

Abstract
Little is known about how individuals might interpret brief genetic risk feedback. We examined interpretation and behavioral intentions (sun protection, skin screening) in melanoma first-degree relatives (FDRs) after exposure to brief prototypic melanoma risk feedback. Using a 3 by 2 experimental pre-post design where feedback type (high-risk mutation, gene environment, and nongenetic) and risk level (positive versus negative findings) were systematically varied, 139 melanoma FDRs were randomized to receive one of the six scenarios. All scenarios included an explicit reminder that melanoma family history increased their risk regardless of their feedback. The findings indicate main effects by risk level but not feedback type; positive findings led to heightened anticipated melanoma risk perceptions and anticipated behavioral intentions. Yet those who received negative findings often discounted their family melanoma history. As such, 25%, 30%, and 32% of those who received negative mutation, gene-environment, and nongenetic feedback, respectively, reported that their risk was similar to the general population. Given the frequency with which those who pursue genetic testing may receive negative feedback, attention is needed to identify ideal strategies to present negative genetic findings in contexts such as direct to consumer channels where extensive genetic counseling is not required.
1. Background
The sequencing of the entire human genome in 2003 has led to a series of unrealized opportunities for public health benefit [1], many of which rest on accurate genetic risk interpretation and adoption of protective behavior [2]. By 2006, direct-to-consumer genetic testing and feedback was available through 24 Internet-based companies, many of which did not require physician or genetic counseling followup to ensure accurate interpretation of test findings [3]. Recent general population surveys indicate high levels of risk misinterpretation even among highly educated general population subgroups [4–6]. To date, the few studies that have examined outcomes associated with direct-to-consumer genetic testing have found no remarkable increases in distress, screening, or behavior change [7–9], yet it is unclear whether these findings may be due to risk misinterpretation, or lack of consideration of diverse elements of risk, including family history.
First-degree relatives (FDRs) of cancer patients may be among the first to pursue cancer genetic susceptibility testing through direct-to-consumer channels, given their heightened risk salience [10]. Among FDRs, interpretation of “negative findings”—the absence of an identified higher risk genetic risk variant—may present a particular challenge, because most of those tested will receive negative findings due to low population prevalence of risk mutations and common risk variants, and because it is unclear how negative genetic findings may be interpreted in the context of other relevant risk factors such as family history. LaRusse and colleagues [11] compared women's interpretation of genetic versus family history risk assessment “negative findings” (identical 29% lifetime estimates of developing Alzheimer's disease) and found that those who received genetic risk feedback reported lower perceived risk and lower anxiety about developing the disease than those who received family history risk assessment. Accordingly, genetic test results indicating negative or uncertain findings may prove to be more salient and impactful than family history information, increasing the probability of diverse risk interpretations and continued information seeking [12, 13], variations in recall of test findings [14], and justifications for continued risk behavior [15].
To closely examine message interpretation and behavioral intentions given plausible genetic risk feedback, we examined these outcomes among individuals with a family history of melanoma. Melanoma is an ideal study context given the established genetic (high-risk mutations, as well as more common genetic variants) and environmental (ultraviolet radiation exposure) risks for this common cancer [16], and the need to enhance early detection and risk reduction strategies in melanoma FDRs [17]. This study employed an experimental pre-post design to assess message interpretation (aim I) and behavioral intentions (sun protection and skin screening, aim II) associated with receipt of hypothetical risk feedback modeled on varied prototypic melanoma genetic risk feedback in melanoma FDRs.
2. Methods
2.1. Participants
Melanoma FDRs (N = 139) participated in the study. With the approval of each patient's physician, 426 melanoma patients (English fluent, ≥age 18) were approached at their postsurgical followup appointments at Memorial Sloan-Kettering's (MSK) Gastric and Mixed Tumor Service by a research study assistant (RSA) who described the study, provided a brochure, and requested patients' assent to contact their eligible FDRs by telephone. Most patients (74%) stated initial willingness to refer an FDR when they were approached in clinic, and 66% of patients provided us with adequate referral information (name, relation to the patient, and telephone and contact information) for us to contact their FDR. Of the 280 FDRs who were referred, 50% participated (N = 139), 44% were unavailable by telephone after five attempts to reach them, and 6% refused participation. Those FDRs who participated did not differ in gender from those who did not participate. Study questionnaires were completed either by telephone or in clinic if the FDR was accompanying the patient. The sample was 70% female, 97% non-Hispanic white, highly educated (71% had a college degree) and mostly (78%) comprised daughters, sons, and mothers; all included participants were unrelated to each other. Few (8%) had more than one family member with melanoma; 14% had a personal melanoma history. Half (54%) had a sun-sensitive phenotype indicating skin prone to burning (skin type I/II; [18]). The study was approved by the MSKCC Institutional Review Board.
