

Abstract
Aim:
This study aimed to determine the level of infant and under-five mortality rates and to examine the effect of socioeconomic, demographic and environmental factors on the health status of the children under five years.
Methods:
The data for this study were collected by means of a questionnaire addressed to women in Wad-Medani, Sudan. Three hundred women in the reproductive age (15-49) years were chosen randomly for this study. The data were analyzed statistically using the Statistical Package for Social Sciences (SPSS). Frequency distributions and a statistical test based on Chi-square for independence was conducted.
Results:
Infant mortality rate was 77 per 100 and child mortality rate was 67 per 100. The results revealed that immunization, child order, child birth weight, birth interval and contraceptive use had a significant influence on the mortality of children under the age of five. The mother's level of education is highly significant on the mortality of children under five years old.
Conclusions:
The Ministry of Health should give greater attention to improving immunization services and concentrate on health education campaigns for mothers and for the community.
Keywords: Determinants, Infant, Underfive mortality, Sudan
INTRODUCTION
Infant and child mortality rates are regarded as indicators of the prevailing health conditions in a society; they measure the success of health programmes and policies aimed at their education.
The World Summit for Children, held in 1990, instituted a package of objectives for implementation by the year 2000. Among these objectives was the aim to reduce infant and under-five mortality by one third or to 50 and 70 deaths per 1000 births, respectively, whichever was less.1 This was reaffirmed at the 1994 International Conference on Population and Development (ICPD).2 The 1992 population policy of Sudan announced the intention to reduce the mortality rates of children under five years of age to 60 deaths per 1000, from the level in 1992 by the year 2002.3
Sudan is a developing country characterized by high levels of infant and child mortality. According to the 1993 fourth national population census, under-five mortality rate was 150 per 1000 live births and one out of ten infants died before reaching their first birth day. The Safe Mother Survey (SMS) which was conducted in 1999 showed that under-five mortality rate was 105 per 1000 live births and infant mortality rate was 69 per 1000 live births.4
The persistence of high infant and child mortality rates, call for the identification of the main causes of this phenomenon. Moreover, there is a dearth of community studies on infant and child mortality.
The main objectives of this study were to determine the level of infant and child mortality rates in Wad-Medani and to identify the main causes.
METHODS
Study area and Population
Wad-Medani is the capital of the Gezira State. It is the second largest town in Sudan and lies on the bank of the Blue Nile. According to the fourth national census, Wad-Medani has a population of 430,487 comprising 214,670 males and 215,817 females.5 Its population is a mixture of different tribal groups of Sudan, most of whom are government employees, traders, farmers, and casual laborers. The average health situation in Wad-Medani town is better than the national average and also better than any of the other towns in Sudan.6
The data of this study came from a household survey conducted in September 2004. A simple random sampling technique was used with anticipated population proportion estimated to yield 300 women who had at least one child under five years of age. A sample of 504 children under-five in 300 household were investigated using a questionnaire. This questionnaire consisted of two sets of data; the first set asked for the child's sex, birth weight, birth order, birth interval, immunization and child mortality, while the second set dealt with the mother's socio-economic status and other environmental variables.
After the data were collected and coded, the Statistical Packet for Social Sciences (SPSS) were used to analyze the data. General tabulations including frequency distribution were used. Also chi-square test was used to evaluate some associations between the dependent variable infant and child mortality and a set of independent variables.
RESULTS
Demographic and Bio-medical Characteristics of the Children
Table 1 shows that 20.6% of the children were below the age of one and 79.6% of them were between 1 and 5 years. The sex percentages of infants and children under five was 43.7% males and 56.3% females. The birth weight of the children was classified into three groups: under weight, normal weight and unknown weight. Those underweight were 26.2%, children with normal birth weight accounted for 62.7% and unknown birth weight were 11.1%.
Table 1.
