

Abstract
Despite substantial increases in the prevalence of adolescent overweight and obesity documented in recent decades, few studies have prospectively tracked their development during the entire adolescent period. The aims of this study were to characterize developmental trends in prevalence, incidence, and remission of overweight and obesity using annual data collected from ages 12 to 19 for 496 adolescent females. Ethnic differences between African American (n = 37), Latina (n = 96), and European American (n = 348) adolescents were also compared. The prevalence of overweight decreased slightly across adolescence and remission rates exceeded incidence (onset). Obesity was more chronic, with increasing incidence accompanied by decreasing remission rates. Middle through late adolescence was the period of greatest risk for the transition from overweight to obesity. African American and Latina females had higher overweight and obesity prevalence than European American females throughout adolescence. Differences in prevalence were driven by higher onset rates for African American and Latina females, whereas remission rates were comparable across ethnic groups. Results suggest that adolescence is not a high-risk period for onset of obesity for European American adolescent females, but is for African American and Latina adolescent females.
Keywords: adolescents, females, overweight, obesity, longitudinal
Adolescent obesity is associated with serious medical problems including cardiovascular disease, colon cancer, and diabetes mellitus, and has psychosocial consequences such as higher body dissatisfaction, lower educational attainment, and higher rates of poverty (Merten, Wickrama, & Williams, 2008; Must & Strauss, 1999; Pesa, Syre, & Jones, 2000; Reilly & Kelly, 2010). An estimated 34% of adolescents are either overweight (16%) or obese (18%) and the prevalence of adolescent obesity has more than tripled since the 1960s (Ogden, Carroll, Curtin, Lamb, & Flegal, 2010; Troiano & Flegal, 1998). Increases in prevalence have been especially pronounced among ethnic minority females; rates among African American females have quadrupled since the 1960s (Troiano & Flegal, 1998) and doubled among Latina females since the 1980s (Flegal, Ogden, & Carroll, 2004). Cross-sectional data from national and state surveys show relatively stable rates of overweight and obesity for males across adolescence, but indicate a marginal drop for females during late adolescence (Centers for Disease Control and Prevention, 2006; Troiano & Flegal, 1998).
Although cross-sectional studies such as the National Health and Nutrition Examination Survey (NHANES) have provided valuable data on the prevalence of adolescent overweight and obesity (e.g., Ogden et al., 2010), few studies have examined developmental trajectories during adolescence by following a cohort longitudinally. One such study that followed rural European American youth from late childhood (age 9) through middle adolescence (age 16) found a marginal increase in the prevalence of obesity with age (Mustillo et al., 2003). Other longitudinal studies have showed relatively stable prevalence of both overweight and obesity throughout adolescence (Neumark-Sztainer, Wall, Eisenberg, Story, & Hannan, 2006; Thompson et al., 2007). However, there is a dearth of data on African and Latino American adolescents, who show the highest prevalence of overweight and obesity.
It is particularly important to study overweight and obesity among adolescent females since ethnic differences are more pronounced than for males. Compared with Latino males, Latina females are at higher risk for overweight (22% vs. 17%). Additionally, African American females are at higher risk for overweight (17% vs. 13%) and obesity (29% vs. 20%) compared with their male counterparts (Ogden et al., 2010). Across adolescence, an estimated 30% of European American females are either overweight (15%) or obese (15%); 46% of African American females are overweight (17%) or obese (29%); and 40% of Latina females are overweight (22%) or obese (18%). This trend persists into adulthood, as data indicate that 50% of African American women and 43% of Latina women are obese, compared with 33% of European American women (Flegal, Carroll, Ogden, & Curtin, 2010). Ethnic minority groups also exhibit greater developmental increases in weight relative to European Americans (e.g., Burke et al., 1996; Kimm et al., 2001).