2.2. Design and Procedure
The study used a 3 by 2 experimental design where feedback type and risk level of the scenarios were varied, and participants were randomized to one of the six conditions. For feedback type, “mutation feedback” was modeled on inherited mutations in CDKN2A (gene encoding p16INK4A), an identified tumor suppressor gene, that has been linked to hereditary melanoma (melanoma diagnosed in a family with two or more affected relatives; [19]). “Gene-environment feedback” was modeled on the melanocortin receptor gene (MC1R), which interacts with sun exposure to heighten population melanoma risk [20]. “Nongenetic feedback” was based on a nongenetic melanoma risk assessment that includes factors such as mole number [21]. Risk level was varied by whether the findings were positive (test identified higher risk genetic marker/nongenetic risk information) or negative. The RSA slowly reads one of six testing scenarios to each participant.
The following elements recommended by Persky and colleagues [22] were used to increase the accuracy of testing outcomes, including verbal elements to increase verbal immediacy of the scenario, use of a request to “imagine” they are having the test, the use of second person (“you”), a test administrator (nurse), a description of the test context in concrete terms, a description of each “new test” as immediately available, inclusion of detail about the tests (blood test, the heritability of melanoma, and the bases on which risk is determined for each test type), the use of a brief, relatively low text-dense scenario description, and finally random assignment to condition and slow, verbal presentation by the RSA.
All scenarios explicitly reminded participants that their melanoma family history raised their risk.
The information varying across conditions is presented in brackets:
-
Please vividly imagine that you find yourself in the situation described below. Think hard about how you would feel and what you would think in this situation.
-
Imagine that you learn from your doctor that there is a new test that will provide information about a person's risk of developing melanoma. [This genetic test involves giving a blood sample that is tested for a gene mutation that places a person at increased risk for developing melanoma/This genetic test involves giving a blood sample that is tested for a common genetic difference that makes someone more susceptible to the negative effects of sunlight and sunburn/This test involves a brief series of questions about whether you have had skin cancer before, freckling and number of large moles, how sun-sensitive you are, and sunburn history.] You know that as a close family member of someone who has had melanoma, that your risk is already increased, regardless of your test results. Imagine that you decide to take this test. [A nurse takes a sample of blood from you for this purpose (deleted for non-genetic feedback)]. Three days later you receive the test results. The results of the test are [positive/negative.]
2.3. Measures of Test Comprehension and Behavioral Intentions
Pretest Assessment —
Prior to scenario administration, we assessed perceived risk using established methods [23]. Accordingly, we assessed absolute verbal likelihood of developing melanoma (“How likely is it that you will develop melanoma in the future? Would you say your chance of getting melanoma is …” assessed on a 5-point scale, “very low” to “very high”) and comparative likelihood of developing melanoma compared to same age and sex others (“Compared to the average person your age, would you say that you are …” assessed on a 3-point scale, “less likely to get melanoma,” “about as likely to get melanoma,” or “more likely to get melanoma”). Current self-reported sun protection practices (use of sunscreen, shirts, hats, shade seeking, and sunglasses when outside on a sunny summer day for more than an hour) were assessed on separate 5-point scales, “Never” to “Always,” [24]. History of healthcare provider skin cancer screening and skin self-examination (history of prior screening, no history of prior screening) was also assessed.
Posttest Assessment —
The posttest assessment was conducted immediately subsequent to scenario administration. Scenario interpretation was assessed two ways—through a multiple-choice item (see Table 1) and by a second administration of the same perceived skin cancer risk questions that were assessed at pretest [23]. Intentions for future sun protection practices (use of sunscreen, shirts, hats, shade seeking, and sunglasses when outside for more than one hour on separate 5-point scales, “Never” to “Always,” [24] and healthcare provider and self-screening intentions (intend, not intend) as well as basic demographic and skin type information) were assessed.
