

Abstract
Objective:
The aim of this study was to evaluate the availability of health materials and means on diabetes and hypertension at PHCCs in Aseer region, Saudi Arabia.
Materials and methods:
This study was carried out in PHCCs in Aseer region. A questionnaire was distributed to all PHCCs in the region. The questionnaire elicited information on the total population served, the number of diabetic and hypertensive patients, and the availability of health materials for diabetes and hypertension. Data were entered and analyzed by using SPSS.
Results:
A total of 242 PHCCs out of 245 responded to this questionnaire. There were 20 health educators (8%).Availability of health education materials ranged between 10 to 50%. Health education programs for Diabetes and hypertension were available in more than 90% of PHCCs.
Conclusion:
This study revealed that most of PHCCs in Aseer region lacked essential health education materials and means for diabetes and hypertension and, therefore were in urgent need of these materials from the Health Education Department, private health sectors and drug companies.
Keywords: Health education, availability, Diabetes, Hypertension, Aseer Region
INTRODUCTION
Health Education (HE) is one of the most important elements of primary health care and an essential function of Family Practice.1,2 It has many advantages for patients, physicians and resources, and plays a major role in strengthening patient-doctor relationship, improving the quality of primary health care, increasing patient compliance with medical advice and reducing financial costs of the health sevices.3,4 Health education particularly for those groups at high risk is considered the responsibility of the health teams at primary health care centers.5 Diabetes Mellitus (DM) and Hypertension(HTN) are two examples of chronic health problems whose prevalence has increased dramatically during the last decade among Saudis.6–8 Both diseases share common properties such as chronicity and the need for continuous medical care and health education.
In spite of the importance of auditing health education programs for DM and HTN, only one study has been carried out to assess diabetic health education program in one PHC in Aseer region. The findings of that study revealed that poor diabetic care outcomes could be due to the shortage of health education resources.9 In order to introduce good health education programs for DM and HTN patients, it is essential to know the extent of availability of essential health education resources at PHCCs.
The aim of this study is to assess the availability of health education resources for DM and HTN in primary health care centers in the Aseer region, in the southwest of Saudi Arabia.
METHODS
This study was conducted in September 2001. A multi-purpose questionnaire was used to assess different aspects of health care services in primary health care centers in Aseer region. One part of this questionnaire assessed the availability of resources for DM and HTN. This part enquired about the total population served, the number of registered diabetic and hypertensive patients, health education materials and means, namely: booklets, pamphlets, posters, videotapes and health education programs at each center. The availability of resources was assessed on a 2-point scale (1=available, 0=not available). Data of the questionnaire were entered and analyzed by using SPSS. Chi-square test was used to assess the association between the availability of each item and both diseases, and p-value was considered significant if it was less than 0.05.
RESULTS
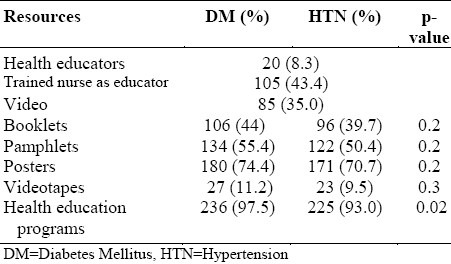
The total number of PHCCs which responded to the questionnaire was 242 out of 245, giving a response rate of 99%. These PHCCs served 970306 individuals. Diabetics and hypertensive patients constituted 26313 (2.7%) and 13087(1.4%) respectively. There were only 20 (8.3%) health educators and 105 (43.4%) well-trained nurses conducting health education. Table 1 shows the resource availability for DM and HTN at PHCC settings in the Aseer region. The most common available resources for both DM &HTN health education were posters followed by pamphlets. Videotapes for DM and HTN were available in 11.2%and 9.5% of PHCCs respectively. More than 90% of PHCC had health education programs on DM and HTN. A comparison of the degree of availability of health education materials for DM and HTN showed no big differences as most of PHCCs were short of most items except those health education programs on DM in 97.5% of PHCC compared to its availability in 93% for HTN (p=0.02).
Table 1.
