

Abstract
Chondroid lipoma is a rare and unusual benign soft tissue lesion. Although there have been several reports of the imaging findings of chondroid lipoma, very few described the radiographic calcification or ossification in a chondroid lipoma. We present a case of chondroid lipoma with adipose tissue and ossified components on plain radiography and MRI images. Correlation of imaging findings and pathological examination is provided to confirm the diagnosis.
Keywords: Chondroid lipoma, soft tissue, radiography, magnetic resonance imaging
Implications for practice
Chondroid lipoma is a rare benign adipose tissue tumour containing mature fat and chondroid matrix.
Typical MRI appearances of chondroid lipoma, in addition to the calcification within the tumour shown on radiographic images are demonstrated in this case report.
A combination of MR imaging and radiography is needed to make the clinical diagnosis of chondroid lipoma.
Background
Chondroid lipoma is a rare benign adipose tissue tumour which has components of mature fat and a chondroid matrix, bearing a markedly close pathologic resemblance to myxoid liposarcoma and extraskeletal myxoid chondrosarcoma.1-5 Chondroid lipoma may arise from the superficial muscular fascia, skeletal muscle or subcutis, and the tumour is most frequently located in the proximal extremity and limb girdle. It is characterised by showing a non-aggressive behaviour that does not require radical treatment. Reports regarding its cytologic and radiological features are scarce.2 There have been very few reports describing radiographic calcification or ossification in a chondroid lipoma.6-8 In this case report, we describe the imaging and pathologic findings of a chondroid lipoma in the right thigh.
Case report
A 34-year-old female was admitted to the outpatient department due to an increasing lump on the right thigh, which she stated as having been present for five years. Painful feeling sometimes occurred to the right upper leg. There was no complaint of lower limb weakness. There was no history of trauma and the patient was otherwise in good health. On physical examination, a deep-seated round mass was detected and located on the right thigh with a size of 25 x 25 x 15 cm, showing hard consistency and non-mobile feature (Figure 1).
Figure 1. Clinical photograph showing a huge lump in the anterior part of the right thigh.

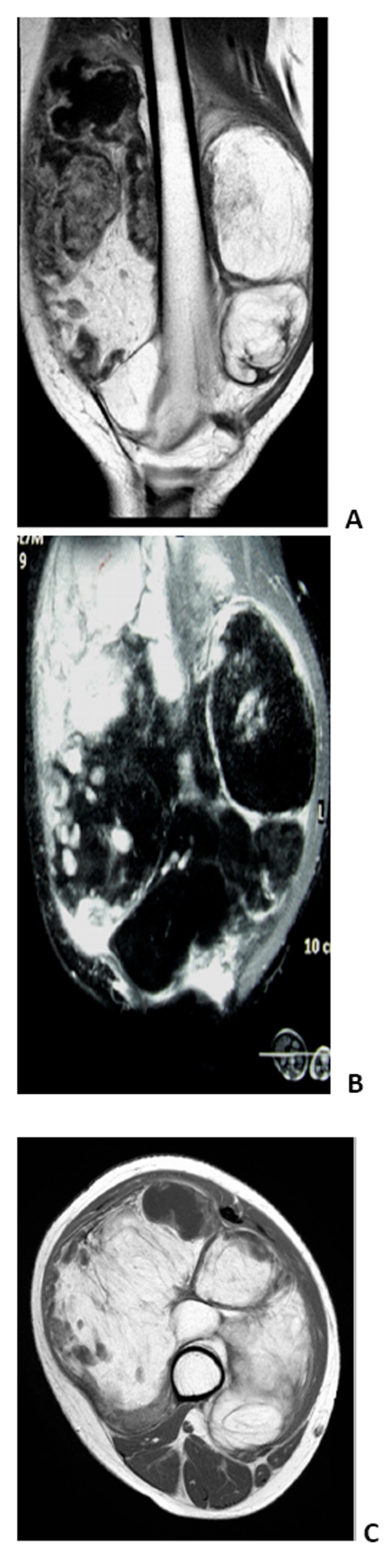