Table 1.
Scenario interpretation response frequencies (N = 139).
| My test results indicate the following | Scenario version n (%) | |||||
|---|---|---|---|---|---|---|
| Mutation positive | Mutation negative | GE positive | GE negative | Nongenetic risk positive | Nongenetic risk negative | |
| My melanoma risk is unknown | 0 (0.0) | 1 (4.2) | 0 (0.0) | 1 (4.3) | 0 (0.0) | 3 (13.6) |
| I am certain to never get melanoma | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| My risk is decreased | 0 (0.0) | 8 (33.3) | 0 (0.0) | 7 (30.4) | 1 (4.3) | 9 (40.9) |
| My risk is not really different from the population | 1 (4.2) | 6 (25.0) | 1 (4.3) | 7 (30.4) | 1 (4.3) | 7 (31.8) |
| My risk is not really different from other people with a melanoma family history | 4 (16.7) | 9 (37.5) | 6 (26.1) | 4 (17.4) | 5 (21.7) | 1 (4.5) |
| My risk is increased | 16 (66.6) | 0 (0.0) | 16 (69.6) | 4 (17.4) | 16 (69.6) | 2 (9.1) |
| I am certain to get melanoma in the future | 3 (12.5) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
|
| ||||||
| Participants (% total) | 24 (17.3) | 24 (17.3) | 23 (16.5) | 23 (16.5) | 23 (16.5) | 22 (15.8) |
GE: gene environment.
2.4. Statistical Analysis
To assess message interpretation (aim I), multiple-choice responses are reported descriptively, and via pre-post melanoma perceived risk assessed with a 3 by 2 analyses of covariance (ANCOVA), with vignette type and vignette risk level as the independent variables, controlling for pretest perceived risk. To assess anticipated sun protection behavioral intentions (aim II), hierarchical linear modeling (HLM; [25]) was employed to examine sun protection (intended use of sunscreen, shirts, hats, shade seeking, and sunglasses on separate 5-point scales, “Never” to “Always”) given the presumed correlation between outcomes, treating study id as the sole random effect. Statistical evidence was evaluated by the type-III test of Wald statistic, using the MIXED procedure in the SPSS statistical package (v.18). For the dichotomous outcome of skin examination (intend/not intend screening), a generalized estimating equation (GEE; [26]) was used to examine intended skin cancer screening (by healthcare provider as well as skin self-examination). Statistical evidence in the GEE was evaluated by the generalized score tests for type III contrasts using the SAS statistical package (v9.2). The independent variables in the HLM and GEE models were vignette type, vignette risk level, and an interaction between vignette type and risk level. We did not include pretest sun protection behaviors in the HLM, nor pretest skin cancer screening in the GEE models because of sample size limitations [27].
3. Results
Randomization was balanced, as indicated by the lack of significant pretest differences in participants' reported sun protection behaviors and skin cancer screening across participants randomized to different experimental conditions. There were no significant differences across conditions in whether participants reported a sun-sensitive phenotype, whether they had one or more family members with melanoma, nor whether they had a prior personal melanoma history.
3.1. Interpretation of Prototypic Skin Cancer Risk Feedback (Aim I)
Positive feedback was interpreted more consistently than negative feedback across all feedback types (see Table 1). Of those who received mutation-positive feedback, two-thirds (67%) interpreted their results to mean that their melanoma risk was increased. Those who received mutation negative findings had more diverse interpretations—only one-third (38%) equated their risk to others with a family history of melanoma, yet 33% reported that their risk was decreased, and 25% reported that their risk did not differ from that of the general population. Interpretation of gene-environment risk feedback showed a similar pattern. Most of those who received positive gene-environment feedback (70%) interpreted their results to mean that their melanoma risk was increased, but of those who received negative gene-environment feedback, 30% reported that their risk was decreased, and 30% reported that their risk was similar to the general population. The pattern was similar for those receiving nongenetic feedback as well. Most of those who received positive feedback (70%) interpreted their results to mean that their melanoma risk was increased, but of those who received negative feedback, 41% reported that their risk was decreased, and 32% reported that their risk was similar to the general population. Interestingly, compared to those who received negative gene environment and nongenetic feedback, more who received positive gene environment and nongenetic feedback interpreted their findings to mean that their risk was not different from others with a melanoma family history. Interpretations that melanoma was either ruled out, or inevitable, were almost nonexistent, with the only three participants who reported certainty that they would get melanoma all having received mutation-positive feedback.
