

Abstract
Objective:
To describe a community-based diabetes and hypertension screening campaign, the percentage of screened positive individuals, identified the participation rate, and the factors affecting the participation.
Campaign design and methods:
A community-based screening campaign whose main objective was the screening for diabetes and hypertension was conducted in the Eastern Province of Saudi Arabia for three and half months in the year 2004. A structured questionnaire was used. Diabetes mellitus was diagnosed on the basis of repeated detection of a fasting blood sugar equal to or more than 126 mg/dl, and hypertension when the blood pressure was 140/90 mm Hg or more.
Results:
Of the 650,000 target population, 214,381 (33%) participated, and 197,681 questionnaire were completed. Of the number of individuals screened, 31,711 (16%) were positive for abnormal blood pressure and /or glucose, and needed confirmation of their results. Only 17296 (54.5%) of them were referred to health facilities for confirmation of results
Conclusion:
Community screening campaigns for diabetes mellitus and hypertension is extremely efficient in identifying undiagnosed diabetic and hypertensive individuals. The most successful strategy for the screening and confirmation of results was through PHCCs, especially in the rural areas, where there was good organization and strict adherence to guidelines on methodology.
Keywords: Campaign, screening, Saudi Arabia, diabetes, hypertension.
INTRODUCTION
Diabetes mellitus (DM) and hypertension are among the most common chronic non-communicable diseases affecting both developed and developing countries. They are the main preventable risk factors for coronary heart disease, stroke, end-stage renal failure, disability and increased health-care costs.1–5 Screening for diabetes mellitus is controversial and has been researched extensively in the medical literature. The recommendation for it varied from promoting it to discouraging it except under certain circumstances. 1,6–8 However, the U.S. Preventive Services Task Force (USPSTF) strongly recommends that clinicians screen adults aged 18 and older for high blood pressure.9
There have been major developments in the Kingdom of Saudi Arabia in the last three decades, to which may be attributed the improvement in the financial status of the population. This has led to changes in major aspects of life generally. There have been environmental, physical, and dietary changes, which in turn have contributed to the decline of infectious diseases, but have resulted in an increase in the rates of chronic illness. Many studies done to estimate the prevalence of diabetes mellitus and hypertension in Saudi Arabia,10–15 have yielded results that vary widely. The reason may be the effect of the different methodologies used, such as the use of different cut-off points and age groups. However, in general, they show a significant increase in the prevalence of diabetes mellitus. According to the WHO, there were 890,000 diabetic patients in Saudi Arabia in 2000. It is estimated that the number will reach 2,523,000 by 2030. The global estimate by the WHO of the number of diabetic patients was 171 million in 2000 which was 2.8% of the total world population. This is expected to rise to more than 350 million by 2030.4 Therefore, health authorities in the Eastern Province of the Kingdom have recognized the seriousness of the problems associated with these chronic diseases which remain asymptomatic for a long time, and are convinced that diabetes mellitus and hypertension are important health problems. It has also been documented that quite a large percentage of these patients are not detected and remain for a long time without significant symptoms to warrant the quest for medical advice.16–20 Besides, the diseases are easy to detect; the test is feasible, with relatively high specificity and sensitivity. DM can be treated and the evidence for the effectiveness of treatment on early detection is promising. 21–25 In addition, primary prevention through the adoption of a healthy lifestyle or glucose lowering drugs have been established.26–30 It is also cost effective at the primary prevention level.31 Therefore, a public campaign was conducted to screen the Saudi population in the Eastern Province aged 30 years or more for diabetic and hypertensive individuals. It was hoped that the successes and failures as well as the lessons learnt from this campaign would encourage the design of a campaign that would cover the entire Kingdom. In addition, it is important to improve public awareness of the seriousness of these diseases and provide health education and other risk factors about them. The age thirty years and over was determined through a focus group in view of the consistent evidence indicating that diabetes mellitus was no longer a disease of old people.32,33
The aim of this paper is to describe the methodology used in the screening campaign, the percentage of screened individuals who were positive, identify the participation rate, as well as factors affecting participation.
