

Abstract
Background:
A medical record contains data on patients to support current and continuing patient care. Medical Records Department has the traditional role of keeping the patient's records safe. This is the first attempt in the Kingdom, to the best of our knowledge, to assess the feasibility of introducing electronic medical records.
Objective:
The aim of the study was to assess the views of physicians, patients and nurses of medical records services and physicians’ views on the use of electronic medical records.
Methods:
The study was conducted with physicians, nurses and patients selected randomly from the Military hospital in Riyadh. The data was collected via a self- administered, pilot-tested, internally consistent questionnaire.
Results:
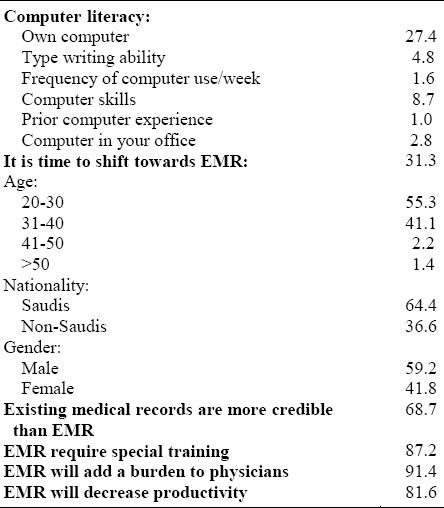
On the staff of medical records, the highest mean score was obtained for confidentiality (2.92), and the lowest for the training of medical staff (1.88). On medical record documents, the highest mean score was reported for “information is confidentially maintained” (2.70), and the lowest for the organization of files within file sections (2.28). On the Medical Records Department, the highest mean score was reported for overstaffing (2.89), and the lowest for receptiveness of receptionists (2.27). Physicians had low scores for computer literacy, ranging from 1% for prior computer experience to 27% for owning a computer. Physicians were not enthusiastic about the change to electronic medical records.
Conclusions:
Despite the observed shortcomings of the existing medical records system, it is not expected that medical records would be computerized in the near future since physicians have not accepted this technology wholeheartedly.
Keywords: Medical records, physicians, nurses
INTRODUCTION
Medical Records Department (MRD) has the traditional role of keeping patients’ records safe. This role consists of compiling, typing, storing, and retrieving medical information concerning patient care in health care organizations.1,2 The information is simply a documentation accumulated over time from various sources within the health care organization for the primary purpose of supporting current and continuing patient care.2,3 This traditional role has grown gradually as the healthcare industry becomes more complex, and critically dependent on accurate comprehensive data to support good clinical management, administrative affairs of the medical institution, teaching, research, utilization review, reimbursement, statutory requirements, and legal needs.4,5 The overwhelming amount of information in patient records and the increasing requests for documentation from the MRD, makes it increasingly difficult to manually keep up with demands in a timely manner.6–9
The handwritten record has been the standard way of documenting medical information in Saudi Arabia since the early 1970s. With the recognition of the importance of accurate patient information as one of the most important criteria for accreditation of hospitals for residency programs by the Arab Medical Board in the 1980s, the proper keeping of medical records has become even more crucial.10 The MRD has functions that are service oriented and vary according to the type of facility. These functions are usually judged in terms of accuracy, legibility, accessibility, completeness, timeliness, confidentiality, accountability and efficiency.11,12 The present paper is an assessment of the perception of physicians, nurses, and patients of medical records services, and physicians’ views on the use of electronic medical records (EMR) at the Military Hospital, Riyadh, Saudi Arabia.
METHODOLOGY
The study used a questionnaire comprising statements to which the respondents were asked to indicate agreement on a four-point scale from strongly agree (= 4) to strongly disagree (= 1). The questionnaire collected information from physicians, nurses and patients. The information concerning qualifications and training of the medical records staff was collected with the help of the Director of the MRD who is a staff member of the College of Applied Medical Sciences, Community Health section. The study was conducted at the Military hospital in Riyadh. The sample consisted of 150 physicians and 120 nurses selected randomly from the list of physicians and nurses available at the Administration Department. A sample of 120 patients was selected from the outpatients clinic. The sample selection criteria limited it to only individuals who were 20 years of age or older. Participation was voluntary and assurance of confidentiality was emphasized. As a pre-test, we administered the questionnaire by interview to 21 physicians and 23 nurses. Questions that were confusing, ambiguous, or gave very skewed responses were either removed, rewritten or replaced. The questionnaire was administered by trained final year students in the Department of Community Health Sciences, School of Applied Medical Sciences.