To examine the effect of feedback type (mutation, gene environment, nongenetic) and risk level (positive or negative findings) on perceived melanoma risk, two 3 by 2 ANCOVAs (feedback type by risk level, controlling for pretest perceived risk) were used. Main effects for risk level for both verbal absolute risk and comparative risk were found, F(1,132) = 59.22, P < 0.0001; F(1,132) = 37.37, P < 0.0001, respectively, such that those who received positive findings had significantly heightened anticipated perceived risk for all types of feedback; those who received negative findings had significantly reduced anticipated perceived risk for all types of feedback. There were no significant main effects for feedback type (mutation, gene environment, nongenetic) nor any significant interactions (all Ps > 0.60; see Figure 1).
Figure 1.
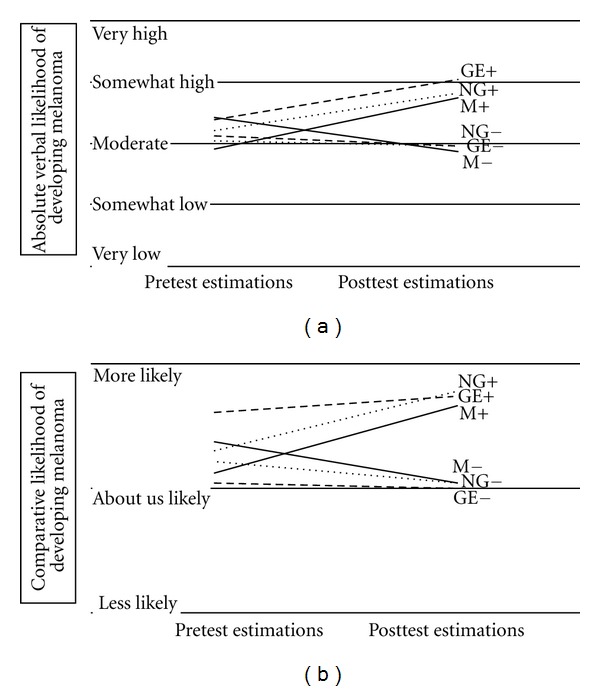
Changes in melanoma risk perceptions (Pretest-posttest). (a) Absolute verbal likelihood. How likely is it that you will develop melanoma in the future? Would you say your chance of getting melanoma is …? (b) Comparative likelihood. Compared to the average person your age, would you say that you are more, less, or about as likely to develop melanoma? GE (gene environment), NG (nongenetic), and M (mutation) are denoted according to feedback, positive or negative (+/–).
3.2. The Influence of Risk Feedback on Behavioral Intentions (Aim II)
Intentions for all sun protection, Wald F(1, 134.27) = 3703.72, P < 0.0001 and skin cancer screening, GEE: χ2(1, N = 139) = 5.09, P = 0.02, were higher among those receiving positive versus negative feedback. Feedback type was not a significant predictor in either the MIXED model (P = 0.37) or the GEE (P = 0.18), and there were no significant interactions (P = 0.74 and P = 0.30, resp.). Figure 2 depicts both pretest (self-reported behavior) and posttest (intended changes in behavior) findings. Those who received positive versus negative feedback showed higher levels of intending to maintain consistent (often or always) sunscreen use such that they reported high pretest sunscreen use and high posttest intentions for sunscreen use. For example, 67% who received positive feedback intended to maintain consistent sunscreen versus 59% of those who received negative feedback. Positive feedback led to higher intentions to adopt consistent (often or always) shade seeking, such that those who did not report consistent shade seeking at pretest reported that they intended to adopt it at posttest. Those who received positive versus negative feedback showed higher levels of intending to maintain healthcare provider screening, as well as increased intentions to adopt skin self-examination. Findings regarding intended use of shirts, hats, and sunglasses are not shown but followed the same pattern.
Figure 2.
