

Abstract
Objectives.
Data from the Healthy Aging Network (HAN) study (Prohaska, T., Eisenstein, A., Satariano, W., Hunter, R., Bayles, C., Kurtovich, E., … Ivey, S. [2009]. Walking and the preservation of cognitive function in older populations. The Gerontologist, 49[Suppl. 1], S86–S93; and Satariano, W., Ivey, S., Kurtovich, E., Kealey, M., Hubbard, A., Bayles, C., … Prohaska, T. [2010]. Lower-body function, neighborhoods, and walking in an older population. American Journal of Preventive Medicine, 38, 419–428.) were used to examine the relationships among physical activity, self-efficacy, functional performance, and limitations.
Method.
Interviews were conducted within homes and senior centers in 4 geographic regions across the United States. Participants were 884 older adults (M age = 74.8; 77% female; 35% minority status) who completed measures of walking behavior, way-finding self-efficacy, walking self-efficacy, functional performance, functional limitations, and demographic characteristics.
Results.
Path analysis within a covariance modeling framework revealed significant direct effects of walking on self-efficacy constructs, functional performance on functional limitations, and efficacy on limitations. Additionally, significant indirect effects were also found, including walking on limitations via walking self-efficacy and performance and walking self-efficacy on limitations via performance. Furthermore, we found support for invariance of the model across geographical grouping.
Discussion.
Our findings provide further validation for an efficacy-based model of functional limitations. Walking-related efficacy may help reduce or possibly delay the onset of functional limitations.
Keywords: Aging, Functional limitations, Physical activity, Self-efficacy
IT has been well-established that functional limitations, for example, self-reported difficulty in stooping or kneeling, in older adults are associated with physical activity participation (Paterson & Warburton, 2010) and that such limitations have implications for compromised quality of life (Rejeski & Mihalko, 2001; Stuifbergen, Blozis, Harrison, & Becker, 2006). Given that functional limitations are risk factors for subsequent disability and institutionalization (Onder et al., 2005; Paterson, Govindasamy, Vidmar, Cunningham, & Koval, 2004) and for maintaining an independent lifestyle, understanding how physical activity levels influence such limitations represents an important public health endeavor. Stewart (2003) and others (Guralnik & Ferrucci, 2003; Huang, Perera, VanSwearingen, & Studenski, 2010; McAuley et al., 2006, 2007) have noted that this understanding has been made difficult by the treatment of functional limitations and functional performance (e.g., direct measures of lower body strength) as isomorphic constructs.
Functional limitations reflect perceptions regarding restrictions in one’s ability to effectively carry out discrete physical actions and activities such as ambulating, climbing stairs, and lifting (Verbrugge & Jette, 1994), all of which are sociocontextual in nature. Functional limitations represent an important part in the disablement process whereby physical, mental, or anatomical impairments lead to functional limitations, which in turn lead to disability (i.e., difficulties in executing day to day activities). This disablement model (Verbrugge & Jette, 1994) also incorporates compensatory strategies and environmental features which might serve to modify progress in the disablement process. Stewart (2003) has further suggested that functional performance should be included as an additional step in the disablement process preceding functional limitations. Specifically, Stewart argues that functional performance testing assesses a broad range of functioning that allows for more variation than self-reported functional limitations. Additionally, functional performance can capture subtle change in basic physical functions that may manifest prior to personal awareness of such change.
McAuley and colleagues (2006, 2007) have further extended this line of thinking by providing empirical evidence to support Stewart’s position and also demonstrating that self-efficacy expectations, as a more proximal outcome of physical activity participation, mediate the effects of physical activity on functional limitations. Self-efficacy, as the key factor in social cognitive theory (Bandura, 1986, 1997), reflects the individual’s beliefs in his or her capabilities to successfully carry out courses of action. Recently, McAuley and colleagues have reported baseline and longitudinal data from a sample of community-dwelling older women supporting the hypothesis that the relationship between physical activity and functional limitations was completely mediated by self-efficacy and functional performance.
It is important to note that efficacy expectations are both situation-specific and modifiable, thereby representing an important point for intervention. In the McAuley and colleagues (2006, 2007) studies, self-efficacy was assessed relative to balance and walking activities. However, there is evidence to suggest that neighborhood characteristics that do not favor walking (i.e., distance to parks and scarcity of sidewalks or trails) may reduce older adult walking behavior (for a review, see Owen, Humpel, Leslie, Bauman, & Sallis, 2004). Individuals living within neighborhoods that are ill-equipped for physical activity are more likely to be obese (Booth, Pinkston, & Poston, 2005; Poortinga, 2006; Sallis et al., 2009), disabled (Beard et al., 2009) and to report poorer overall health status (Bowling, Barber, Morris, & Ebrahim, 2006). Moreover, walking outside can become more cumbersome and challenging for older adults, as subtle age-related changes in physical functioning can influence the distance they can walk and their ability to negotiate obstacles.
The aging process may also influence way-finding, which Lawton (2010, p. 328) defined as “finding one’s way in three-dimensional environments,” and involves the tactical and strategic cognitive elements of navigation that guide one’s movements. Cornell, Sorenson, and Mio (2003) found that way-finding performance was positively related to perceived sense of direction. Way-finding performance is poor among individuals with dementia (Sheehan, Burton, & Mitchell, 2006), and has been linked to the hippocampus (Head & Isom, 2010), a brain region associated with structural and functional decline in aging populations (Driscoll et al., 2009; Raz et al., 2005). Physical activity interventions with older adults have been shown to increase hippocampal volume (Erickson et al., 2011) and thus may enhance actual way-finding abilities and in turn, their way-finding efficacy. Way-finding efficacy is the belief that one can successfully negotiate one’s environment. This capability is of particular relevance to older populations, as it may serve as an antecedent factor contributing to functional limitations. Although no research to our knowledge has examined way-finding efficacy, West, Welch, and Knabb (2002) found that self-efficacy for remembering directions to a store (which the authors referred to as “spatial self-efficacy”) was related to location memory recall. Way-finding efficacy is likely to be positively influenced by the extent to which older adults engage in outdoor physical activity, although we acknowledge the possibility that a reciprocal relationship among walking efficacy, way-finding efficacy, and walking behavior may also exist. Whether way-finding efficacy mediates the physical activity–functional performance–functional limitation relationship independent of the effects of walking efficacy remains to be determined.