Analysis of variance using Kruskal–Wallis, and t-test using Mann-Whitney were used to compare the mean score levels between nurses, physicians and patients. Data were analyzed using SPSS computer package program.
RESULTS
Data were obtained from 105 physicians, 109 nurses and 120 patients; giving a response rate of 74%. The sample was composed of 73 males (70%) and 32 females (30%). The majority of physicians and nurses were 31-40 years old, 42% and 45% respectively. Regarding experience, the majority of physicians (60%) had more than 11 years of experience, while more than 80% of nurses had less than 10 years experience. More than 60% of the patients were males, aged 20- 39, had finished secondary school and 62% of the patients were married.
Table 1 shows the mean score of the views of physicians and nurses on the staff of medical records. There were no significant differences between physicians and nurses in their overall views on the medical record staff. The overall mean score was 2.52. The overall mean score for nurses (2.55) was higher than that of physicians (2.49). There was a significant difference between nurses and physicians on MRD (Table 2). For physicians, the overall mean score was 2.45, and for nurses it was 2.64. The difference was related to design and shape of the medical record and organization of files within the records. There was a significant difference between respondents on MRD (Table 3). For physicians, the overall mean response was 2.50, for nurses it was 2.60 and for patients it was 2.39. Low scores were reported for the location of MRD and receptiveness of receptionists. Table 4shows physicians′ opinion on electronic medical records (EMR). For computer literacy, 27.4% reported they owned a computer, 8.7% had computer skills, 4.8% had typing-writing ability and only 1.6% spend time on the computer. Overall, 31.3% of the physicians stated that it was time to move to EMR. More than 90% of the physicians admitted that EMR would add the burden of the entry of data and 81.6% reported that it would decrease productivity.
Table 1.
Mean score of physicians and nurses about the staff of medical records
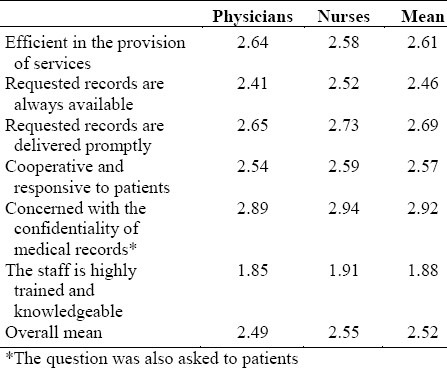
Table 2.
Mean score of physicians and nurses about Medical Records Department
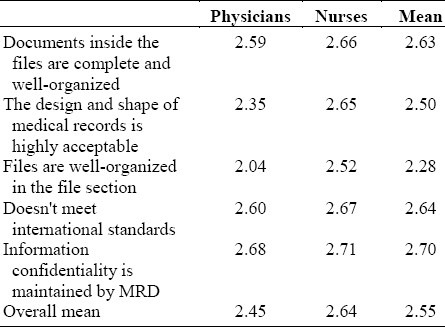
Table 3.
Mean score of physicians, nurses and patients about Medical Records Department
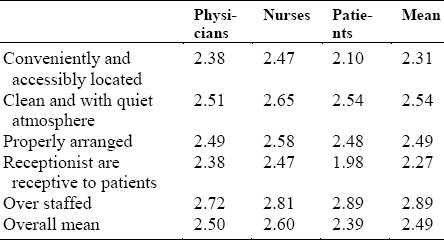
Table 4.
Physicians’ opinion on electronic medical records
DISCUSSION
Besides contributing to medical research, medical record benefits the patient, the health facility, the doctor, as well as the community. Poorly designed medical record acts more as a loosely woven historical archive than a clinically useful database. It can lead to poorly informed clinical practice, medication errors, inappropriate repeat investigations and unnecessary referrals and waste of clinical time and other resources.13–17 In this study, 65.5% of the respondents stated that the design and shape of medical record was not acceptable and did not meet international standards. Else et al18 stated that the design could be improved to make patients’ data easily accessible by highlighting certain data items in color or by other means. In Sweden, red-date stamps mark the beginning of each progress note and assists the doctor to skip encounter by encounter. In the USA, the nightshift annotates the record in red so the doctor can see at a glance if a patient had a troublesome night. Medical professionals have long considered confidentiality of patients’ medical information of paramount importance. Access to such information must be controlled because disclosure can be harmful to the patient.19–22 Twenty-seven percent of the respondents indicated that information from medical records is leaked in different ways and this leakage was not limited to the MRD. Najla22 reported a similar result (24%) in a previous study. Information can be leaked anywhere on the hospital premises, when the records are transferred to other departments.7,8,22,23 Andrew and Karine24 stated that medical information remains privileged even after a patient dies and this privilege can be only abrogated by spoken or written communication from the patient. The importance of physical facilities in the medical record department was emphasized by all the respondents. A considerable percentage of physician and nurses considered physical facilities appropriate. The low scores reported by patients especially for receptiveness of receptionists (1.98) might be explained by the fact that the majority of patients were young with high expectations. Many authors1,7,8,17 emphasized the importance of various characteristics and qualities expected of the MRS staff. They must have a pleasant personality and maintain a good personal appearance. However, these are qualities that can be acquired through training, continuous education and proper supervision. Most of the physicians complained about missing and lost files. The physical space of the MRD is very limited with more than 20,000 medical records. This raises the possibility of loss. With the amount of clinical activity and high rate of admissions, errors are likely to occur. To solve this low level of efficiency, the skills and knowledge of the staff should be developed through training, incentives and the adequate budgetary allocation.