Radiographs showed a bulge soft tissue mass in the right lower thigh having predominantly radiolucent density with multiple chondroid matrix of calcification (Figure 2), but the bone cortex is still intact. A MRI was obtained to further define the extent and nature of the lesion, confirming heterogeneous soft tissue mass in the anterior compartment of the muscle of the right lower thigh which mostly consisted of fat tissue, thick septation and some nodular non-adipose components (Figure 3). T2-weighted images through the tumour demonstrated high signal intensity comparable with the signal intensity of fat (Figure 3A). Fat-suppressed T2-weighted images through the distal part of the tumour showed suppression of the signal through the central fatty components and lobular high signal intensity component at the peripheral rim (Figure 3B). After intravenous administration of gadolinium, the heterogeneous mass showed peripheral enhancement (Figure 3C). According to these MRI findings, diagnosis of liposarcoma was initially suggested. Because the presence of chondroid calcification which was shown on radiographs, and these nodular non-adipose components tend to be chondroid matrix, the diagnosis of chondroid lipoma was recommended.
Figure 2. Radiographs revealed a bulged soft tissue mass in anterior compartment of right lower thigh showing predominantly radiolucent density with multiple chondroid matrix of calcification. Bone structure is still intact.
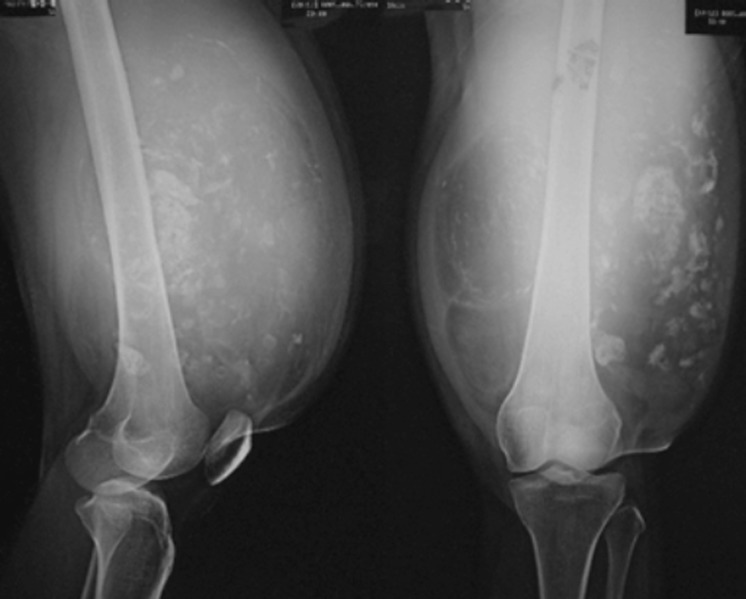
Figure 3. Sagital T2-weighted (3A), coronal, Fat-suppressed T2-weighted (3B) and axial T1-weighted with gadolinium enhanced MR images (3C) demonstrated heterogeneous soft tissue mass with mostly consisting of lipomatous components centrally and low-attenuation chondroid areas peripherally, with thick septa and show peripheral enhancement.
Fine needle aspiration biopsy was then performed. The smear from the biopsy showed chondroid material with sparse spindle cells with mild nuclear atypia. Cytology diagnosis was suggesting for malignancy. Based on clinical, radiological and cytological findings, the patient underwent extensive surgical excision of the tumour.
Pathological examination revealed that macroscopically the tumour was solid, composed of yellow material, which mostly consisted of fat tissue but in the periphery there were some foci of white solid area of cartilage tissue (Figure 4). Microscopically the tumour was composed of mature adipose tissue admixed with well formed lobules of hyaline cartilage (Figure 5). Based on the microscopic findings, a diagnosis of chondroid lipoma was established. Due to its rarity, the slides were sent to the University of California, Los Angeles for a second opinion, and the diagnosis of chondroid lipoma was confirmed. The patient had a good recovery after surgery, and did not develop any post- operative complications.