MATERIALS AND METHODS
The Eastern Province is considered one of the largest provinces in Saudi Arabia and is located on the Arabian Gulf. It consists of fifteen sectors (Dammam, Khobar, Qatif, Ras Tanura, Abqaiq, Safwa, Jubail, Khafji, Oraiera, Nuaeria, Sarar, Qaria olaya, Rafia, Hassa, and Hafr Al-Baten). It is a mix of different cultures, backgrounds and is also geographically varied. A central committee that was established and led by the Director of General Directorate of Health Affairs, Eastern Province designed the details for the conduct of this campaign. A scientific committee led by the general director's assistant in primary health care centers (PHCCs), determined the risk groups of the population, and designed the detailed process for the running of this campaign. This included the establishment of the standards for the campaign, accreditations of instruments and health education materials to be used, training, financing, supervising, health education committees, and data processing committees.
Thirty-four trainers selected from the health sectors in the Eastern Province, were physicians or nurses with bachelors degree, and who had had previous experience in training, and had attended a scheduled course for conducting the campaign (accredited by Saudi Commission for Health Specialties by four hours of CME). They in turn trained the team members in their respective sectors for data collection. Mobile team supervisors in each sector, were responsible for quality control. PHCC physicians attended a one-day course for management of hypertension and diabetes mellitus, and were provided with written guidelines.
The campaign was conducted through examination posts run by nurses and technicians who were distributed to more than 190 primary health centers in the Eastern province, 40 hospitals (governmental and private), 30 dispensaries and polyclinics, 16 shopping malls and recreation centers in Eastern Province. In addition, 23 mobile teams visited the target population in places of work that had more than 30 employees aged 30 years or more. Each team included two local staff members, a nurse, and a health technician or clerk.
The job of one coordinator chosen from each sector was to supervise the examination posts, ensure the continuity of work and resolve issues such as the absence of health workers, equipment breakdown, shortage of forms, collection of forms, ensure that all forms were completed, remind defaulters, pursue campaign letters and cooperate with coordinators in other sectors and main supervision committees.
A media campaign was organized in each sector using the written material and audiovisual media. Besides, posters were put up on billboards along the streets and public places in the Eastern Province. The forms were collected from each sector and sent to the (PHCCs’) administration center, where they were double-checked for completeness. Non-eligible people were excluded, and the forms which were incomplete, or had un-confirmed results were sent back to the sectors with a covering letter for corrections to be made.
Male and female residents who were 30 years and above were invited to participate in the community-based screening for diabetes and hypertension, which was conducted between August 2004 and February 2005 (interrupted by Ramadan and feast holiday). The target population was estimated as 650,000 Saudis (pregnant women excluded) resident in the Eastern Province for more than six months.
A structured questionnaire developed through a focused group, and validated by experts in the fields of diabetes mellitus and hypertension, containing demographic data, medical history, social details including occupation, monthly income, educational level, physical activity and smoking status were completed during personal interviews. Weight and height were measured using standardized balance beam; height was measured to the nearest centimeter. The body mass index (BMI) was calculated as weight in kilograms divided by height in square meter.
Blood pressure was measured twice, one to two minutes apart. It was measured in the sitting position at rest. The average of the two readings was taken. If the second value was more than 5 mmHg different from the first, measurements were taken until a stable reading was attained. Blood pressure measurement was taken using standardized mercury sphygmomanometers with an appropriate cuff inflated to a pressure approximately 30 mmHg greater than systolic, and the patient's arm at the level of the heart. The systolic blood pressure was taken as that corresponding to the Korotkoff phase I, and the diastolic blood pressure was taken as that corresponding to the Korotkoff phase V.
Hypertension was defined as any one or combination of systolic blood pressure ≥ 140 mmHg, and diastolic blood pressure ≥ 90mmHg2 or previous diagnoses of hypertension on antihypertensive agents, regardless of the results.
If the systolic BP was ≥ 140mmHg or diastolic BP ≥ 90 or both in an undiagnosed subject, a confirmatory measurement was done in the nearest PHCCs on another day. Pre-hypertension was defined as systolic blood pressure 120-139mmHg, and/ or diastolic blood pressure 80-89 mmHg.