Most studies of adolescent overweight and obesity have focused exclusively on tracking prevalence, typically the percentage of individuals meeting the BMI cutoff at a given age. However, clarifying incidence and remission from overweight and obesity during adolescence is particularly valuable in elucidating peak periods of risk for onset, providing information on the chronicity of these conditions, and identifying key intervention windows. We define incidence (onset) as the percentage of individuals who previously did not meet criteria for overweight or obesity, but exceeded the BMI threshold the following year. Conversely, we define remission as the percentage of individuals who previously met criteria for overweight or obesity, but fell below the BMI threshold the following year. A 1-year prospective study that examined onset and remission from obesity in children and young adolescents aged 5-13 found that children were more likely to become obese than their older counterparts and were at higher risk for remaining obese over the 1-year follow-up, with African American females exhibiting the highest incidence followed by Latina females and European American females (Kim et al., 2005). Although this study used a large and ethnically diverse population, their investigation of onset and remission consisted of cross-sectional cohorts rather than a single group followed over an extended period. Thompson and colleagues (2007) examined the annual incidence of overweight from late childhood to early adolescent in a longitudinal cohort and found that African American females had twice the incidence in early adolescence compared to their European American counterparts. However, there are no published studies to date that have examined both onset and remission across the entire adolescent period.
Studies that have examined ethnic differences in body mass index (BMI) trajectories suggest that differences in overweight and obesity emerge sometime between late childhood and early adolescence, and increase during the transition to adulthood. A cross-sectional study of African and European American females aged 5 to 17 suggests that ethnic differences emerge by middle adolescence, as African American females had a higher mean BMI than European American females after age 13 – this difference increased steadily through age 16 and accelerated through late adolescence (Freedman, Kettel-Khan, Srinivasan, & Berenson, 2000). A prospective study following African and European American females from ages 9 to 19 found that the critical age for racial divergence in adiposity was age 12, the average age at which African American females experience menarche (compared to an average age of 13 for European American girls; Kimm et al., 2001). Although these studies shed light on differences in the development of obesity among African and European Americans, they do not include Latinas, who evidence the second highest rates of obesity (Ogden et al., 2010) and represent the fastest growing minority group in the U.S. (U.S. Census Bureau, 2009).
Aims of the Present Study
This study addresses several gaps in the literature. First, we examine developmental trends descriptively over the entire period of adolescence, an especially critical time in the development of obesity in females. Second, we examine changes in incidence and remission, which could elucidate the processes that drive changes in prevalence across adolescent development and help to identify key intervention periods, which may differ by ethnicity. Third, we investigate ethnic differences between Latina females and other groups with respect to the development of adolescent overweight and obesity, for which there are limited data. Thus, the aims of the study are to examine the prevalence, incidence, and remission of overweight and obesity during adolescence for females and to test for differences in the prevalence, incidence, and remission for various ethnic groups. Examining ethnic differences in incidence and remission will help clarify whether the elevated prevalence of overweight and obesity among African American and Latina females, relative to European American females, occurs because of elevated incidence or because of lower remission (or some combination). This study should contribute to a better understanding of the development of overweight and obesity during adolescence, which is critical in informing the design of more effective prevention and treatment programs targeting unhealthy weight gain, as existing programs have been met with only limited success (see Stice, Shaw, & Marti, 2006, for a review).
Methods
Participants
Participants were 496 adolescent females from four public (82%) and four private (18%) middle schools in a metropolitan area of the southwestern U.S. Adolescents ranged in age from 11 to 15 years (M = 13) at baseline. The sample included 68% European Americans, 18% Latinas, 7% African Americans, 4% who specified other or mixed racial heritage, 2% Asian/Pacific Islanders, and 1% Native Americans. This was representative of the schools from which we sampled (65% European Americans; 21% Latinas; 8% African Americans; 4% other or mixed; 2% Asian/Pacific Islanders). Average parental education was 29% high school graduate or less, 23% some college, 33% college graduate, and 15% graduate degree, which was similar to census data for comparably aged adults in the county (34% high school graduate or less; 25% some college; 26% college graduate; 15% graduate degree).