Although the McAuley and colleagues (2006, 2007) model has contributed to our understanding of the physical activity and functional limitations relationship in older adults, its application has been limited, in large part, to relatively small urban samples of community-dwelling women. The objective of the present study was to provide a stronger test of this model in a large purposively diverse sample of older adults. To do so, we used data from the Healthy Aging Network Study, which represent a population of older adults who vary in demographics, health status, and the environments they encounter when engaged in neighborhood walking. Second, we were interested in examining the potentially independent role that the way-finding efficacy construct might play in physical activity’s relationship with functional performance and limitations. It was hypothesized that greater physical activity, as assessed by walking behavior, would be associated with higher levels of self-efficacy for walking and way-finding. In turn, having stronger self-efficacy would be associated with better functional performance and fewer functional limitations. Finally, it was hypothesized that better functional performance would be associated with fewer functional limitations.
METHOD
Participants and Procedure
The sample has been described in detail elsewhere by Prohaska and colleagues (2009) and Satariano and colleagues (2010). Briefly, participants were recruited from four U.S. locations; Alameda County, CA, Cook County, IL, Allegheny County, PA, and Durham/Wake Counties, NC. To be eligible, participants were required to be 65 years of age or older, live in one of the aforementioned regions for at least 12 months with no plans of moving, and have levels of cognitive functioning commensurate with completing an in-person interview. Further exclusionary criteria included having had surgery in the past 3 months; suffering from other chronic health conditions (e.g., chest pain) that might have limited unsupervised light physical activity. Participants were purposively sampled from a large geographic region to ensure diversity in self-ratings of health. Anyone who could not walk outdoors was excluded. A geographic information system (ArcGIS) was implemented to verify that recruitment from all four regions was diverse at ethnic, socioeconomic, and neighborhood levels. Trained interviewers conducted 1-hr in-person interviews with participants at their preferred location (i.e., either home or senior center). Study approval was obtained from the university institutional review board at each of the respective recruitment sites.
Measures
Demographic characteristics.—
Basic demographic information including age, gender, race/ethnicity, family income, education, marital status, and self-reported overall health were assessed in all participants.
Walking behavior.—
This measure was assessed by questions adapted from Michael, Green, and Farquhar (2006), whereby participants were asked to report the numbers of times that they spent brisk walking per week and the typical minutes they spent walking per session.
Self-efficacy.—
Two measures of self-efficacy were used in the current study, way-finding self-efficacy and self-efficacy for walking (Prohaska et al., 2009). The way-finding measure was adapted from self-efficacy items previously used in wellness assessments at one of the collaborating institutions. It also parallels similar measures of related constructs, including “perceived sense of direction” (Cornell et al., 2003) and “spatial self-efficacy” (West et al., 2002). The way-finding efficacy construct was assessed by two items reflecting participants’ confidence in their capability to (a) find their way on foot to places they want to go in their neighborhood and (b) to find their way on foot if they encountered detours or obstacles. Responses were given in an ordered response format (“Completely confident,” “Confident,” and “Not at all confident”). Walking self-efficacy was assessed as participants’ confidence for walking sequentially longer distances in terms of city blocks with three questions reflecting distances of ½ block, four blocks, and 10 blocks. These items were rated on a 10-point Likert scale (1 = not at all confident, 10 = absolutely confident). Cronbach’s alphas for way-finding and walking self-efficacy were .78 and .84, respectively.
Functional performance.—
Given our interest in walking as the physical activity behavior of interest, functional performance was restricted to the assessment of lower extremity functioning. To this end, we used a modified version of the Short Physical Performance Battery (SPPB; Guralnik, Ferrucci, Simonsick, Salive, & Wallace, 1995; Guralnik et al., 1994). Walking speed (i.e., feet per second) was assessed by a timed 60-s walk (rather than an 8-foot walk), and a one-legged stand (i.e., time that participants were able to remain balanced on one leg, up to 10 s) was included and used here due to lack of variability in full tandem stand (76% of sample could hold the stand for the full 10 s), the most challenging balance component of the standard SPPB tests. A chair stand assessment (i.e., time taken for participants to stand up five times within 60 s) was also conducted, and time was reverse coded; thus, higher scores for all performance variables indicated better performance.
Functional limitations.—
To assess perceived functional limitations, a series of items adapted from the Study of Physical Performance and Age Related Changes in Sonomans project (see Tager, Swanson, & Satariano, 1998) and from measures by Nagi (1976) and Rosow and Breslau (1966) were used. Initial confirmatory factor analytic procedures resulted in four items representing a single index of lower functional limitations (“Stooping, crouching, or kneeling,” “Getting up from a stooping, crouching, or kneeling position,” “Getting up or down a flight of stairs,” and “Standing up after sitting in a chair”). Items were scored on a 4-point Likert scale (i.e., 0 = None, 3 = A lot). This measure was used in all subsequent analyses. Participants were also asked to indicate whether they were unable to do these activities or if they were cautioned against doing these activities by their physician. Affirmative responses to these latter questions were subsequently coded as having maximal limitations for the respective item. Internal consistency for this measure was good, α = .82.