Blood glucose concentration was measured with a glucometer, utilizing glucose oxidase method. If the participant had been fasting for ≥8 hours and blood sugar was <100mg/dl after fasting for at least 8 hours, or random blood sugar was <140 mg/dl, he/she was considered non diabetic, and nothing was offered apart from health education brochures, especially if they had other risk factors. If the fasting blood sugar was ≥100mg/dl, or random capillary blood sugar was ≥140 mg/dl, the participant was sent to the nearest health facility with his / her request stamped with the campaign sticker supplied by his/her serial number, for confirmatory venous fasting blood sugar with instructions to fast for at least 8 hours before the test. Diagnosis of diabetes is based on the World Health Organization and American Diabetic Association criteria.34,3 A FBS of 100-125 mg/dl, is considered as impaired fasting glucose (IFG), while FBS≥ 126 mg/dl is considered diabetic, and referred to the health services, with a referral for management and further investigation. If the participant was previously diagnosed as diabetic on diet or blood sugar lowering agents, he/she was considered as diabetic regardless of the results, and no confirmatory test was required.
A pilot study was carried out in one of the PHCCs centers in Dammam, to check the accuracy of methodology, the time needed to screen each individual in the population, and the possible difficulties that would be encountered during the campaign.
Data was entered and processed using SPSS version 15. For this paper, a frequency distribution table was constructed. Chi-squared test was used for the comparison of appropriate variables. A p-value of <0.05 was considered indicative of statistical significance throughout the study.
The participants were assured of confidentiality of information collected, and newly diagnosed hypertensive and diabetic participants were informed that follow-up would be given free in the PHCCs or governmental hospitals. The gender of the participants was taken into consideration in completing the forms and in the clinical assessment
RESULTS
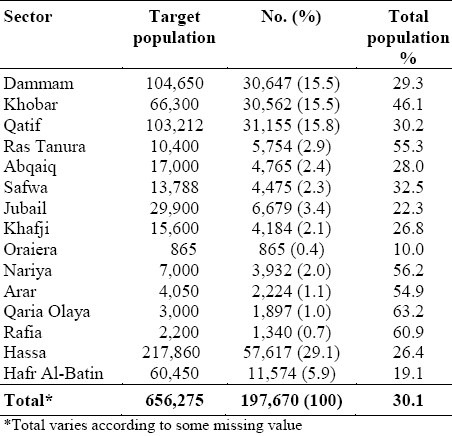
The total number of individuals screened, was 214,381, constituting 33% of the target population. The total number of forms sent to the PHCC administration was 198,489, and the remaining forms were considered as dropout (this could be the results of over-reporting from the sectors, or considered lost in transit). Up to 808 (0.4%) forms were excluded because they belonged to people from outside the Eastern Province, under 30 years of age, non-Saudis or pregnant women. Duplicate completed forms or forms with no results for blood sugar or blood pressure were also excluded. A total of 197,681 forms constituting 30.4% of the target population were entered into the computer from the various sectors (Table 1)
Table 1.
Distribution of screened population by sectors
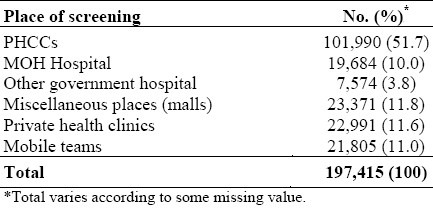
Most of the screening events 101,990 (51.7%) were conducted through PHCCs. Smaller numbers were screened in MOH hospital 19,684 ) 10%), 7574 (3.8%) in other government hospitals, 11991 (11.6%) in private hospitals and dispensaries, 23,371 (11.8%) at other public venues, and 21,805 (11%) seen by mobile teams, and for 266 individuals the venue was not indicated (Table 2).
Table 2.
Distribution of screened population according to place of examination
Of the participants screened 31,711 (16%) were positive for blood pressure and/or glucose, and needed confirmation of the results. However, only 17,296(54.5%) were referred to a health facility for confirmation of results. Mos t of them were referred to PHCCs-15,024 (91.4(%, 626 (3.8%) to MOH hospitals, 302 (1.8%) to private, and 485 (3%) to other government hospitals p<0.0005, and the place of referral for 859 was missing.
The total number of individuals whose results were not confirmed was 14,415 (45.4%). The most frequent cause was non-referral by the local health team 9,214 (63.9%). Other causes were: loss of contact 3107 (21.6%) refusal of referral 753 (5.2%), 1,373 (9.3%) did not respond to the invitation and on four the causes were not indicated (Figure 1).
Figure 1.