Procedures
The study was described as an investigation of adolescent mental and physical health. An active parental consent procedure was used to recruit participants. An informed consent letter describing the study and a stamped self-addressed return envelope were sent to parents of eligible females (a second mailing was sent to non-responders). Adolescent assent was also secured. This resulted in an average participation rate of 56% of all eligible females, which was similar to that of other school-recruited longitudinal studies that required active consent and involved structured interviews (e.g., 61% for Lewinsohn, Hops, Seeley, & Andrews, 1993). The one-year prevalence rate of adolescent obesity in African Americans (19%), Latinas (13%), and European Americans (4%) was representative of the region sampled (Park, Menard, & Schoolfield, 2001). Participants completed a questionnaire, participated in a structured interview, and had their weight and height measured by female research assistants at baseline (T1) and at six annual follow-ups (T2-T7). The current report examines data collected at all seven time points. Assessments generally occurred during school hours or immediately after school at the schools. Participants received a $15 gift certificate as compensation for participating in each assessment.
Measures
Body mass
The BMI (kg/m2) was used as a proxy measure of adiposity. Height was measured to the nearest millimeter with a portable direct-reading stadiometer (Shorr Infant/Child/Adult Height Measuring Board). Cole and colleagues (Cole, Faith, Pietrobelli, & Heo, 2005) demonstrated that non-transformed BMI was superior to BMI z-scores, and comparable to BMI percentiles, for the longitudinal assessment of adiposity. Students were measured without shoes and with the body positioned such that the heels and buttocks were against the vertical support of the stadiometer and the head aligned so that the auditory canal and lower rim of the orbit were in a horizontal plane. We assessed weight to the nearest 0.1 kg using digital scales (SECA 770 Digital Floor Scale), with participants wearing light clothing without shoes or coats. At each assessment, two measures of height and weight were obtained and averaged. When it was not possible to directly measure height and weight because participants had moved out of the area, self-reported height and weight data were used. Previous research has supported the adequacy of BMI calculated from self-report data when direct measurements are not available; in one study adolescent obesity status correctly classified 96% of the time using self-reported measurements (Goodman, Hinden, & Khandelwal, 2000).
Socioeconomic status
Average parental education was used as a proxy index of adolescent socioeconomic status (SES). At T1, participants self-reported their mother and father’s highest level of educational achievement on a 6-point scale (grade school graduate, some high school, high school graduate, some college, advanced degree). Mother and father’s educational achievement were averaged to form an index of adolescent SES. Average parental education is a frequently used and accepted measure of SES in epidemiological studies of adolescent overweight and obesity (e.g., Delva, Johnston, & O’Malley, 2007).
Criteria for Overweight and Obese
We used the terms overweight and obesity since this is the terminology currently endorsed by the American Medical Association (Barlow, 2007). Because of the normative increases in BMI that occur during adolescence as a function of physical maturation, we used the international standards developed by Cole and colleagues (2000) that represent downward, age-adjusted extensions of the 25.0 and 30.0 kg/m2 cut-points recommended by the World Health Organization for overweight and obesity, respectively. The international standards are based on data from a more ethnically diverse sample, which make them well suited for testing ethnic differences. These cut points correspond to BMI values that are associated with particularly increased risk for weight-related medical problems such as diabetes mellitus (Cole, 2000; World Health Organization, 2000).
Incidence of overweight and obesity was computed as the rate among those who exhibited onset of each condition over each one-year follow-up (e.g., those who did not meet criteria for obesity at one assessment and did at the subsequent assessment). Remission of overweight and obesity was computed as the rate among those who previously met criteria, but had dropped below threshold by the subsequent annual follow-up.