Like other fields of human endeavour, MRD has taken a leap forward by entering the World Wide Web.25 Many studies have emphasized the importance of EMR.26–29 EMR has a lot to offer to the physicians. Not only do they have access to patients′ records with the press of a button but they also have easy access to information on drug interaction, care protocol and other information that they would have had to look up in the paper records. The reality is that this technology requires skill and training. The majority of physicians were unconvinced about the need for the EMRs. This may be explained by the lack of skills and computer knowledge of most physicians.30–32 Physicians are known to have an aversion for clerical work. More than 90% of physicians were worried that EMR would give them the burden of entering patient data. This would transfer to them some tasks that support staff do, such as retrieving and preparing the paper records. The majority of the physicians (72%) reported the EMR would decrease productivity and detract from patient-physician relationship. Doctors would see fewer patients because schedules would be expanded to give doctors more time for data entry, especially for those who lack computer knowledge and typing skills since going to various screens to review charts would take longer than reviewing paper records.32–34 Seth et al27 reported that desktop computers could become a physical barrier, making a clinician avoid eye-contact with patients. He found that patients were less satisfied with care when data were entered through a computer. Laerum et al32 reported a low level of EMR use in Norway despite its extensive availability. He found that more than 50% of the physicians were not satisfied and preferred the use of paper records, and that physicians used the system for less than half of the tasks for which it was meant.
In clinical practice, data had to be on the right patient at the right time and in the right place. Improving record design, training of the staff would enable faster services and searches and thereby improve the outcome for patients and reduce the cost of health care. Although efficient and usable software EMR do exists, their application is not feasible at the moment. Strategies for successful implementation of EMR should include engaging the physicians and practitioners in computer activities and providing strong support from the Ministry of Health before and during the redesign effort.
REFERENCES
- 1.Fung V. The development of medical records services in Hong Kong public hospitals. Health Inf Manag. 1994;24:151–2. doi: 10.1177/183335839402400413. [DOI] [PubMed] [Google Scholar]
- 2.Rustom AH. Medical records in the government hospitals, Gaza Strip. Palestine. 2000;41:19–23. [PubMed] [Google Scholar]
- 3.Margret A. Preparing the organization for the computer-based patient record. J Health Care Information Management. 1998;4:21–7. [PubMed] [Google Scholar]
- 4.Lowes R. EMR? Not exactly good enough? For now. Med Econ. 2002;79:32–4. [PubMed] [Google Scholar]
- 5.Ching CY. Medical records development in Malaysia. IHRIM. 1995;12:3–5. [PubMed] [Google Scholar]
- 6.Ken T. Electronic medical records make sense at last. Medical Economics. 2001;10:134–43. [PubMed] [Google Scholar]
- 7.Al-Hayan S. Evaluation of medical record contents in Kuwait government general hospitals. MSc thesis; University of Alexendria; 1989. [Google Scholar]
- 8.Ajluni M. Evaluation of medical record services in some general hospitals in Jordan. Ph.D thesis; University of Alexendria; 1993. [Google Scholar]
- 9.Hagland M. Moving gradually towards a paperless world. J AHIMA. 2000;8:33–4. [PubMed] [Google Scholar]
- 10.Survey manual for accreditation of hospital for teaching purposes. Amman: Arab Medical Board; 1983. Arab Medical Board. [Google Scholar]
- 11.Merz B. General practice computerization: lessons from United Kingdom. Med J Aust. 2000;172:22–4. doi: 10.5694/j.1326-5377.2000.tb123873.x. [DOI] [PubMed] [Google Scholar]