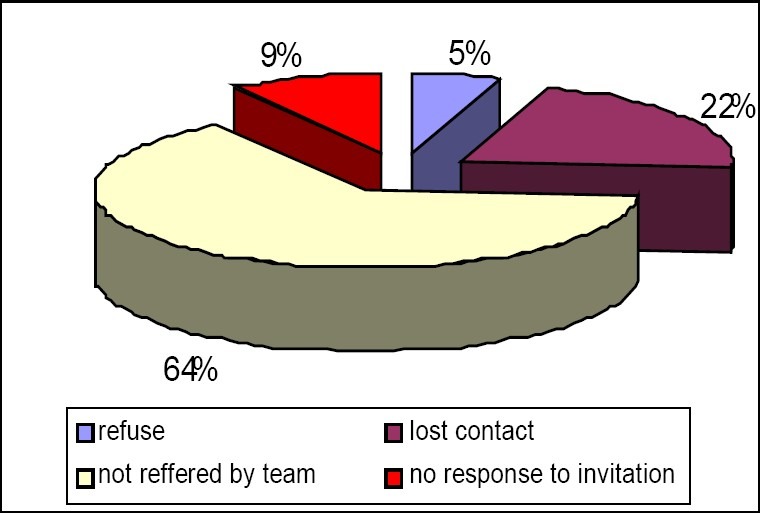
Percentage of screened positive for blood pressure and glucose according to the confirmation scenario
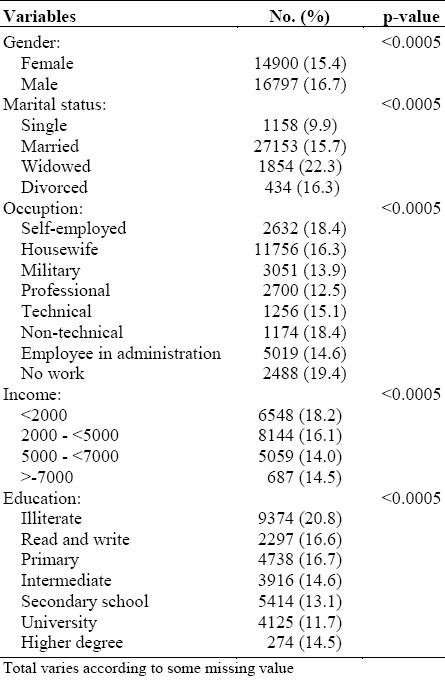
The results revealed that significantly more men than women were screened positive and needed referral for confirmatio (p<0.0005),(Table 3) but more women (9,594) 55.5% than men (7,700) 44.5% (p<0.0005) had successful referral. Of the fifteen sectors in the Eastern Province, the percentage of those who screened positive and needed referral was higher in the rural areas, 3030 (20.2%), compared with 28,674 (15.7%) in the urban areas. The percentage of non-referral of positively screened individuals for result confirmation was highest in Jubail 907 (91.3%), followed by Nuairia 607 (81.6%) and Dammam 2,836 (57.9%), while the best performance in the confirmation of results for subjects who were screened positive was in Hafr Al-Baten 1,902 (99%), (p<0.0005), attaining the highest rate of compliance for confirmation.
Table 3.
Comparison of different demographic variables according to screened positive subjects
It was observed that the most frequent venue of non- referral of screened positive cases were from MOH hospitals 1681(75.1%), followed by mobile teams 2,068(72.4%), while the highest percentage of successful referral were through PHCCs 13,375 (67.9%) followed by other government hospitals 656 (67.2%) (p<0.0005). In addition, the lowest percentage for the loss of contact with the participants was at PHCCs 1215 (6.2%) followed by other government hospitals 61 (6.3%), while highest rates of loss of contact were at (MOH) hospitals 524 (23.4%) and mobile teams 450(15.8%) p<0.0005.
The highest percentage of individuals who were screened positive but who refused referral came from the teams at the various public places 166 (6%), followed by private hospitals 159 (5.2%), while the lowest was from PHCCs 230 (1.2%) and MOH hospitals 44(2%) p<0.0005. Most of the participants who didn't receive confirmation of their results were around the cut-off point for systolic 140 and diastolic blood pressure 90 (4,429) 55.4%, compared with higher reading 3,654 (49.4%) p<0.0005. The same obtained for individuals with border line values of FBS (100-125) 4,682 (40.1%) compared with higher blood glucose 1,625 (38.9%) p<0.0005.