Analytical Strategy
Structural equation models were estimated with the Mplus 6.0 (Muthén & Muthén, 1998–2011) software program using the maximum likelihood estimator with robust standard errors. We validated the hypothesized model using conventional structural equation modeling practices; that is, we first evaluated a 5-factor measurement model followed by a structural model with direct and indirect effects. We subsequently tested this model when controlling for demographic factors. Additionally, invariance testing was also conducted to evaluate potential differences between recruitment sites which may have been influenced by socioenvironmental factors. Specifically, equality constraints were successively added for model parameters between more rural (i.e., Durham/Wake counties) and more urban groups (i.e., Alameda, Allegheny, and Cook counties). We first tested the equivalence of the factor structure itself (i.e., configural invariance), followed by the equivalence of the factor loadings (i.e., metric invariance), intercepts (scalar invariance), and residual variances (strict invariance).
Multiple indices were used for evaluating overall and relative fit of the theoretical model to the observed data. Specifically, for the traditional structural equation models, the chi-square (χ2) goodness-of-fit test was used to assess global fit of the model, whereby χ2 with p values ≥ .05 indicate a good overall model fit. Additionally, because the χ2 value is sensitive to sample size, we used two additional criteria recommended by Hu and Bentler (1999) to estimate goodness of model fit: the Comparative Fit Index (CFI), Tucker-Lewis Index (TLI), and Root Mean Square Error of Approximation (RMSEA) with values ≥0.95, ≥0.95, and ≤0.06, respectively, being indicative of good model fit. Evidence of invariance of parameters between nested models was based on nonsignificant chi-square difference tests, corrected for nonnormality (Satorra & Bentler, 2001). Note that changes in χ2 are associated with the same problems χ2 has as a global fit index. Therefore, we also relied on additional recommendations, including incremental change in CFI < 0.01 (G. W. Cheung & Rensvold, 2002), TLI < 0.01 (Marsh, Hau, & Grayson, 2005), and RMSEA < 0.015 (Chen, 2007).
RESULTS
Demographics
Our sample was composed of 884 community-dwelling older adults between the ages of 65 and 88 (M = 74.8) who were primarily White (65%), female (77%), had attended some college (54.8%), were not married (61.4%), and reported being in good health or better (78%; 22% self-reported their health to be fair). Descriptive statistics for all other model variables are shown in Table 1.
Table 1.
Descriptive Statistics for Main Study Variables
| Variable | Sample range | Means (n) | SDs |
| Walking (min)a | 0–2,310.00 | 167.80 (874) | 235.87 |
| Walk sessions per week | 0–70.00 | 3.61 (882) | 4.89 |
| Way-finding efficacyb | 0–4.00 | 3.35 (871) | 1.00 |
| Walking efficacyb | 3.00–30.00 | 24.44 (882) | 7.12 |
| Chair stand time (s) | 5.03–45.44 | 13.33 (796) | 5.39 |
| Walking speed (ft/s) | 0–6.85 | 2.75 (864) | .92 |
| One-leg stand (s) | 0.66–50.00 | 7.91 (606) | 3.55 |
| Perceived functional limitationsb | 0–15.00 | 3.42 (850) | 3.37 |
Notes. aValues are based on raw data.
Total scores.
Measurement Model
The initial correlated latent-factor measurement model provided an adequate fit to the data (χ² = 199.851 (67), p < .001, RMSEA = 0.047, 90% confidence interval [CI] = 0.040–0.055, CFI = 0.960, TLI = 0.946). Although the χ² goodness-of-fit test was significant, it is sensitive to sample size and the combination of other fit indices suggested an adequate model-to-data fit (Hu & Bentler, 1999). For identification purposes, two items representing self-efficacy for walking the two longest distances (i.e., four blocks and 10 blocks) were allowed to correlate and way-finding efficacy residual variances were set equal to each other. Further item content review suggested considerable overlap among two of the functional limitation items. These items contained the phrase “stooping, crouching, or kneeling” and modification indices indicated that there was a strong likelihood of common measurement error across these items. Therefore, the model was rerun with the residuals of these two variables allowed to correlate, thereby accounting for the shared variance. This resulted in a significantly better fitting model (χ² = 77.513 (65), p = .138, RMSEA = 0.015, 90% CI = 0.000–0.026, CFI = 0.996, TLI = 0.995). This was the final measurement model used in all subsequent analyses.
Correlations Among Latent Constructs
Table 2 shows the correlations among all of the latent variables. As expected, based on predictions of the hypothesized model, greater physical activity was significantly associated with higher levels of self-efficacy, better functional performance, and fewer functional limitations. More efficacious participants in turn demonstrated better functional performance and reported fewer functional limitations. Finally, better functional performance was strongly associated with fewer lower body functional limitations.
Table 2.
Correlations Among Latent Factor Means Scores
| Factor names | 1 | 2 | 3 | 4 | 5 |
| 1. Walking behavior | — | ||||
| 2. Wayfinding self-efficacy | .09 | — | |||
| 3. Walking self-efficacy | .26 | .24 | — | ||
| 4. Lower-body functional performance | .24 | .20 | .45 | — | |
| 5. Lower-body functional limitations | −.18 | −.17 | −.51 | −.42 | — |
Note. All correlations are significant at p < .001.
Structural Model
The next stage of analysis was to add the hypothesized direct and indirect effects (see Figure 1) to the measurement model. The overall fit of the model was relatively unchanged (χ² = 71.933 (64), p = .232, RMSEA = 0.012, 90% CI = 0.000–0.024, CFI = 0.998, TLI = 0.997), and all hypothesized direct paths were significant (see Figure 1 for standardized path estimates). As can be seen, the relationships between walking behavior and lower extremity functional limitations was rendered nonsignificant when the self-efficacy variables were treated as mediating variables. As hypothesized, walking more frequently and longer was associated with stronger way-finding and walking self-efficacy. Walking and way-finding self-efficacy was in turn associated with better functional performance, and better functional performance was associated with fewer functional limitations. Additionally, there were significant direct effects of walking self-efficacy, but not way-finding self-efficacy, on functional limitations. Finally, as hypothesized, the overall indirect effects from walking behavior to functional limitations via walking self-efficacy (−0.13), via functional performance (−0.08), and via walking self-efficacy and functional performance (−0.09) were all significant (p < .01). The hypothesized model accounted for 50% of the variance in lower extremity functional limitations.