- 12.Guler I, Muldur S. A model approach to sharing electronic medical records between and within state hospitals in turkey. Comp Biol Med. 2001;31:513–23. doi: 10.1016/s0010-4825(01)00018-x. [DOI] [PubMed] [Google Scholar]
- 13.Meyers JS. Electronic medical records: 10 questions I do not know to ask. Fam Pract Manag. 2000;8:29–32. [PubMed] [Google Scholar]
- 14.Bobis KG, Camoriano J. Managing technology in a physician-led organization. J Health Inf Manag. 2003;17:24–31. [PubMed] [Google Scholar]
- 15.Patricia W, Carel J, Jeremy W. How to limit clinical errors in interpretation of data. Lancet. 1998;352:1539–43. doi: 10.1016/S0140-6736(98)08308-1. [DOI] [PubMed] [Google Scholar]
- 16.Jeremy CW, Patricia W. Design should help use of patients’ data. Lancet. 1998;352:1375–8. doi: 10.1016/S0140-6736(97)08306-2. [DOI] [PubMed] [Google Scholar]
- 17.Shehata AI, Hashim TJ. Study of medical and nursing staff attitude and satisfaction with hospital medical record services. Journal of the Medical Research Institute. 1997;18:50–60. [Google Scholar]
- 18.Else N, Jeremy CW, Patricia W. Helping clinicians to find and avoid delays. Lancet. 1998;352:1462–6. doi: 10.1016/S0140-6736(97)08307-4. [DOI] [PubMed] [Google Scholar]
- 19.Ohliger PC. Are your medical records confidential. AIDS Read. 1999;9:282–3. [PubMed] [Google Scholar]
- 20.Pyper C, Amery J, Waston M, Crook C, Thomas B. Patients access to their online electronic health records. J Telemed Telecare. 2002;2:103–5. doi: 10.1177/1357633X020080S247. [DOI] [PubMed] [Google Scholar]
- 21.Kenneth DM, Peter S, Issac SK, David M, Rhona MD. Public standard and patients’ control: how to keep electronic medical records accessible but private. BMJ. 2001;322:283–94. doi: 10.1136/bmj.322.7281.283. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Najla Al-Sheifi. King Saud University; 2001. Attitiude of physicians and nurses towards medical records. Graduation project, Department of Community Health, College of Applied Medical Sciences. [Google Scholar]
- 23.Mogli GD. Oman towards electronic medical records. IHRIM. 2001;42:22–4. [PubMed] [Google Scholar]
- 24.Andrew HM, Karine M. Confidentiality of health information postmortem. Arch Pathol Lab Med. 2001;125:1189–92. doi: 10.5858/2001-125-1189-COHIP. [DOI] [PubMed] [Google Scholar]
- 25.Kohane IS, Greenspun P, Fackler J, Cimino C, Azolovits P. Building national electronic medical record systems via the WWW. J Am Med Information Association. 1996;3:191–207. doi: 10.1136/jamia.1996.96310633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Reider J. Technology in your practice: the electronic medical records: promises and pitfalls. Med Gen Med. 2003;5:32–4. [PubMed] [Google Scholar]
- 27.Seth MP, Jeremy CW, Patricia W. Medical records: opportunities for and challenges of computerization. Lancet. 1998;352:161–72. [Google Scholar]
- 28.Ameth EA, Shehu BB. Medical record keeping and information retrieval in developing countries: surgeons′ perspective. Trop Doct. 2002;32:232–4. doi: 10.1177/004947550203200418. [DOI] [PubMed] [Google Scholar]
- 29.Hajra A. Lessons learned from electronic medical records implementation. NAHAM Manag J. 1998;24:3–7. [PubMed] [Google Scholar]
- 30.Hunt DL, Haynes RB, Hanna SE, Smith K. Effects of computer-based clinical decision support systems on physician performance and patient outcomes. JAMA. 1998;280:1339–46. doi: 10.1001/jama.280.15.1339. [DOI] [PubMed] [Google Scholar]
- 31.Szynal D. Doctors become palm readers. Health Data Manag. 2001;20:23–5. [PubMed] [Google Scholar]
- 32.Laerum H, Ellingsen G, Faxvaag A. Doctors’ use of electronic medical records systems in hospitals: cross sectional survey. BMJ. 323:1344–8. doi: 10.1136/bmj.323.7325.1344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Mandl KD, Kohane IS, Brandt AM. Electronic patient-physician communication: problems and promise. Ann Intern Med. 1998;129:495–500. doi: 10.7326/0003-4819-129-6-199809150-00012. [DOI] [PubMed] [Google Scholar]
- 34.Jim S. The medical records professionals′ view of the electronic medical record. J Ambulatory Care Manage. 2000;23:18–26. doi: 10.1097/00004479-200004000-00004. [DOI] [PubMed] [Google Scholar]