DISCUSSION
This is the largest community-based screening campaign for diabetes mellitus and hypertension in Saudi Arabia. Although there have been many studies on diabetes mellitus and hypertension, most involved numbers that were lower than ours; very few were done on a large scale. The participation rate in our study was 33% of the target population which was lower than the campaign done in Brazil and Mexico,3,35 but is much higher than that done in the New York city.36 This may be attributed to the easy access the people of Saudi Arabia have to health care. This is evident in the variety of responses from rural to urban areas ranging from 24% in some urban areas to 100% in some rural areas. Another explanation for the relatively low participation rate, as indicated.by the Inter99 study37 could be that the healthier population showed up for examination, while the sick could not. It may be that the health personnel involved in the campaign were overloaded with work, for besides their normal work they had to undertake the screening program without any incentives. This might have played a major role in their attitude towards inviting more participants to the campaign. This can be evidenced by the fact that quite a large number of participants who needed test confirmation, were not referred. The reason could also be that the large number of health teams working in this campaign made coordination more difficult. The reason for the non-appearance of a large number of participants for the confirmation test could be the participants’ refusal to accept the screening result, or as explained by Lawrence JM et al8 in their having to fast before the test. The study revealed a variation among the sectors in the number of cases who were screened positive and needed confirmation. This was considerably higher in the rural sectors, possibly because of the lack of efficient health care and public awareness.
Complete coverage with follow-up for confirmation of results noted in Hafr Albaten could be attributed to the commitment and the organizational ability of the personnel. In some other sectors, the lack of commitment resulted in a lower percentage of confirmation for screened positive cases than in other sectors.
It was noted that the higher proportion of participants who were not referred for result confirmation, were those whose results were around the cut-off point. This may be because of the recent recommendation of American Diabetic Association (ADA) to lower the level of what constituted impaired fasting blood sugar from 110-125 to 100-125 mg/dl, a position about which the health personnel working in the campaign, remained unconvinced, in spite of previous orientation and training. This raises the important issue of the lack of strict adherence to methodological guidelines, particularly noted from the excluded forms (mentioned above), the level of which was higher in the Michigan screening program,38 in which, 14% of the 3506 screened individuals were excluded. We found that in terms of high coverage the number of positive screening with successful referral and follow-up, was high at PHCCs while mobile teams, other public venues had the disadvantage of a limited coverage and the failure to confirm positive screening owing to the loss of contact, or shortage of time and manpower. This goes to show that the PHCCs were the best venues for screening, and the support they give the public in educating them about modification of dietary habits, increase in physical exercise, and weight control.
This campaign has important implications for screening. First, the most successful strategy for screening and confirmation of test results was through PHCCs. Second, follow-up after screening in other public places was poor. Third, the rural areas, which lack effective health care services, need more screening than the urban areas. Fourth, a motivated health team with good coordination is the cornerstone for a successful campaign.
ACKNOWLEDGMENT
The campaign was supported in part by Al-Dawaa Pharmacy and Qusaibie Company. We thank Dr. Mona. H. Hassan, PhD, Biostatistics, for her assistance. We are most grateful to all the health workers and local coordinators in all the sectors who supported us in various ways to conduct this campaign. The authors would also like to thank Dr. Mohamed Al-Qadri, Dr. Attia Taha, and Dr. Ahmed Bahnnasy for their advice and support.