Figure 1.
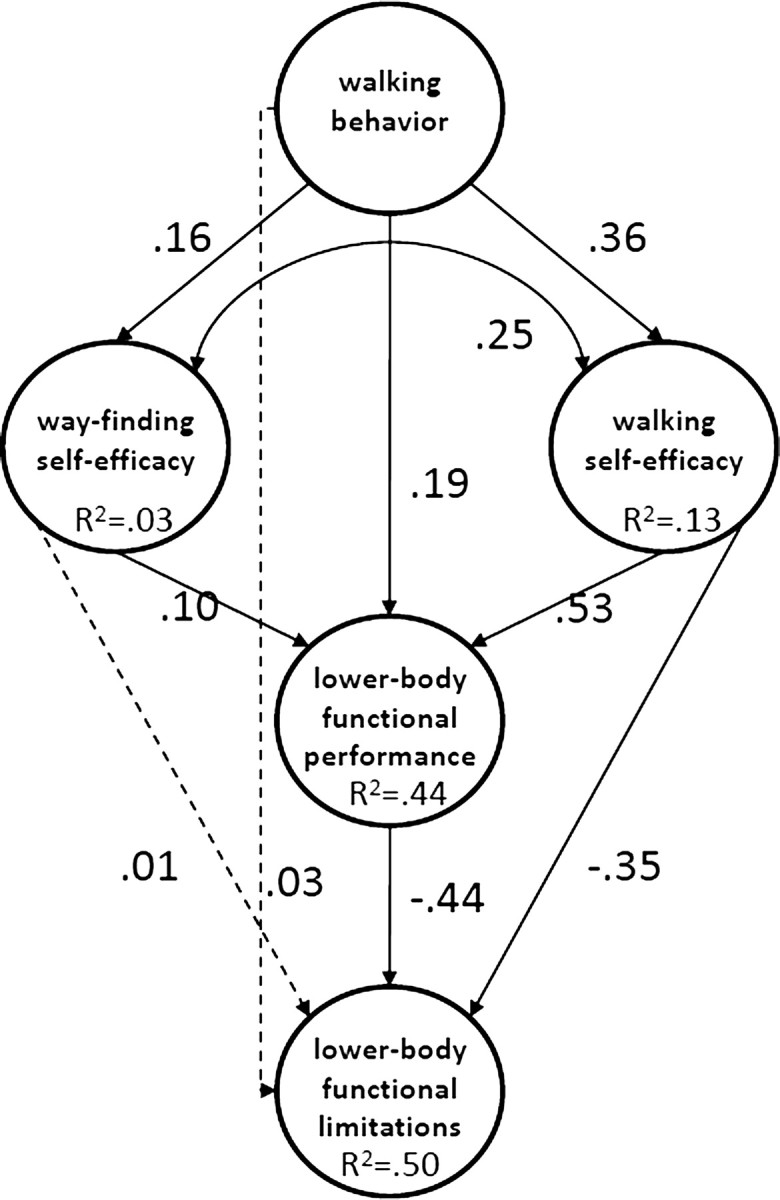
Path diagram of functional limitations. Solid lines represent significant direct effects, whereas dotted lines represent nonsignificant relationships. Standardized coefficients are reported for ease of interpretation.
Effects of Demographic Characteristics on Hypothesized Model
In the next series of analyses, we reran our hypothesized model saturating it for sex (0 = female; 1 = male), marital status (0 = not married; 1 = married), age, and education. This model continued to fit the data well (χ² = 170.307 (101), p < .001, RMSEA = 0.028, 90% CI = 0.021–0.035, CFI = 0.982, TLI = 0.974). None of hypothesized paths previously tested were significantly altered in terms of strength or direction of the path loading. However, there were a number of interesting significant (p < .05) relationships among the demographic characteristics and model constructs. For example, male participants (β = .20) and more educated participants (β = .17) reported higher levels of walking behavior. Younger participants (β = −.17) and those who were male (β = .13), more educated (β = .13), and married (β = .06) reported higher levels of way-finding efficacy, whereas higher levels of walking efficacy were associated with being younger (β = −.17), having more education (β = .11) and being married (β = .13). Older (β = −.19), female (β = −.07), and unmarried (β = −.15) participants had poorer functional performance. Finally, as might be expected, older adults (β = .10) reported more functional limitations than their younger counterparts.
Invariance Across Groups That Differ by Geographic Location
To determine if our best-fitting measurement model could be generalized across older adults from qualitatively different regions of the country, we next tested group invariance across rural and urban locations. The configural invariance model (i.e., identical factor structure across groups, while factors, item loadings, intercepts, and residual variances were allowed to vary) fit the data well (χ2 = 188.202 (131), p = .001, RMSEA = 0.031, 95% CI = 0.021–0.041, CFI = 0.986, TLI = 0.980). The metric invariance model, with the addition of identical factor loadings across groups, also provided an excellent fit to the data (χ2 = 218.768 (144), p < .001, RMSEA = 0.034, 95% CI = 0.025–0.043, CFI = 0.981, TLI = 0.976). The adjusted Satorra–Bentler (S–B) χ2 Δ test (Satorra & Bentler, 2001) was significant (p = .02), but change in CFI, TLI, and RMSEA change did not exceed recommendations; thus, we conclude that the additional restrictions did not substantively change the model fit and that the model meets the minimal requirements for invariance (Horn & McArdle, 1992). Next, the item intercepts were constrained across groups and this scalar invariance model provided a relatively good fit (χ2 = 275.251 (158), p < .001, RMSEA = 0.041, 95% CI = 0.033–0.049, CFI = 0.970, TLI = 0.966). The S–B χ2 Δ test was significant again, but incremental change in CFI, TLI, and RMSEA did not point to any substantive differences. Finally, when residual variances and correlated uniquenesses were constrained across groups, this model also fit the data (χ2 = 326.859 (174), p = < .001, RMSEA = 0.045, 95% CI = 0.037–0.052, CFI = 0.961, TLI = 0.960). Again, S–B χ2 Δ test was significantly different (p = .002), but minute changes in CFI, TLI, and RMSEA suggest that χ2 Δ may be trivial. Together, these results suggest that there were no substantive differences in the theoretical model between geographical grouping.