Demographic and Biomedical Characteristics of the Children
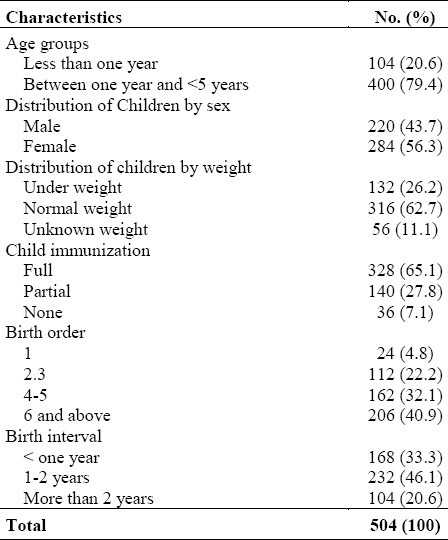
On the immunization status of the children, 65.1% of the children had been fully vaccinated, 27.8% partially immunized, while only 7.1% had no immunizations. The distribution of children by birth order is shown in Table 1. As can be seen from the table, 40.9% of the children were in the group ( six and more) births, 32.1% in the group (four to five) births, 22.2% in the group (two- three) births and only 4.8% in the first group (first child). For 33.3% of the children, the birth interval was less than one year, for 46.1% it was 1-2 years and it was more than two years for 20.6%.
Mother's Educational, Occupational and Marital Status
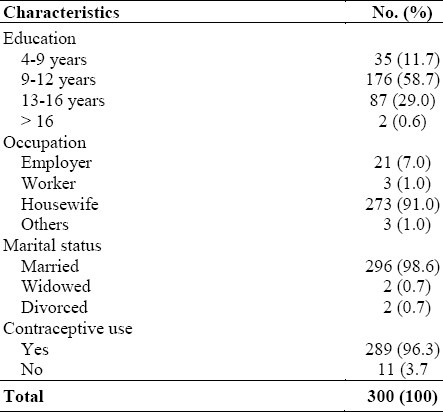
Table 2 shows mother's education, occupation and marital status. The percentage of women with 4-8 years of education was 11.7%, 9-12 years was 58.7%, 13-16 years was 29% and 0.6 formed the last category with more than 16 years of education. The same table shows that 91% of the women were housewives, 7% were employed,1% had other occupations. It was found that 98.6% were married, 0.7% were widowed and 0.7% were divorced. Of the mothers, 96.3% used contraceptive measures, while 3.7% did not.
Table 2.
Mother's educational, occupational and marital status
Family Income and some Selected Community and Environmental Variables
Table 3 shows the distribution of the sample households by the level of expenditure. It is obvious from the table that the majority of families (60.7%) belonged to the middle income group, whereas the low and high income groups formed 30.0% and 9.3% respectively.
Table 3.
Family income and some selected community and environmental variables
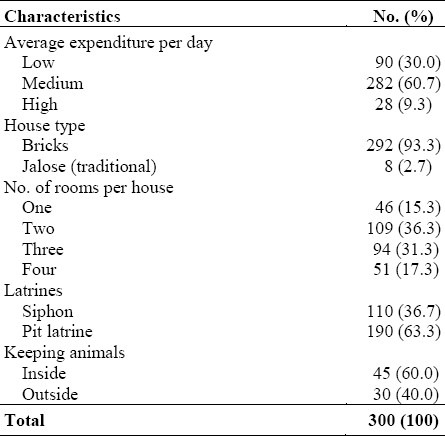
Housing conditions and sanitation are known to be important determinants of the level of infant and child mortality. Table 3 shows the types of houses, and number of the rooms and latrines. Ninety-seven point 3 percent of the women reported that their houses were made of bricks, 36.3% reported their houses had two rooms, 31.3% three rooms, and 17.1% had four rooms while 15.3% had one room only. When asked about latrines, 63.3% of the same women said they had pit-latrines, while only 36.7% had siphon. Seventy-five families kept animals, 60% of whom said the animals were kept inside the house, while 40% kept them outside.
Infant and Under-Five Mortality
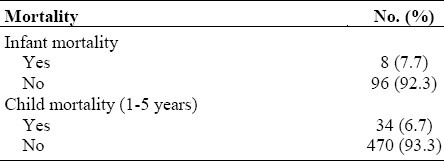
Table 4 shows child deaths. It was found that 7.7% of the women's infants had died, while 92.3% of them are alive. This meant that infant mortality rate was 77 deaths per 1000 live births. For the age group 1-5 years, 6.7% of the children had died, while 93.3% of them were alive, yielding Child Mortality Rate for that age group as 67 per 1000 live births.