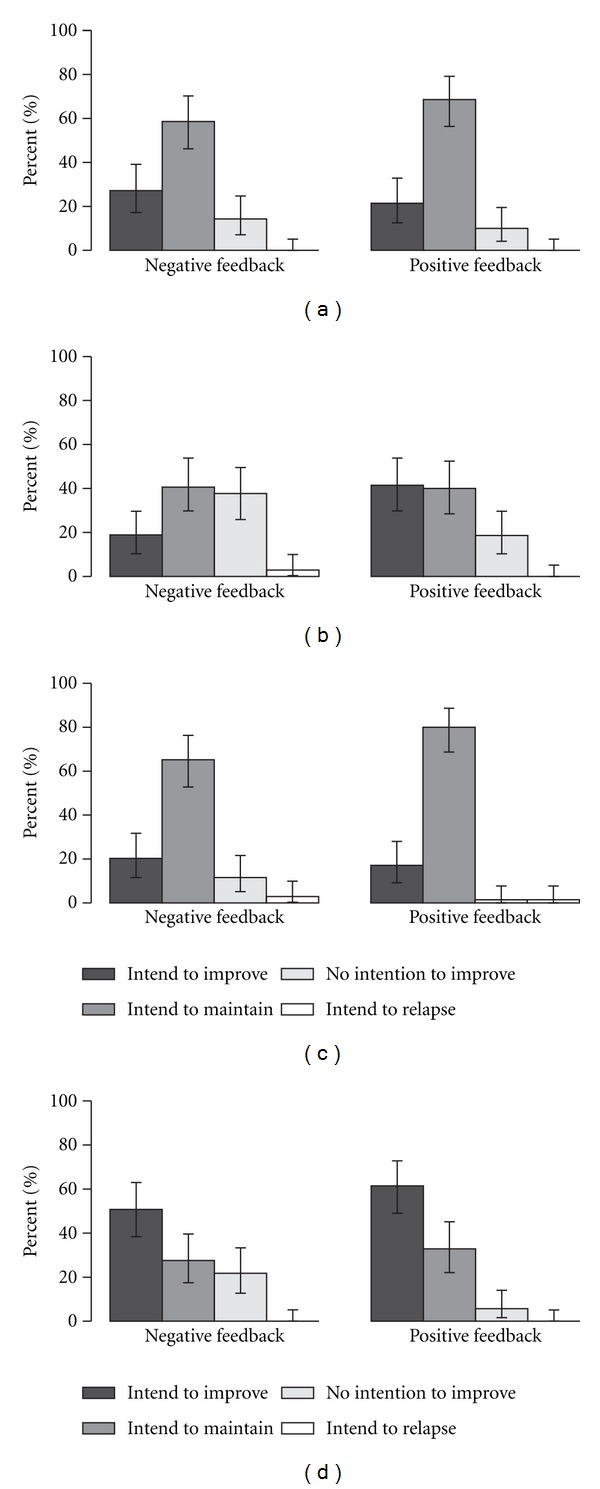
Changes in intentions regarding sun protection and screening (pretest-posttest). (a) Sunscreen use. (b) Shade seeking. For sunscreen use and shade-seeking outcomes, intend to improve is indicated by lower pretest utilization (never, sometimes) and higher posttest intentions (often or always). Intend to maintain is indicated by higher pretest utilization (often or always) and higher posttest intentions (often or always). No intention to improve is indicated by lower pretest utilization (never, sometimes) and lower posttest intentions (never, sometimes). Finally, intend to relapse is indicated by higher pretest utilization (often or always) and lower posttest intentions (never, sometimes). (c) Skin cancer screening by a healthcare professional. (d) Skin cancer self-screening. For screening outcomes, intend to improve is indicated by no reported prior screening at pretest but intentions to screen at posttest. Intend to maintain is indicated by reported prior screening at pretest and intentions to screen at posttest. No intention to improve is indicated by no reported prior screening at pretest and no intentions to screen at posttest. Intend to relapse are indicated by reported prior screening at pretest, yet no intentions to screen at posttest.