DISCUSSION
The purpose of this study was to evaluate, in a large geographically diverse sample of older adults, the roles played by self-efficacy and functional performance in the physical activity and functional limitations relationship. Our findings provide validation evidence for the model proposed and tested by McAuley and colleagues (2006, 2007). Specifically, walking more frequently and for longer duration was positively associated with beliefs in capabilities to finding one’s way in compromised environments and walking incrementally further distances. Walking-related self-efficacy was, in turn, positively associated with having better lower extremity function and fewer lower body function limitations. Having better functional performance was also associated with reporting fewer functional limitations. Furthermore, through a series of group invariance analyses, we established that the model is not different for people who reside in more rural versus more urban areas.
Keysor (2003) has previously noted that the protective effect of physical activity on self-reported functional limitations is relatively consistent. However, this association is typically reported only at the bivariate level. More recent evidence suggests that this relationship is completely mediated by such constructs as efficacy for physical capabilities and actual ability to perform functional tasks tested. McAuley and his colleagues have previously reported such findings both at baseline and longitudinally in a sample of community-dwelling older women. The present data offer support for the robustness of this general pattern of relationships in a number of ways.
First, we employed entirely different measures to assess each of the theorized model constructs. Such a practice is permitted within a latent variable framework, given that there could be limitless numbers of measures which reflect any one of the constructs within the model. For example, as well as assessing walking self-efficacy, which one would expect to be associated with physical activity as a proximal outcome, we also assessed a new construct; way-finding efficacy. Given the increasing interest in the effects of the built environment on health behaviors (Bowling et al., 2006) and the potential for difficulties in negotiating such environments as we age, we reasoned that the construct of way-finding efficacy could have important implications for abilities to carry out physical function activities. Indeed, in our structural model, way-finding efficacy was influenced by walking behavior and was associated with better functional performance.
Although way-finding efficacy relationships were significant, they were quite modest. It is not entirely surprising that way-finding efficacy had a significant positive effect on functional performance, as this cognitive skill is positively associated with spatial abilities. Thus, more favorable way-finding beliefs may transfer to positive beliefs about proprioception, heightened awareness of task demands associated with novel physical performance tasks, and in turn, affect chair standing, single-leg balance, and gait performance. However, way-finding efficacy had no direct effect on self-reported functional limitations. These associations contrasted markedly with walking efficacy, which was moderately to strongly associated with all model constructs. Walking self-efficacy may overlap more strongly with functional performance and functional limitations because it assesses a more relevant task-specific confidence.
Given the modest role played by way-finding efficacy in the present study, subsequent tests of this model may do well to incorporate a more refined measure of efficacy to negotiate the built environment, which could include confidence in capabilities to be physically active relative to neighborhood safety, connectivity, and aesthetics (Saelens, Sallis, Black, & Chen, 2003). It is certainly possible that way-finding is one of many aspects already considered in overall walking efficacy judgments by older adults. For example, assessments of efficacy for balance (Nagi, 1976) and preventing falls (Tinetti, De Leon, Doucette, & Baker, 1994) have been previously developed, and way-finding efficacy could be viewed similarly, as an aspect of confidence in one’s walking coordination abilities. However, we feel that way-finding efficacy is a separate construct altogether, and it should be viewed as confidence in a cognitive ability. Further exploration into the factor structure of this construct and whether walking efficacy should be conceptualized hierarchically would add greater breadth and complexity to our understanding of walking-related self-efficacy.
Additionally, we provide further support for the suggestion of Stewart (2003) and Guralnik and Ferrucci (2003) that objective physical performance measures and self-reported functional limitations are not necessarily isomorphic constructs. For example, the latent variables reflecting these constructs showed only a moderately strong positive relationship (r = −.42). Moreover, it would appear that physical function performance may be an important prior step to functional limitations in the disablement process (Stewart, 2003). We note also that our measure of lower extremity functional performance contained items reflecting gait speed, balance, and strength, all important factors in preventing age-related decline in mobility disability. For example, Rantanen and colleagues (2001) using data from the Women’s Health and Aging Study examined the cumulative effect of coimpairments on walking disability in older women. They reported a five times greater relative risk of severe walking disability for women with the poorest balance and strength. That the effects of physical activity on this important predictor of dependence in older adults are indirect, through self-efficacy, rather than direct is an important finding. As McAuley and colleagues (2007) note, self-efficacy is a modifiable construct and therefore an important target for intervention (Brassington, Atienza, Perczek, DiLorenzo, & King, 2002; C. Cheung et al., 2007). Providing successful walking experiences involving the negotiation of barriers, obstacles, and difficulties is likely to enhance self-efficacy that, in turn, is likely to lead to improved lower extremity function and thereby preventing further onset of functional limitations.
There are a number of significant strengths to the present study. First, the sample size was approximately 3.5 times larger than the sample in which the hypothesized model was originally tested. Moreover, our sample was drawn from four distinct geographic areas reflecting good diversity and representativeness and included both men and women. In addition, few theoretical models have ever been tested for group invariance to examine the possibility that participants from different regions may interpret the meaning of constructs differently. Given that few substantive differences were found, our model appears to be fairly generalizable in this respect. Finally, the latent variable approach to examining the proposed model represents a strength, as does the adoption of the key factor in Bandura’s (1997) social cognitive theory, self-efficacy, as a central model component.