REFERENCES
- 1.American Diabetes Association Standards of Medical Care in Diabetes-2006. Diabetes Care. 2006;29:S4–S42. [PubMed] [Google Scholar]
- 2.Chobanian AV, Bakris GL, Black HR, et al. National High Blood Pressure Education Program Coordinating Committee.The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC 7 Report. JAMA. 2003;289:2560–71. doi: 10.1001/jama.289.19.2560. [DOI] [PubMed] [Google Scholar]
- 3.The World Health Organization. Geneva: World health Organization; 2003. Screening of type 2 diabetes.Report of World Health Organization and International diabetes federation meeting. [Google Scholar]
- 4.Wild S, Roglic G, Green A, Sicree R, King H. Global prevalence of diabetes estimate for the year 2000 and projections for 2030. Diabetes Care. 2004;27:1047–53. doi: 10.2337/diacare.27.5.1047. [DOI] [PubMed] [Google Scholar]
- 5.Mokdad AH, Ford ES, Bowman BA, et al. Diabetes trends in the U.S:1990-1998. Diabetes Care 2000. 23:1278–83. doi: 10.2337/diacare.23.9.1278. [DOI] [PubMed] [Google Scholar]
- 6.Harris R, Donahue K, Rathore S, Frame P, Woolf S, Lohr K. Screening Adults for Type 2 Diabetes: A Review of the Evidence for the U.S. Preventive Services Task Force. Annals of Internal Med. 2003;138(3):215–29. doi: 10.7326/0003-4819-138-3-200302040-00015. [DOI] [PubMed] [Google Scholar]
- 7.Engelgau MM, Narayan KMV, Herman WH. Screening for type 2 diabetes. Diabetes Care. 2000;23:1563–80. doi: 10.2337/diacare.23.10.1563. [DOI] [PubMed] [Google Scholar]
- 8.Lawrence JM, Bennett P, Young A, Robinson AM. Screening for diabetes in general practice: Cross sectional population study. BMJ. 2001;323:548–51. doi: 10.1136/bmj.323.7312.548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.U.S. Preventive Services Task Force. 2003. Jul, High Blood pressure screening. [Google Scholar]
- 10.Al-Nozha MM, Al-Maatouq MA, Al-Mazrou YY, et al. Diabetes mellitus in Saudi Arabia. Saudi Med J. 2004;25(11):1603–10. [PubMed] [Google Scholar]
- 11.Osman Ak, Al-Nozha MM. Risk factors of coronary artery disease in different regions of Saudi Arabia. East Mediterr Health J. 2000;6(2-3):465–74. [PubMed] [Google Scholar]
- 12.Karim A, Ogbeide DO, Siddiqui S, AL-Khalifa IM. Prevalence of diabetes mellitus in Saudi community. Saudi Med J. 2000;21(5):438–42. [PubMed] [Google Scholar]
- 13.Kalantan KA, Mohamed AG, AL-Taweel AA, Abdul Ghani HM. Hypertension among attendants of primary health centers in AL-Qassim region, Saudi Arabia. Saudi Med J. 2001;22(11):960–3. [PubMed] [Google Scholar]
- 14.El-Hazmi MA, Warsy AS. Prevalence of hypertension in obese and non-obese Saudis. Saudi Med J. 2001;22(1):44–8. [PubMed] [Google Scholar]
- 15.Al-Nozha MM, Abdullah M, Arafah MR, Khalil MZ, et al. Hypertension in Saudi Arabia. Saudi Med J. 2007;28(1):77–84. [PubMed] [Google Scholar]
- 16.Harris MI, Flegal KM, Cowei CC, et al. Prevalence of diabetes, impaired fasting glucose and impaired glucose tolerance In U.S. adults. The third national health and nutrition examination survey, 1988-1994. Diabetes care. 1998;21(4):518–24. doi: 10.2337/diacare.21.4.518. [DOI] [PubMed] [Google Scholar]
- 17.Harris MI, Klein R, Welborn TA, Knuiman MW. Onset of NIDDM occurs at least 4-7 yr before clinical diagnosis. Diabetes Care. 1992;15:815–9. doi: 10.2337/diacare.15.7.815. [DOI] [PubMed] [Google Scholar]
- 18.Oliveria JE, Milech A, Franco LJ The Cooperative Group for the Study of Diabetes Prevalence in Rio De Janeiro. The prevalence of diabetes in Rio de Janeiro, Brazil. Diabetes Care. 1996;19(6):663–6. doi: 10.2337/diacare.19.6.663. [DOI] [PubMed] [Google Scholar]
- 19.Satman I, Yilmaz T, Sengül A, et al. Population-based study of diabetes and risk characteristics in Turkey: result of the Turkish diabetes epidemiology study (TURDEP) Diabetes Care. 2002;25:1551–6. doi: 10.2337/diacare.25.9.1551. [DOI] [PubMed] [Google Scholar]
- 20.Colagiuri S, Colagiuri R, Na’ati S, Muimuiheata S, Hussain Z, Palu T. The prevalence of diabetes in the Kingdome of Tonga. Diabetes care. 2002;25:1378–83. doi: 10.2337/diacare.25.8.1378. [DOI] [PubMed] [Google Scholar]