4. Discussion
This study found that the positive versus negative dimension of the prototypic melanoma risk feedback consistently influenced melanoma FDRs' melanoma risk perceptions as well as behavioral intentions. Those study participants receiving positive feedback anticipated higher-risk perceptions compared to pretest levels; those participants receiving negative feedback anticipated lower-risk perceptions compared to pretest levels as evaluated in aim I. Similarly, as evaluated in aim II, anticipated intentions for protective behaviors (such as use of sunscreen and shade-seeking) and screening (provided by a health-care provider, as well as self-screening) increased more among those who received positive risk feedback, confirming the theoretical connection between increased risk judgments and intentions to self-protect [28]. Recent studies have documented that individuals at moderate cancer risk are not highly sensitive to low-penetrance genetic quantitative risk magnitude and pictorial information [29–31] and that findings regarding whether a test was “positive” or “negative” may be more salient than the exact percentage risk feedback [11]. Indeed, genetic risk feedback necessarily contains two dimensions: first, whether a genetic mutation or risk variant is identified or not; second, what quantitative risk level the genetic mutation or variant confers. This may be because the easily understood “gist” is the presence or absence of the risk-conferring gene mutation or variant. It may be that the risk level is only salient to those who have already been identified to have a risk-conferring genetic factor present. For those receiving negative feedback, or feedback that a risk-conferring genetic factor is not present, it may be most important for them to integrate their findings with other relevant personal risk information.
We found that negative feedback led to more varied interpretations than positive feedback, with over half of those receiving negative feedback interpreting their feedback as either decreased melanoma risk, or as risk similar to the general population. It is possible that some of those receiving negative feedback may have discounted their family history—despite the clarity with which this information was presented—either defensively [14], or because of a recency effect [32] since hypothetical genetic feedback findings were presented subsequent to the family history risk statement. This is of potential concern given that early adopters of genetic testing outside the high-risk clinic are likely to include those with family disease histories who may be more motivated to use their genetic test findings to minimize their concerns than to amplify them. Some who received positive feedback did not interpret their risk to exceed that of others with a melanoma family history, as this was a more common interpretation among those who received positive (versus negative) gene environment or nongenetic feedback. Suggestions for careful presentation of negative findings include prominent repetition of reminders about other relevant risk factors, including family history, after genetic test findings are conveyed, as well as consideration of whether different types of risk information can and should be integrated in genetic risk calculations. Most importantly, we advocate for the careful evaluation of message interpretation and comprehension prior to the use of these messages in direct-to-consumer contexts.
An analog study presents both opportunities and limitations. The use of scenarios is a widely used research strategy to examine decision-making processes associated with genetic testing [22]. It is possible that the brevity of prototypic feedback may have impeded interpretations of negative findings, in particular. Another limitation involved the fact that 14% of our FDR participants also had a personal melanoma history, which was an additional source of risk heterogeneity in our sample. However, our results clearly showed that those who received positive feedback both increased their risk perceptions and showed higher intentions for behavior change, supporting relatively accurate interpretations of the positive versus negative feedback dimension. A strength of our study involved the use of first-degree family members of melanoma patients who are at actual increased melanoma risk based on their family history [33], as well as the fact that changes in risk judgments led to changes in intended behavior change predicted by major health behavior theories [28]. Our findings need to be confirmed in actual testing situations, with larger samples that will allow stratification across skin type, sun exposure histories, strength of family history, and whether individuals have a personal melanoma history, with longitudinal followup of actual sun protection and skin cancer screening adoption.
In conclusion, much remains to be learned regarding the translational behavioral potential of human genomics, especially outside of the high-risk setting where extensive genetic counseling will be unavailable or not required. Our study casts a spotlight on the need to conduct further research on those who receive negative genetic feedback, who may be relieved about their findings and yet discount other important cancer risk factors.
Acknowledgments
The authors acknowledge the Martell Foundation that funded the study. They thank Drs. Charlotte Ariyan, Mary Sue Brady, and Daniel Coit for providing clinic and patient access. They also thank Susan Gall, Marcel Ramos, and Christopher Webster for providing critical support in paper completion, Dr. Kevin McCaul and three anonymous reviewers for their useful input on the paper, and finally to their study participants for their valued participation.