We further tested the veracity of the model by using a partial least squares (PLS) path modeling approach (details available from S. P. Mullen). PLS estimation has several advantages over covariance-based modeling, including minimizing residual variance, providing the best estimated weights for each latent variable, and maximizing the explained variance in each dependent variable. The results supported the direction of hypothesized relationships. However, we do acknowledge the limitations associated with our data. At the forefront of these is the cross-sectional design of the study which limits the interpretation of our findings and certainly precludes statements about causality. Experimental and longitudinal approaches should be used in future research, as they are the best ways to determine causal ordering. It is also quite possible that the direction of the relationships might evolve in the reverse order, which would be in line with the reciprocal deterministic tenets of social cognitive theory. For example, it is reasonable to expect that the emergence of functional limitations might lead to subsequent reductions in physical activity (e.g., Jerome et al., 2006). In a previous version of the model, McAuley and colleagues (2007) tested this proposition in the context of a longitudinal panel model and reported only one cross-lagged effect from baseline functional limitations to changes in self-efficacy at 24 months. A more definitive test of this model and the relationships among its components could be tested within the context of targeted randomized controlled trials. For example, interventionists could aim to enhance self-efficacy beliefs by providing multiple sources of efficacy information in the form of maps to safe walking routes and assisting in the formation of walking groups. Changes in efficacy could then be tracked in parallel with changes in subsequent physical activity, functional performance and limitations. Alternatively, by changing the built indoor (e.g., lowering cabinets, removing clutter) or outdoor environment (e.g., improving the landscaping, increasing the visibility of signs and key landmarks), functional performance or functional limitations could be the focus of an intervention and model constructs could be subsequently tested for change. One should also note that our way-finding efficacy measure could be improved upon to capture more variability, by adding more items or increasing the range of responses. Finally, our sample was well-educated and relatively healthy and the results may not generalize to less-educated older adults, or to those with severe disabilities.
In conclusion, we provide further evidence for the veracity of a self-efficacy–based model of the relationship between physical activity and functional limitations. Hypothesized model relationships were supported when controlling for education, marital status, age, and gender. Whether it is possible to reduce or delay the onset of functional limitations in older adults through the implementation of efficacy-enhancing strategies is an intriguing question that awaits an answer.
FUNDING
The HAN Walking Study was also made possible through work conducted by the CDC Healthy Aging Research Network. The CDC Healthy Aging Research Network is a Prevention Research Centers Program funded by the CDC Healthy Aging Program. This research was supported in part by cooperative agreements from CDC’s Prevention Research Centers Program: U-48-DP-001911, 001908, 001921, 001924, 001936, 001938, and 001944. The contents of this manuscript are solely the responsibility of the authors and do not necessarily represent the official views of the CDC.
The project also used data from the RAND Center for Population Health and Health Disparities (CPHHD), which is funded by Grant 1-P50-ES012383 from the National Institute of Environmental Health Sciences. For further information on CPHHD, see www.rand.org/health/centers/pophealth/index.html.
Edward McAuley is supported by a Shahid and Ann Carlson Khan Professorship in Applied Health Sciences.
Acknowledgments
The HAN Walking Study was made possible through a grant from the Robert Wood Johnson Foundation, Active Living Research Program (052515). The main participants on that grant include the following: William Satariano and Susan Ivey (Principal and Co-Principal Investigators/Site Directors, UC Berkeley, Alameda County, CA); Elaine Kurtovich (Project Manager, UC Berkeley); Melissa Kealey (Data Manager, UC Berkeley); Constance Bayles (Site Director, University of Pittsburgh, Allegheny County, PA); Rebecca Hunter (Site Director, University of North Carolina, Wake and Durham counties, NC); and Thomas Prohaska (Site Director, University of Illinois, Chicago, Cook County, IL). S. P. Mullen was involved in the data analysis and manuscript preparation. E. McAuley was involved in supervising the data analysis and manuscript preparation. W. A. Satariano was involved in study planning and revising the manuscript. M. Kealey was involved in data preparation and manuscript revising. T. R. Prohaska was involved in study planning and manuscript revising.
References
- Bandura A. Social foundations of thought and action. Englewood Cliffs, NJ: Prentice-Hall; 1986. [Google Scholar]
- Bandura A. Self-efficacy: The exercise of control. New York: W. H. Freeman; 1997. [Google Scholar]
- Beard J, Blaney S, Cerda M, Frye V, Lovasi G, Ompad D, Vlahov D. Neighborhood characteristics and disability in older adults. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2009;64:252–257. doi: 10.1093/geronb/gbn018. doi:10.1093/geronb/gbn018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Booth K, Pinkston M, Poston W. Obesity and the built environment. Journal of the American Dietetic Association. 2005;105:110–117. doi: 10.1016/j.jada.2005.02.045. doi:10.1016/j.jada.2005.02.045. [DOI] [PubMed] [Google Scholar]