Figure 4. Gross specimen photograph during operation showed that a multilobulated mass was totally resected (4A), and axially sectioned gross specimen revealed a predominantly lipomatous component with multiple lobules of chondroid tissue and thick septation caudally (4B).

Figure 5. Under microscopic examination, the tumour was composed of mature adipose tissue admixed with well formed lobules of hyaline cartilage. Histopathologic examination with HE (Hematoxylin Eosin) staining low power view H&E 100 showed vacuolated cells (black arrows) embedded in chondroid/cartiliginous like matrix (red arrows), admixed with mature adipocytes/fat cells (blue arrows) (5A). Histopathologic examination with HE staining high power view H&E 400 showed vacuolated cytoplasm with central nuclei (black arrows) deposited in a chondroid/cartiliginous like matrix (red arrows), associated with mature adipocytes/fat cells (blue arrows) (5B).

Discussion
Chondroid lipoma is a rare, benign, lipomatous soft tissue tumour that manifests as a painless lump. Tumours are located most frequently in the proximal extremity and limb girdle, then in decreasing frequency in the leg, trunk, head and neck region, foot, and hand.4,9 Tumour depth was predominantly in the deep subcutis or skeletal muscle. The median tumour size was 4cm, and usually occurs predominantly in middle-aged adults. Women are more commonly affected than men. An accurate diagnosis is essential in guiding the treatment plan; however, imaging and histologic examination are not always conclusive, and reliance may be placed on immunohistochemical features.1- 6
There are few reports of imaging studies of chondroid lipoma. Reports of chondroid lipoma with evidence of radiographic calcification are very limited.7,8 In this case, a large tumour was found in the right thigh with presence of calcification, as shown in the radiographic images. The curvilinear calcification within the soft tissue mass raised a differential diagnosis of an extraskeletal chondroma or chondrosarcoma, a lipomatous lesion together with fat necrosis, or even synovial sarcoma. MRI features of chondroid lipoma help to make the diagnosis, although MRI appearances of6 chondriod lipoma were only reported in a very few studies. 1,6-8,10
MRI images demonstrate the typical fatty components based on signal intensity. Chondroid lipoma reflects the large fat and chondroid consistency of the tumour. These lesions often reveal high signal of fat peripherally, but contain nodular foci representing cartilage matrix of low signal intensity relative to muscle on T1 and T2 weighted MRI images. High signal intensity indicative of fat observed on T1- or T2-weighted MRI images is suppressed on Fat - supressed or short time-to-inverse inversion-recovery weighted (STIR) images, as is noticed in this case. These MRI findings are similar to the previous cases of chondroid lipoma with intralesional calcification. 6,7
At gross pathological examination, chondroid lipoma is an encapsulated, often multilobular, yellow to white mass with a size range of 1–11 cm. Chondroid lipomas are characterised by the presence of cells resembling chondroblasts and lipoblast mature adipose tissue, and myxoid matrix. These features may closely resemble myxoid liposarcoma or extraskeletal myxoid chondrosarcoma and thus lead to a pseudosarcomatous misdiagnosis. Immunohistochemically, tumour cells are consistently positive for vimentine and S100 protein. Positivity for CD68 and cytokeratins also has been observed.2,4
Unlike other malignant tumours such as chondrosarcoma which require the consideration of radical surgery and postoperative radiotherapy, chondroid lipoma is considered to be treated successfully with local excision. No recurrences, metastasis, or lead to malignant transformation have been observed. 6,7
In conclusion, we report a case of chondroid lipoma of the right thigh, a rare benign adipose tissue tumour containing mature fat and chondroid matrix. The correlation between radiological features as well as clinical presentation and the cytohistomorphology of this case plays an important role in making accurate diagnosis and guiding the treatment plan. In particular, we demonstrate the typical MRI appearances of chondroid lipoma, in addition to the calcification within the tumour shown on radiographic images. A combination of MR imaging and radiography is needed to make the clinical diagnosis of chondroid lipoma.