References
- 1.Collins FS, Green ED, Guttmacher AE, Guyer MS. A vision for the future of genomics research. Nature. 2003;422(6934):835–847. doi: 10.1038/nature01626. [DOI] [PubMed] [Google Scholar]
- 2.Khoury MJ, Clauser SB, Freedman AN, et al. Population sciences, translational research, and the opportunities and challenges for genomics to reduce the burden of cancer in the 21st century. Cancer Epidemiology, Biomarkers and Prevention. 2011;20(10):2105–2114. doi: 10.1158/1055-9965.EPI-11-0481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Geransar R, Einsiedel E. Evaluating online direct-to-consumer marketing of genetic tests: informed choices or buyers beware. Genetic Testing. 2008;12(1):13–23. doi: 10.1089/gte.2007.0024. [DOI] [PubMed] [Google Scholar]
- 4.Gollust SE, Gordon ES, Zayac C, et al. Motivations and perceptions of early adopters of personalized genomics: perspectives from research participants. Public Health Genomics. 2012;15(1):22–30. doi: 10.1159/000327296. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Leighton JW, Valverde K, Bernhardt BA. The general public's understanding and perception of direct-to-consumer genetic test results. Public Health Genomics. 2012;15(1):11–21. doi: 10.1159/000327159. [DOI] [PubMed] [Google Scholar]
- 6.McGuire AL, Diaz CM, Wang T, Hilsenbeck SG. Social networkers’ attitudes toward direct-to-consumer personal genome testing. The American Journal of Bioethics. 2009;9(6-7):3–10. doi: 10.1080/15265160902928209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bloss CS, Schork NJ, Topol EJ. Effect of direct-to-consumer genomewide profiling to assess disease risk. The New England Journal of Medicine. 2011;364(6):524–534. doi: 10.1056/NEJMoa1011893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.James KM, Cowl CT, Tilburt JC, et al. Impact of direct-to-consumer predictive genomic testing on risk perception and worry among patients receiving routine care in a preventive health clinic. Mayo Clinic Proceedings. 2011;86(10):933–940. doi: 10.4065/mcp.2011.0190. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kaphingst KA, McBride CM, Wade C, et al. Patients' understanding of and responses to multiplex genetic susceptibility test results. doi: 10.1038/gim.2012.22. Genetics in Medicine. In press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.McBride CM, Emmons KM, Lipkus IM. Understanding the potential of teachable moments: the case of smoking cessation. Health Education Research. 2003;18(2):156–170. doi: 10.1093/her/18.2.156. [DOI] [PubMed] [Google Scholar]
- 11.LaRusse S, Roberts JS, Marteau TM, et al. Genetic susceptibility testing versus family history-based risk assessment: impact on perceived risk of Alzheimer disease. Genetics in Medicine. 2005;7(1):48–53. doi: 10.1097/01.gim.0000151157.13716.6c. [DOI] [PubMed] [Google Scholar]
- 12.Ersig AL, Hadley DW, Koehly LM. Understanding patterns of health communication in families at risk for hereditary nonpolyposis colorectal cancer: examining the effect of conclusive versus indeterminate genetic test results. Health Communication. 2011;26(7):587–594. doi: 10.1080/10410236.2011.558338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Ersig AL, Ayres L, Hadley DW, Koehly LM. Explanations of risk in families without identified mutations for hereditary nonpolyposis colorectal cancer. Journal of Nursing Scholarship. 2010;42(2):139–146. doi: 10.1111/j.1547-5069.2010.01342.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Lipkus IM, McBride CM, Pollak KI, Lyna P, Bepler G. Interpretation of genetic risk feedback among African American smokers with low socioeconomic status. Health Psychology. 2004;23(2):178–188. doi: 10.1037/0278-6133.23.2.178. [DOI] [PubMed] [Google Scholar]
- 15.Docherty SL, McBride CM, Sanderson SC, O'Neill SC, Shepperd JA, Lipkus IM. Young smokers' views of genetic susceptibility testing for lung cancer risk: minding unintended consequences. Journal of Community Genetics. 2011;2(3):165–172. doi: 10.1007/s12687-011-0053-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hay JL, Meischke HW, Bowen DJ, et al. Anticipating dissemination of cancer genomics in public health: a theoretical approach to psychosocial and behavioral challenges. Annals of Behavioral Medicine. 2007;34(3):275–286. doi: 10.1007/BF02874552. [DOI] [PubMed] [Google Scholar]