- Bowling A, Barber J, Morris R, Ebrahim S. Do perceptions of neighbourhood environment influence health? Baseline findings from a British survey of aging. Journal of Epidemiology and Community health. 2006;60:476–483. doi: 10.1136/jech.2005.039032. doi:10.1136/jech.2005.039032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brassington GS, Atienza AA, Perczek RE, DiLorenzo TM, King AC. Intervention-related cognitive versus social mediators of exercise adherence in the elderly. American Journal of Preventive Medicine. 2002;23:80–86. doi: 10.1016/s0749-3797(02)00477-4. [DOI] [PubMed] [Google Scholar]
- Chen FF. Sensitivity of goodness of fit indexes to lack of measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal. 2007;14:464–504. doi:10.1080/10705510701301834. [Google Scholar]
- Cheung C, Wyman J, Gross C, Peters J, Findorff M, Stock H. Exercise behavior in older adults: A test of the transtheoretical model. Journal of Aging and Physical Activity. 2007;15:103–118. doi: 10.1123/japa.15.1.103. [DOI] [PubMed] [Google Scholar]
- Cheung GW, Rensvold RB. Evaluating goodness-of-fit indexes for testing measurement invariance. Structural Equation Modeling: A Multidisciplinary Journal. 2002;9:233–255. doi:10.1207/S15328007SEM0902_5. [Google Scholar]
- Cornell EH, Sorenson A, Mio T. Human sense of direction and wayfinding. Annals of the Association of American Geographers. 2003;93:399–425. doi:10.1111/1467-8306.9302009. [Google Scholar]
- Driscoll I, Davatzikos C, An Y, Wu X, Shen D, Kraut M, Resnick S. Longitudinal pattern of regional brain volume change differentiates normal aging from MCI. Neurology. 2009;72:1906–1913. doi: 10.1212/WNL.0b013e3181a82634. doi:10.1212/WNL.0b013e3181a82634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Erickson KI, Voss MW, Prakash RS, Basak C, Szabo A, Chaddock L, White SM. Exercise training increases size of hippocampus and improves memory. Proceedings of the National Academy of Sciences of the United States of America. 2011;108:3017–3022. doi: 10.1073/pnas.1015950108. doi:10.1073/pnas.1015950108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guralnik J, Ferrucci L. Assessing the building blocks of function: Utilizing measures of functional limitation. American Journal of Preventive Medicine. 2003;25:112–121. doi: 10.1016/s0749-3797(03)00174-0. doi:10.1016/S0749-3797(03)00174-0. [DOI] [PubMed] [Google Scholar]
- Guralnik J, Ferrucci L, Simonsick E, Salive M, Wallace R. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. New England Journal of Medicine. 1995;332:556–562. doi: 10.1056/NEJM199503023320902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Guralnik J, Simonsick E, Ferrucci L, Glynn R, Berkman L, Blazer D, Wallace R. A short physical performance battery assessing lower extremity function: Association with self-reported disability and prediction of mortality and nursing home admission. Journal of Gerontology. 1994;49:M85–M94. doi: 10.1093/geronj/49.2.m85. [DOI] [PubMed] [Google Scholar]
- Head D, Isom M. Age effects on wayfinding and route learning skills. Behavioural Brain Research. 2010;209:49–58. doi: 10.1016/j.bbr.2010.01.012. doi:10.1016/j.bbr.2010.01.012. [DOI] [PubMed] [Google Scholar]
- Horn JL, McArdle JJ. A practical and theoretical guide to measurement invariance in aging research. Experimental Aging Research. 1992;18:117–144. doi: 10.1080/03610739208253916. [DOI] [PubMed] [Google Scholar]
- Hu L, Bentler P. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal. 1999;6:1–55. doi:10.1080/10705519909540118. [Google Scholar]
- Huang WNW, Perera S, VanSwearingen J, Studenski S. Performance measures predict onset of activity of daily living difficulty in community-dwelling older adults. Journal of the American Geriatrics Society. 2010;58:844–852. doi: 10.1111/j.1532-5415.2010.02820.x. doi:10.1111/j.1532-5415.2010.02820.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jerome GJ, Glass TA, Mielke M, Xue QL, Andersen RE, Fried LP. Physical activity participation by presence and type of functional deficits in older women: The Women's Health and Aging Studies. The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences. 2006;61:1171. doi: 10.1093/gerona/61.11.1171. [DOI] [PubMed] [Google Scholar]
- Keysor J. Does late-life physical activity or exercise prevent or minimize disablement? A critical review of the scientific evidence. American Journal of Preventive Medicine. 2003;25:129–136. doi: 10.1016/s0749-3797(03)00176-4. doi:10.1016/S0749-3797(03)00176-4. [DOI] [PubMed] [Google Scholar]
- Lawton CA. Gender, spatial abilities, and wayfinding. In: Chrisler JC, McCreary DR, editors. Handbook of gender research in psychology. New York: Springer; 2010. pp. 317–341. [Google Scholar]
- Marsh HW, Hau KT, Grayson D. Goodness of fit in structural equation models. In: Maydeu-Olivares A, McArdle J, editors. Psychometrics. A Festschrift to Roderick P McDonald. Hillsdale, NJ: Erlbaum; 2005. [Google Scholar]
- McAuley E, Konopack JF, Morris KS, Motl RW, Hu L, Doerksen SE, Rosengren K. Physical activity and functional limitations in older women: Influence of self-efficacy. The Journals of Gerontology, Series B: Psychological Sciences and Social Sciences. 2006;61:270–277. doi: 10.1093/geronb/61.5.p270. [DOI] [PubMed] [Google Scholar]
- McAuley E, Morris KS, Doerksen SE, Motl RW, Liang H, White SM, Rosengren K. Effects of change in physical activity on physical function limitations in older women: Mediating roles of physical function performance and self-efficacy. Journal of the American Geriatrics Society. 2007;55:1967–1973. doi: 10.1111/j.1532-5415.2007.01469.x. doi:10.1111/j.1532-5415.2007.01469.x. [DOI] [PubMed] [Google Scholar]
- Michael Y, Green M, Farquhar S. Neighborhood design and active aging. Health & Place. 2006;12:734–740. doi: 10.1016/j.healthplace.2005.08.002. doi:10.1016/j.healthplace.2005.08.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén L, Muthén B. Mplus user’s guide. Los Angeles, CA: Author; 1998–2011. [Google Scholar]