- 21.Clark CM, Fradkin JE, Hiss RG, Lorenz RA, Vinicor F, Warren-Boulton E. Promoting early diagnosis and treatment of type 2 diabetes: the National Diabetes Education Program. JAMA. 2000;284:363–5. doi: 10.1001/jama.284.3.363. [DOI] [PubMed] [Google Scholar]
- 22.Levin SR, Coburn JW, Abraira C, et al. Effect of intensive glycemic control on microalbuminuria in type 2 diabetes.Veterans Affairs Cooperative Study on Glycemic Control and Complications in Type 2 Diabetes Feasibility Trial Investigators. Diabetes Care. 2000;23(10):1478–85. doi: 10.2337/diacare.23.10.1478. [DOI] [PubMed] [Google Scholar]
- 23.United Kingdom Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–53. [PubMed] [Google Scholar]
- 24.Shichiri M, Kishikawa H, Ohkubo Y, Wake N. Long-term results of the Kumamoto Study on optimal diabetes control in type 2 diabetic patients. Diabetes Care. 2000;23:B21–9. [PubMed] [Google Scholar]
- 25.UK Prospective Diabetes Study (UKPDS) Group. Effect of intensive blood-glucose control with metformin on complications in overweight patients with type 2 diabetes (UKPDS 34) Lancet. 1998;352:854–65. [PubMed] [Google Scholar]
- 26.Pan XR, Li GW, Hu YH, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance: the Da Qing IGT and Diabetes Study. Diabetes Care. 1997;20:537–44. doi: 10.2337/diacare.20.4.537. [DOI] [PubMed] [Google Scholar]
- 27.Knowler WC, Barrett-Connor E, Fowler SE, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346:393–403. doi: 10.1056/NEJMoa012512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tuomilehto J, Lindstrom J, Eriksson JG, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344:1343–50. doi: 10.1056/NEJM200105033441801. [DOI] [PubMed] [Google Scholar]
- 29.Buchanan TA, Xiang AH, Peters RK, et al. Preservation of pancreatic β-cell function and prevention of type 2 diabetes by pharmacological treatment of insulin resistance in high-risk Hispanic women. Diabetes. 2002;51:2796–803. doi: 10.2337/diabetes.51.9.2796. [DOI] [PubMed] [Google Scholar]
- 30.The Diabetes Prevention Program Research Group. Prevention of type 2 diabetes with troglitazone in the Diabetes Prevention Program. Diabetes. 2005;54:1150–6. doi: 10.2337/diabetes.54.4.1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Segal L, Dalton AC, Richardson J. Cost-effectiveness of the primary prevention of non-insulin dependent diabetes mellitus. Health Promotion International. 1998;13:197–209. [Google Scholar]
- 32.Dabelea D, Hanson RL, Bennett PH, Roumain J, Knowler WC, Pettitt DJ. Increasing prevalence of type 2 diabetes in American Indian children. Diabetologia. 1998;41(8):904–10. doi: 10.1007/s001250051006. [DOI] [PubMed] [Google Scholar]
- 33.Rosenbloom AL, Joe JR, Young RS, Winter WE. Emerging epidemic of type 2 diabetes in youth. Diabetes Care. 1999;22:345–54. doi: 10.2337/diacare.22.2.345. [DOI] [PubMed] [Google Scholar]
- 34.American Diabetes Association. Screening for type 2 diabetes. Diabetes Care. 2004;27:S11–S14. doi: 10.2337/diacare.27.2007.s11. [DOI] [PubMed] [Google Scholar]
- 35.Nucci LB, Toscano CM, Maia ALM, et al. Brazilian National Campaign for Diabetes Mellitus Detection Working Group. A nationwide population screening program for diabetes in Brazil. Revista Panamericana de Salud Púlica/Pan American Journal of Public Health. 2004;16(5):320–7. doi: 10.1590/s1020-49892004001100005. [DOI] [PubMed] [Google Scholar]
- 36.Hosler AS, Berberian EL, Spence MM, Hoffman DP. Outcome and cost of a statewide diabetes screening and awareness initiative in New York. J Public Health Manag Pract. 2005;11(1):59–64. doi: 10.1097/00124784-200501000-00010. [DOI] [PubMed] [Google Scholar]
- 37.Glümer C, Jørgensen T, Borch-Johnsen K. Prevalence of Diabetes and Impaired Glucose Regulation in a Danish Population .The Inter99 study. Diabetes Care. 2003;26:2335–40. doi: 10.2337/diacare.26.8.2335. [DOI] [PubMed] [Google Scholar]
- 38.Tabaei B, Burke R, Constance A, et al. Community-Based Screening for Diabetes in Michigan. Diabetes Care. 2003;26:668–70. doi: 10.2337/diacare.26.3.668. [DOI] [PubMed] [Google Scholar]