Table 4.
Infant and child mortality
Associations Between the Mortality of Infants and Children Under five and Some Selected Variables
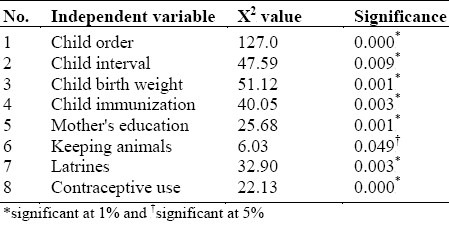
In this part, cross-tabulation for the most important variables relating to infant and under-five mortality are presented. In each case, a test of independence was performed using χ2 (Chi -square) test of independence. The independent variables that were assumed to affect the mortality of infants and children under five significantly (dependent variable) were child order, child interval, child weight, child immunization, mothers’ education, family income, keeping of animals, latrines and the use of contraceptives.
Table 5 shows that child order, child weight, interval between children, child immunization, the use of contraceptives, family income, mother's education and latrines were all significant at 1%, while only the keeping of animals was significant at 5%. This means that all these variables were strongly associated with the mortality of children under five years old and increased the risk of infant and child mortality.
Table 5.
Association between children under-five mortality and some selected variables
DISCUSSION
Since the 1970s, the estimated annual number of deaths among children of less than 5 years has decreased by almost a third. This reduction has been very uneven and in some countries the rates of childhood mortality are increasing. In 1998, more than 50 countries including Sudan still had childhood mortality rates of over 100 per 1000 live births.7
According to Rutstein (1984), Infant Mortality Rate (IMR) is the number of infants dying in the first year of life per 1000 live birth, whereas child mortality rate (1-5) is the probability of dying between the first and fifth birthday expressed per 1000.8
The analysis of infant and child mortality in Wad-Medani reveals that infant mortality rate is 77 per 1000 live births. This figure is consistent with the findings of the 1999 Safe Mother Survey (SMS),7 in which the national level of infant mortality was estimated at 68 deaths per 1000 live births. Also the study estimated under-five mortality as 67 deaths per 1000 live births. The Multiple Indicators Cluster Survey (MICS) which was conducted in the Gezira State in 2002, showed an analogous level in which 59 out of 1000 children died before reaching the age of five.9
On examination of the determinants of infant and child mortality, the study found a strong association with child order. As parity increases, the risk of infant and child mortality increase. Many studies suggest that infant and child mortality increase with the increase of parity after the second birth. The higher the parity, the shorter the birth interval, and the shorter the birth interval the higher risk of dying for a child. The risk of dying is considerably higher for a child who has a sibling born within the preceding two years.10,11 On the other hand, other studies suggest that infant and child mortality is generally higher for first born children, especially during the first year of life.12
The study showed that there is a significant association between birth interval and infant and under-five mortality. The length of the birth interval is a very important factor for the survival status of infants and children. If the length of the birth interval is short, the probability of dying is high. The probability of dying before age five for children born less than two years after a previous birth is more than double that for children born four or more years after a previous birth.13 Moreover, short birth intervals have indirect effects through such factors as mother's depletion, premature birth and limited family resources.11
The birth weight of the child has been found to be statistically significant as a determinant of under-five mortality. In line with results found elsewhere, mortality decreased with the child's increase in weight at birth. The rates of mortality for children who were under weight at birth were higher than those who had normal weight at birth.14
Further, the study showed a significant association between mother's education and infant and under-five mortality. Maternal education has been identified as one of the most important socioeconomic determinants of infant and child mortality. Many studies show that the higher the level of maternal education, the lower the infant and child mortality.15 Caldwell (1981) provided three explanations for the phenomenon: better educated mothers become less fatalistic about their children's illnesses. They are more capable of manipulating available health facilities and personnel and they greatly change the traditional balance of familial relationships with a profound effect on child care. In addition to these, they are more likely to have had antenatal care, to have given birth with some medical attention, and to have taken their children at some point to see a physician.16.