Footnotes
PEER REVIEW
Not commissioned. Externally peer reviewed.
CONFLICTS OF INTEREST
The authors declare that they have no competing interests.
FUNDING
Not applicable.
PATIENT CONSENT
- They have obtained written, informed consent for the publication of the details relating to the patient(s) in this report.
- All possible steps have been taken to safeguard the identity of the patient(s).
- This submission is compliant with the requirements of local research ethics committees.
Please cite this paper as: Setiawati R, Dimpudus FJ, Sun Z, Chondroid lipoma of the right thigh: Correlation of imaging findings and histopathology of an unusual benign lesion. AMJ 2012, 5, 7, 355-358. http//dx.doi.org/10.4066/AMJ.2012.1260.
References
- 1.Boets A, Van Mieghem IM, Sciot R, Breuseghem IV. Chondroid lipoma of the trunk: MRI appearance and pathologic correlation. Skeletal Radiol. 2004;33:666–669. doi: 10.1007/s00256-004-0774-x. [DOI] [PubMed] [Google Scholar]
- 2.Yang YJ, Damron TA, Ambrose JL. Diagnosis of chondroid lipoma by fine-needle aspiration biopsy. Arch Pathol Lab Med. 2001;125:1224–1226. doi: 10.5858/2001-125-1224-DOCLBF. [DOI] [PubMed] [Google Scholar]
- 3.Murphey MD, Carroll JF, Flemming DJ, Pope TL, Gannon FH, Kransdorf MJ. Benign musculoskeletal lipomatous lesions. Radiographics. 2004;24:1433–1466. doi: 10.1148/rg.245045120. [DOI] [PubMed] [Google Scholar]
- 4.Vasili C, Kligman M, Kirsh G. Incidental finding of chondroid lipoma at total hip arhtroplasty. J South Orthop Assoc. 2000;9(3):219–221. [PubMed] [Google Scholar]
- 5.Gaskin CM, Helms CA. Lipoma, lipoma variants, and well- differentiated liposarcoma (Atypical Lipomas): results of MRI evaluations of 126 consecutive fatty masses. Am J Roentgenol. 2004;182:733–739. doi: 10.2214/ajr.182.3.1820733. [DOI] [PubMed] [Google Scholar]
- 6.RAR , Cannon SR, Flanagan AM. Chondroid lipoma: correlation of imaging findings and histopathology of an unusual benign lesion. Skeletal Radiol. 2004;33:670–673. doi: 10.1007/s00256-004-0818-2. [DOI] [PubMed] [Google Scholar]
- 7.Hyzy MD, Hogendoorn PCW, Bloem JL, De Schepper AM. Chondroid lipoma: findings on radiography and MRI (2006; 7b). Eur Radiol. 2006;16:2373–2376. doi: 10.1007/s00330-006-0243-0. [DOI] [PubMed] [Google Scholar]
- 8.Hoch B, Hermann G, Klein MJ, Abdelwahab IF. Ossifying chondroid lipoma. Skeletal Radiol. 2008;37:475–480. doi: 10.1007/s00256-007-0444-x. [DOI] [PubMed] [Google Scholar]
- 9.Lakshmiah SR, Scott KWM, Whear NM, Monogham A. Chondroid lipoma: a rare but diagnostically important lesion. Int J Oral Maxillofac Surg. 2000;29:445–446. [PubMed] [Google Scholar]
- 10.Logan PM, Janzen DL, O'Connell JX, Munk PL, Connell DG. Chondroid lipoma: MRI appearances with clinical and histologic correlation. Skeletal Radiol. 1996;25:592–595. doi: 10.1007/s002560050143. [DOI] [PubMed] [Google Scholar]