Statistical Methods
To examine overweight and obesity prospectively we applied longitudinal regression analyses using generalized estimating equations (GEE). GEE is a multilevel analytic technique that is appropriate for modeling dichotomous repeated-measures data (Diggle, Heagerty, Liang, & Zeger, 2002; Liang & Zeger, 1986). A “working correlation” structure is specified a priori and defines the hypothesized relation between repeated observations on a subject. A first-order autoregressive correlation structure (AR-1) was chosen for all GEE models. This assumption is appropriate in the context of balanced longitudinal data when measurements closer in time are more correlated than measurements further apart. All GEE models were estimated with a logit link function and robust standard errors. We first examined the prevalence, incidence, and remission of overweight and obesity by participant age in the full sample (aim 1). These models regressed each outcome on age. We next examined ethnic differences in these outcomes across adolescence. In these models we regressed each outcome on age and ethnicity (aim 2). All analyses controlled for average parental education, a proxy for socioeconomic status.
The evaluation of ethnic differences focused on African American (n = 37), Latinas (n = 96), and European American (n = 348) ethnicity. Other ethnicities (n = 15) were dropped from the analyses because of insufficient numbers. For the analyses of prevalence, incidence, and remission by ethnicity, three contrasts were evaluated: African American versus European American, Latina versus European American, and African American versus Latina. Preliminary longitudinal GEE analyses tested whether the age ethnicity term accounted for significant differences in the slopes of prevalence, incidence, and remission across adolescence by ethnicity for both overweight and obesity (6 models total). In these models, the dichotomous outcome was regressed on average parental education, age, ethnicity, and the interaction of age and ethnicity. The interaction terms expressly tested whether the changes in each outcome differed significantly across the ethnic groups. Of these six models, the age ethnicity interaction was marginally significant only in the model predicting obesity incidence (χ2[2] = 5.00, p = .08), and was therefore excluded from the remaining 5 models.
Results
Missing Data
With respect to overall attrition, the percentages of participants missing both self-report and direct measurement from ages 12-19 were 0%, 1%, 3%, 3%, 2%, 3%, 4%, and 6% respectively. There were no statistically significant ethnic differences in the degree of overall attrition at any age. The percentages of participants for whom we only collected self-reported height and weight data were of the study were 0%, 1%, 4%, 8%, 13%, 14%, 28%, & 45%, from ages 12-19 respectively. Across assessment points, BMIs calculated from self-report versus direct measurement were highly correlated for the participants with both types of data (Mean r = .84, p’s < .0001). Therefore, self-reported height and weight were used to assess overweight and obesity when direct measurements were not available, to maximize statistical power.
Developmental Trends in Adolescent Overweight and Obesity
Yearly prevalence, incidence, and remission of overweight and obesity across adolescence are presented in Figures 1, 2, and 3, respectively. Most diagnoses of overweight (85.4%) and obesity (95.0%) were at least 0.5 BMI units from the clinical cut points, indicating that the majority of diagnoses were not marginal cases.
Figure 1.
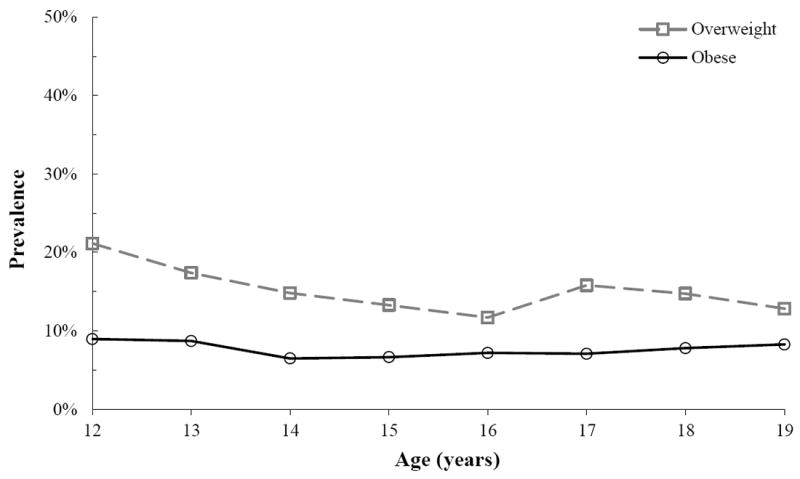
Prevalence of Adolescent Female Overweight and Obesity. All ethnicities.
