaria case management at the community level in Gezera, Sudan. Afr J Med Sci. 2001;30(Suppl):43–6. [PubMed] [Google Scholar]