- Nagi S. An epidemiology of disability among adults in the United States. The Milbank Memorial Fund Quarterly. Health and Society. 1976;54:439–467. [PubMed] [Google Scholar]
- Onder G, Penninx B, Ferrucci L, Fried L, Guralnik J, Pahor M. Measures of physical performance and risk for progressive and catastrophic disability: Results from the Women's Health and Aging Study. The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences. 2005;60:74–79. doi: 10.1093/gerona/60.1.74. [DOI] [PubMed] [Google Scholar]
- Owen N, Humpel N, Leslie E, Bauman A, Sallis J. Understanding environmental influences on walking: Review and research agenda. American Journal of Preventive Medicine. 2004;27:67–76. doi: 10.1016/j.amepre.2004.03.006. doi:10.1016/j.amepre.2004.03.006. [DOI] [PubMed] [Google Scholar]
- Paterson DH, Govindasamy D, Vidmar M, Cunningham D, Koval J. Longitudinal study of determinants of dependence in an elderly population. Journal of the American Geriatrics Society. 2004;52:1632–1638. doi: 10.1111/j.1532-5415.2004.52454.x. doi:10.1111/j.1532-5415.2004.52454.x. [DOI] [PubMed] [Google Scholar]
- Paterson DH, Warburton DER. Physical activity and functional limitations in older adults: A systematic review related to Canada's Physical Activity Guidelines. International Journal of Behavioral Nutrition and Physical Activity. 2010;7:38. doi: 10.1186/1479-5868-7-38. doi:10.1186/1479-5868-7-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poortinga W. Perceptions of the environment, physical activity, and obesity. Social Science & Medicine. 2006;63:2835–2846. doi: 10.1016/j.socscimed.2006.07.018. doi:10.1016/j.socscimed.2006.07.018. [DOI] [PubMed] [Google Scholar]
- Prohaska T, Eisenstein A, Satariano W, Hunter R, Bayles C, Kurtovich E, Ivey S. Walking and the preservation of cognitive function in older populations. The Gerontologist. 2009;49(Suppl. 1):S86–S93. doi: 10.1093/geront/gnp079. doi:10.1093/geront/gnp079. [DOI] [PubMed] [Google Scholar]
- Rantanen T, Guralnik J, Ferrucci L, Penninx B, Leveille S, Sipilä S, Fried L. Coimpairments as predictors of severe walking disability in older women. Journal of the American Geriatrics Society. 2001;49:21–27. doi: 10.1046/j.1532-5415.2001.49005.x. doi:10.1046/j.1532-5415.2001.49005.x. [DOI] [PubMed] [Google Scholar]
- Raz N, Lindenberger U, Rodrigue KM, Kennedy KM, Head D, Williamson A, Acker JD. Regional brain changes in aging healthy adults: General trends, individual differences and modifiers. Cerebral Cortex. 2005;15:1676–1689. doi: 10.1093/cercor/bhi044. doi:10.1093/cercor/bhi044. [DOI] [PubMed] [Google Scholar]
- Rejeski W, Mihalko S. Physical activity and quality of life in older adults. The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences. 2001;56(Suppl. 2):23–35. doi: 10.1093/gerona/56.suppl_2.23. doi:10.1093/gerona/56.suppl_2.23. [DOI] [PubMed] [Google Scholar]
- Rosow I, Breslau N. A Guttman health scale for the aged. Journal of Gerontology. 1966;21:556–559. doi: 10.1093/geronj/21.4.556. [DOI] [PubMed] [Google Scholar]
- Saelens B, Sallis J, Black J, Chen D. Neighborhood-based differences in physical activity: An environment scale evaluation. American Journal of Public Health. 2003;93:1552–1558. doi: 10.2105/ajph.93.9.1552. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sallis J, Saelens B, Frank L, Conway T, Slymen D, Cain K, Kerr J. Neighborhood built environment and income: Examining multiple health outcomes. Social Science & Medicine. 2009;68:1285–1293. doi: 10.1016/j.socscimed.2009.01.017. doi:10.1016/j.socscimed.2009.01.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Satariano W, Ivey S, Kurtovich E, Kealey M, Hubbard A, Bayles C, Prohaska T. Lower-body function, neighborhoods, and walking in an older population. American Journal of Preventive Medicine. 2010;38:419–428. doi: 10.1016/j.amepre.2009.12.031. doi:10.1016/j.amepre.2009.12.031. [DOI] [PubMed] [Google Scholar]
- Satorra A, Bentler PM. A scaled difference chi-square test statistic for moment structure analysis. Psychometrika. 2001;66:507–514. doi: 10.1007/s11336-009-9135-y. doi:10.1007/BF02296192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheehan B, Burton E, Mitchell L. Outdoor wayfinding in dementia. Dementia. 2006;5:271–281. doi:10.1177/1471301206062254. [Google Scholar]
- Stewart AL. Conceptual challenges in linking physical activity and disability research. American Journal of Preventive Medicine. 2003;25:137–140. doi: 10.1016/s0749-3797(03)00187-9. doi:10.1016/S0749-3797(03)00187-9. [DOI] [PubMed] [Google Scholar]
- Stuifbergen A, Blozis S, Harrison T, Becker H. Exercise, functional limitations, and quality of life: A longitudinal study of persons with multiple sclerosis. Archives of Physical Medicine and Rehabilitation. 2006;87:935–943. doi: 10.1016/j.apmr.2006.04.003. doi:10.1016/j.apmr.2006.04.003. [DOI] [PubMed] [Google Scholar]
- Tager I, Swanson A, Satariano W. Reliability of physical performance and self-reported functional measures in an older population. The Journals of Gerontology, Series A: Biological Sciences and Medical Sciences. 1998;53:295–300. doi: 10.1093/gerona/53a.4.m295. [DOI] [PubMed] [Google Scholar]
- Tinetti ME, De Leon CFM, Doucette JT, Baker DI. Fear of falling and fall-related efficacy in relationship to functioning among community-living elders. Journal of Gerontology. 1994;49:M140–M147. doi: 10.1093/geronj/49.3.m140. [DOI] [PubMed] [Google Scholar]
- Verbrugge L, Jette A. The disablement process. Social Science & Medicine. 1994;38:1–14. doi: 10.1016/0277-9536(94)90294-1. [DOI] [PubMed] [Google Scholar]
- West RL, Welch DC, Knabb PD. Gender and aging: Spatial self-efficacy and location recall. Basic and Applied Social Psychology. 2002;24:71–80. [Google Scholar]