Figure 2.
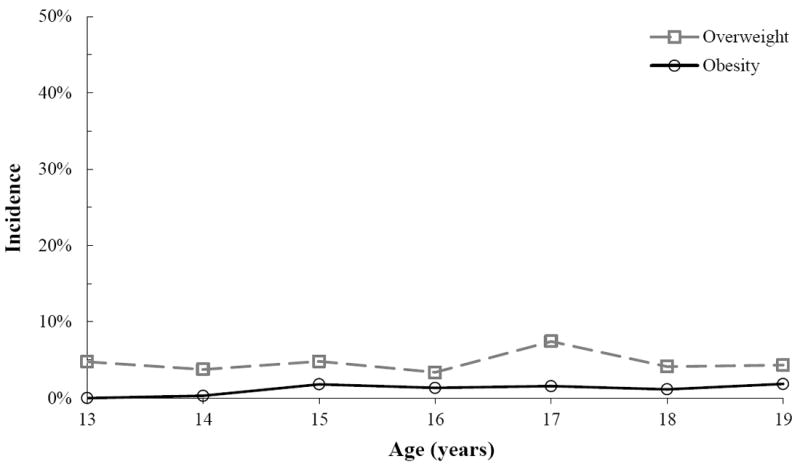
Incidence of Adolescent Female Overweight and Obesity. All ethnicities.
Figure 3.

Remission from Adolescent Female Overweight and Obesity. All ethnicities.
Prevalence
Within the overweight category, prevalence decreased from early through middle adolescence (ages 12-16) from 21.1% to 11.7%. The prevalence of overweight rebounded slightly at the beginning of late adolescence before decreasing again from 15.8% to 12.8% between ages 17-19. The effect of age was marginally significant (OR = 0.98, 95% CI = 0.96 – 1.00, p = .08), suggesting a modest decrease in overweight prevalence across adolescence. The prevalence of obesity was relatively stable across adolescence, ranging between 6.5-8.9% from ages 12-19, with no significant effect of age (OR = 1.01, 95% CI = 0.98 – 1.03, p = .52).
Incidence
The average amount of weight gain was 7.2 kg for the transition to overweight and 11.6 kg for the transition to obesity, suggesting that participants gained more than a trivial amount of weight to cross each threshold. Rates of overweight incidence varied between 3.4-4.8% during most of adolescence, peaking during middle adolescence to 7.4% at age 17. To test for curvilinear trends, overweight incidence was regressed on linear and quadratic contrasts of age. There were no significant linear (OR = 1.06, 95% CI = 0.93 – 1.20, p = .40) nor quadratic effects (OR = 0.97, 95% CI = 0.91 – 1.04, p = .41) of age indicating that risk for onset of overweight was constant through adolescence.
Obesity incidence increased from 0.0 to 1.8% between ages 13-15 and remained relatively stable through late adolescence. To test for curvilinear trends, obesity incidence was regressed on linear and quadratic contrasts of age. The linear term was significant (OR = 1.27, 95% CI = 1.04 – 1.56, p = .02) indicating that risk for obesity onset increased through adolescence. The quadratic term was non-significant (OR = 0.92, 95% CI = 0.81 – 1.04, p = .18) suggesting that the increase in obesity onset was constant through adolescence. The incidence of obesity was driven primarily by the transition from overweight into obesity (84.8%), indicating that adolescents did not typically jump from normal BMI range to obese status within any one-year interval.