Regarding the significant association between the use of contraception and child mortality, we found that 73% of the women had not used any contraceptive methods within the last twelve months because of lack or unavailability in many of the areas covered by the study.
Immunization was an important factor affecting under-five mortality. The study showed a significant association between immunization and child mortality. However, not all the children had been vaccinated (full immunization 65.1%), because of the fear of complications from immunization.
Lack of latrines leads to high environmental contamination in houses and makes children more vulnerable to infectious diseases. Poor toilet facilities tend to increase infant and child mortality. For example, in an inter-American study, the incidence of diarrheal disease was lowest in households with pipe-borne drinking water and flush toilet facilities. Current access to proper toilet facilities was found to influence infant mortality, especially beyond the post-neonatal stage.12 Considering the association between the keeping of animals and child mortality, it was found that most households kept animals inside their houses, which increased the hazards of infectious diseases.
CONCLUSION AND RECOMMENDATIONS
The conclusion of this study is that infant and under-five mortality in Gezira State was still high and socioeconomic and environmental factors had a lot of influence on the health status of children in Wad Medani.
Finally, this study recommends the expansion of immunization of children, and education for mothers in order to promote family planning and improve child health. Also further detailed research is needed to provide better explanations for the determinants of the higher rates of infant and child mortality in Sudan.
REFERENCES
- 1.Dashtseren Ariunaa. Determinants of Infant and child Mortality in Mangolia. Bangkong, Thailand: IUSSP Regional Conference; 2002. Jun 9-13, [Google Scholar]
- 2.Programme of Action of the 1994 International Cosnference on Population and Development. New York: United Nation Publication; 1999. United Nation. [Google Scholar]
- 3.Population Policy of Sudan. Sudan: Population Council Khartoum; 1996. Government of Sudan. [Google Scholar]
- 4.Safe Motherhood Survey (1999) Khartoum: National Report; 2001. Central Bureau of Statistics. [Google Scholar]
- 5.The Fourth Population Census, 1993. Khartoum: Principal Report; 1995. Central Bureau of Statistics. [Google Scholar]
- 6.Sudan in Figures. Khartoum: Ministry of Finance and Economy; 2000. Central Bureau of Statistics. [Google Scholar]
- 7.World health report 1999: Making diffrence. Geneva: WHO; 1999. World Health Organization. [Google Scholar]
- 8.Rustein, Shea O. World Fertility Survey comparative studies, No. 43. Voorburg, Netherlands: International Statistical Institute; 1984. Infant and Child Mortality: Levels, trends and demographic differentials. [Google Scholar]
- 9.Multiple Indicators Cluster Survey (MICS) Medani, Khartoum: Ministry of Finance and Economy; 2002. Central Bureau of Statistics. [Google Scholar]
- 10.Hobcraft JN, McDonald JW, Rutstein SO. Socioeconomic factors in infant and child mortality: A cross-national comparison. London: World Fertility Survey; 1982. [PubMed] [Google Scholar]
- 11.Hobcraft JN, McDonald JW, Rutstein SO. Demographic determinants of infant and early child mortality: Comparative analysis. Population studies. 1985;39:363–85. [Google Scholar]
- 12.Hobcraft JN, McDonald JW, Rutstein SO. Child spacing effects on infant and child mortality. Population Index. 1983;49:585–618. [Google Scholar]
- 13.National Office of Statistics and UNFPA (1999) The Reproductive Health Survey of Mongolia. 1998 [Google Scholar]
- 14.Mosley WH, Chen LC. An analytical frame-work for the study of child survival in developing countries. Population and Development Review. 1984;(10 Suppl):25–45. [Google Scholar]
- 15.Caldwell JC. Maternal education as a factor in child mortality’. World Health Forum. 1981;2:75–8. [Google Scholar]
- 16.Murray CJL, Lopez AD. The global burden of disease a comprehensive assessment of mortality and disability from diseases, injuries and risk factors 1990; project to 2020. Geneva: WHO; 1996. [Google Scholar]