- 17.Bergenmar M, Brandberg Y. Sunbathing and sun-protection behaviors and attitudes of young Swedish adults with hereditary risk for malignant melanoma. Cancer Nursing. 2001;24(5):341–350. doi: 10.1097/00002820-200110000-00002. [DOI] [PubMed] [Google Scholar]
- 18.Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Archives of Dermatology. 1988;124(6):869–871. doi: 10.1001/archderm.124.6.869. [DOI] [PubMed] [Google Scholar]
- 19.d Snoo FA, Bergman W, Gruis NA. Familial melanoma: a complex disorder leading to controversy on DNA testing. Familial Cancer. 2003;2(2):109–116. doi: 10.1023/a:1025758527675. [DOI] [PubMed] [Google Scholar]
- 20.Raimondi S, Sera F, Gandini S, et al. MC1R variants, melanoma and red hair color phenotype: a meta-analysis. International Journal of Cancer. 2008;122(12):2753–2760. doi: 10.1002/ijc.23396. [DOI] [PubMed] [Google Scholar]
- 21.Glanz K, Schoenfeld E, Weinstock MA, Layi G, Kidd J, Shigaki DM. Development and reliability of a brief skin cancer risk assessment tool. Cancer Detection and Prevention. 2003;27(4):311–315. doi: 10.1016/s0361-090x(03)00094-1. [DOI] [PubMed] [Google Scholar]
- 22.Persky S, Kaphingst KA, Condit CM, McBride CM. Assessing hypothetical scenario methodology in genetic susceptibility testing analog studies: a quantitative review. Genetics in Medicine. 2007;9(11):727–738. doi: 10.1097/gim.0b013e318159a344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Weinstein ND. Unrealistic optimism about future life events. Journal of Personality and Social Psychology. 1980;39(5):806–820. [Google Scholar]
- 24.Glanz K, Yaroch AL, Dancel M, et al. Measures of sun exposure and sun protection practices for behavioral and epidemiologic research. Archives of Dermatology. 2008;144(2):217–222. doi: 10.1001/archdermatol.2007.46. [DOI] [PubMed] [Google Scholar]
- 25.Raudenbush SW, Bryk AS. Hierarchical Linear Models. 2nd edition. Vol. 1. Newbury Park, Calif, USA: Sage Publications; 2002. [Google Scholar]
- 26.Zeger SL, Liang KY. Longitudinal data analysis for discrete and continuous outcomes. Biometrics. 1986;42(1):121–130. [PubMed] [Google Scholar]
- 27.Peduzzi P, Concato J, Kemper E, Holford TR, Feinstem AR. A simulation study of the number of events per variable in logistic regression analysis. Journal of Clinical Epidemiology. 1996;49(12):1373–1379. doi: 10.1016/s0895-4356(96)00236-3. [DOI] [PubMed] [Google Scholar]
- 28.Conner M, Norman P. Predicting Health Behaviour: Research and Practice with Social Cognition Models. 2nd edition. Buckingham, UK: Open University Press; 2005. [Google Scholar]
- 29.Cameron LD, Sherman KA, Marteau TM, Brown PM. Impact of genetic risk information and type of disease on perceived risk, anticipated affect, and expected consequences of genetic tests. Health Psychology. 2009;28(3):307–316. doi: 10.1037/a0013947. [DOI] [PubMed] [Google Scholar]
- 30.Cameron LD, Marteau TM, Brown PM, Klein WMP, Sherman KA. Communication strategies for enhancing understanding of the behavioral implications of genetic and biomarker tests for disease risk: the role of coherence. Journal of Behavioral Medicine. 2012;35(3):286–298. doi: 10.1007/s10865-011-9361-5. [DOI] [PubMed] [Google Scholar]
- 31.Graves KD, Peshkin BN, Luta G, Tuong W, Schwartz MD. Interest in genetic testing for modest changes in breast cancer risk: implicationsfor SNP testing. Public Health Genomics. 2011;14(3):178–189. doi: 10.1159/000324703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Crowder RG. Principles of Learning and Memory. Hillsdale, NJ, USA: Erlbaum; 1976. [Google Scholar]
- 33.Ford D, Bliss JM, Swerdlow AJ, et al. Risk of cutaneous melanoma associated with a family history of the disease. International Journal of Cancer. 1995;62(4):377–381. doi: 10.1002/ijc.2910620403. [DOI] [PubMed] [Google Scholar]