Remission
The average weight loss was 2.8 kg for the transition out of overweight and 8.1 kg for the transition out of obesity. Overweight remission rates peaked at 40.3% during early adolescence at age 14 and decreased to 21.3% at age 19. The effect of age on overweight remission was statistically significant indicating that overweight remission decreased through adolescence (OR = 0.90, 95% CI = 0.80 – 1.00, p = .05). In contrast, obesity remission rates fluctuated from 8.0 to 24.1% during adolescence with no significant effect of age (OR = 0.90, 95% CI = 0.80 – 1.00, p = .05). Of the cases of obesity remission, 79.3% transitioned into overweight while 20.7% jumped directly to normal range within the one-year time frame.
Ethnic Differences in Developmental Trends
Prevalence
Ethnic differences in overweight were well established by early adolescence and persisted through age 19 with average yearly prevalence of 26.5% for African American, 19.4% for Latina, and 12.2% for European American females. The prevalence of overweight in African American (OR = 2.89, 95% CI = 1.61 – 5.20, p = .0004) and Latina females (OR = 1.64, 95% CI = 1.01 – 2.67, p = .04) was significantly higher than for European American females. The prevalence of overweight for African American females was marginally greater than the rate among Latina females (OR = 1.77, 95% CI = 0.94 to 3.31, p = .08).
With respect to obesity, average yearly prevalence was 20.5% for African American, 13.4% for Latina, and 4.2% for European American females. African American (OR = 3.94, 95% CI = 1.74 – 8.95, p = .001) but not Latina (OR = 1.84, 95% CI = 0.81 – 4.17, p = .15) females had significantly higher rates of obesity than European American females. African American females had marginally greater rates of obesity than Latina females (OR = 2.15, 95% CI = 0.88 – 5.26, p = .09).
Incidence
Yearly incidence of overweight and obesity across adolescence by ethnicity is presented in Figure 4. Ethnic differences in overweight onset were stable by age 15 with average yearly onset rates of 13.6% for African American, 5.9% for Latina, and 3.3% for European American females across adolescence. African American (OR = 4.04, 95% CI = 2.01 – 8.14, p = .0001) but not Latina (OR = 1.57, 95% CI = 0.81 – 3.01, p = .18) females had significantly higher rates of overweight onset than European American females. African American females had significantly higher rates of overweight onset than Latina females (OR = 2.58, 95% CI = 1.13 – 5.89, p = .02).
Figure 4.
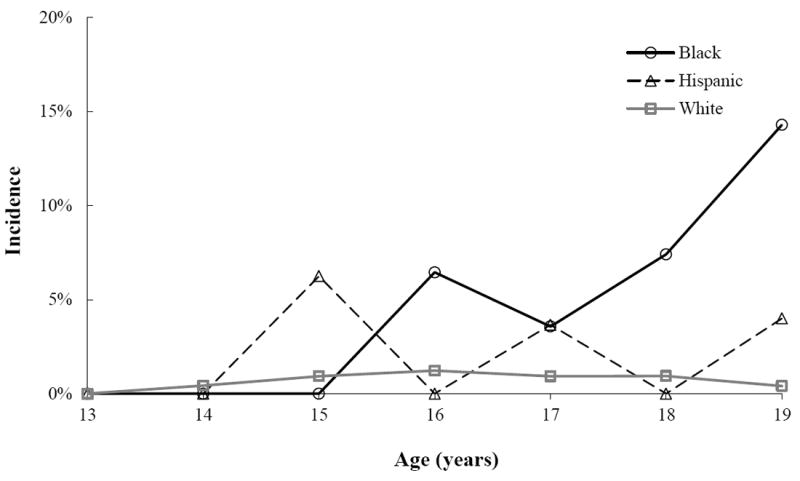
Incidence of Adolescent Female Obesity by Ethnicity. African Americans, Latinas, and European Americans only.