Availability of health education resources on Diabetes and Hypertension in PHCC, Aseer Region, SaudiArabia, 2001 (N=242)
DISCUSSION
Successful management of chronic health problems such as DM and HTN depends on comprehensive continuous care with health education as its the back bone. Health education is not only essential in helping patients to adhere to medical advice on treatment but also important for prevention with periodic health examination and screening particularly for those health problems that are highly prevalent such as DM and HTN.5
Competent health educators in the Aseer region are few, which makes it difficult to cover all PHCCs. To overcome this shortage, Arabic speaking nurses who care for diabetics and hypertensive patients must be given a health education training course on DM and HTN.
In this study, we found that essential resources for conducting health education for diabetics and hypertensives were not adequate. Only education programs on the action plans were available in more than 90% of PHCCs. However, to make these programs efficient, other resources such as booklets, pamphlets and videotapes should be made available.
There should be a multi-system approach towards making these aids available; health friends committees, pharmacological companies and private medical sectors can make significant contribution towards this.
In primary care settings, the face to face method is still the usual method for conducting health education. However, with the increasing number of diabetic and hypertensive patients, this approach is difficult for PHC physicians who have so many other responsibilities. To reduce the time spent on face to face health education, it is essential to provide PHCCs with adequate booklets and pamphlets to be read and used as good references by educated patients while waiting to be seen. Although, the use of audiovisual aids is helpful in disseminating information on health education, they were scarce in PHCCs. Videotapes (VT) about DM and HTN were only present in 11% and 9.5% of PHCCs respectively while videos were available in 35% of PHCCs. All PHCCs should be provided with videotapes on DM and HTN as a matter of urgency particularly in those that do not have enough health educators and Arabic speaking doctors.
Generally, resources for health education on DM and HTN were inadequate. The following recommendations are therefore made:
Health Education Department in the General Directorate should have a budget for the production of health education materials on DM and HTN.
Donation by the Health Committees could be directed to the provision of health education resources according to need.
Pharmaceutical companies should be invited to assist in providing PHCCs with some health education resources such videotapes, booklets and pamphlets.
DM and HTN health education program should be audited periodically.
CONCLUSION
This study revealed that the essential resources for health education on DM and HTN were not adequate at PHCCs in Aseer region. The provision of PHCCs with health education resources is therefore, a matter of urgency.
REFERENCES
- 1.Al-Mazrou Y, Al-Shehri S, Rao M. Principles and Practice of Primary health care. 1st edition. Riyadh: Al-Helal Press; 1990. pp. 101–12. [Google Scholar]
- 2.Rakel RE. Essentials of Family Practice. 2nd edition. Philadelphia (USA): WB Saunders; 7. pp. 6–7. [Google Scholar]
- 3.Shires DB, Hennen BK, Rice DI. Family Medicine, A Guide Book for Practitioners of the Art. 2nd edition. NY (USA): Mcgraw-Hill Book company; 1987. [Google Scholar]
- 4.Sloane PD, Slatt LM, Curtis P. Essentials of Family Medicine. 2nd edition. Baltimore(USA): Williams & Wilkins; 1993. pp. 155–162. [Google Scholar]
- 5.The Scientific Committee of Quality assurance in Primary Health Care. Quality assurance in Primary Health Manual. :223–40. WHO –EM/PHC/81—A/G/93, (Arabic version) [Google Scholar]
- 6.Warsy AS, El-Hazmi MAF. Diabetes Mellitus, Hypertension and obesity. Common multi-factorial disorders in Saudis. East Mediterr Health J. 1999;5:1236–42. [PubMed] [Google Scholar]
- 7.Al-Nuaim A, Rubean K, Al-Mazrou Y, Khoja T, Al-Attas O, Al-Daghri N. National Chronic Metabolic Diseases Survey. Part 1. Riaydh (KSA): Ministry of Health and King Saud University; 1995. p. 31. [Google Scholar]
- 8.El-Hazmi M MAF, Warsy AS, Al-Swailem A, Al-Swailem AM. Prevalence of hypertension in adult Saudi population. Saudi Med J. 1998;19:117–22. [PubMed] [Google Scholar]
- 9.Al-Khaldi YM, Khan MY. Audit of a diabetic health education program at a large primary health care center in Asir region. Saudi Med J. 2000;21(9):838–42. [PubMed] [Google Scholar]