Average obesity incidence was 4.5% for African American, 2.0% for Latina, and 0.7% for European American females. African American females had significantly greater (OR = 5.69, 95% CI = 2.37 – 13.66, p = .0001) and Latina females marginally greater (OR = 2.15, 95% CI = 0.85 – 5.42, p = .11) incidence relative to European American females. Additionally, African American females had marginally greater incidence relative to Latina females (OR = 2.65, 95% CI = 0.96 – 7.32, p = .06). Obesity incidence among African American females was at zero levels in early adolescence and increased to 14.3% by age 19. Rates among Latina females were also at zero levels in early adolescence, peaking to 6.3% at age 15 before dropping to 4% by age 19. Incidence among European American females was the most stable with the lowest levels in early and late adolescence and peaking at 1.2% at age 16. The interaction between age and the contrast of African American versus European American ethnicity (OR = 1.74, 95% CI = 0.86 – 2.61, p = .0001) was significant indicating a greater increase in obesity incidence with age among African American compared with European American females. The interaction between age and the contrast of African American versus Latina ethnicity approached significance (OR = 2.65, 95% CI = 9.06 – 7.32, p = .06) indicating a trend of greater increase in risk for obesity incidence among African American females as they aged than Latina females.
Remission
Year-to-year rates of remission by ethnicity were somewhat unstable for both overweight and obesity, particularly for African Americans and Latinas, due to low base rates. Among initially overweight participants, the average yearly rate of remission for overweight was 25.0% in African American, 30.1% in Latina, and 23.5% in European American females. African American (OR = 1.37, 95% CI = 0.60 – 3.11, p = .19) and Latina females (OR = 1.34, 95% CI = 0.69 – 2.60, p = .39) did not show significantly different rates of remission relative to European American females and the rate of overweight remission for African Americans was comparable to that of Latinas, OR = 1.02, 95% CI = 0.42 – 2.49, p = .96.
Among initially obese participants, the average yearly rates of remission from obesity were 12.7% for African American, 14.3% for Latina, and 14.5% for European American females. Differences in the rates of obesity remission for African American (OR = 0.87, 95% CI = 0.70 – 1.09, p = .23) and Latina females (OR = 1.27, 95% CI = 0.38 – 4.23, p = .69) compared with European Americans were non-significant. The rate of overweight remission for African Americans not significantly different from that of Latinas, OR = 0.96, 95% CI = 0.20 – 4.60, p = .96.
Discussion
Substantial increases in the prevalence of adolescent overweight and obesity have been documented in recent decades, with the most pronounced increases among African Americans and Latinas. However, only a handful of studies have tracked the development of overweight and obesity across the entire adolescent period using prospective data (e.g., Kimm, Barton, et al., 2002). We used a large prospective dataset to examine maturational trends in female overweight and obesity status from ages 12 to 19 years. The aims were to describe rates of prevalence, incidence, and remission by age and elucidate differences in developmental trends among African American, Latina, and European American adolescent females. The study contributes to the extant literature by examining the entire period of adolescence, which allows identification of specific windows when intervention may be the most successful, looks at incidence and remission in order to better understand changes in prevalence, uses direct measures of height and weight, and includes Latina females.
Developmental Trends in Adolescent Overweight and Obesity
Adolescent overweight showed a trend towards decreasing prevalence, declining an average of one percentage point per year from ages 12-19. The one other study that evaluated yearly adolescent overweight prevalence (Terrell, 2002) showed comparable declines from early through middle adolescence. Two-thirds of overweight adolescents (66%) remained overweight at one-year follow-up with 27% dropping to healthy weight and 7% crossing to full threshold obesity. Year-to-year incidence (5%) of overweight did not change significantly across adolescence, indicating that the decline in prevalence was driven by remission to healthy weight. However, although remission outpaced incidence during adolescence, the rate of remission declined by an average of 2% per year, suggesting that overweight was increasingly chronic with age among adolescents that did not remit.
In contrast to the trend towards decreasing overweight prevalence, the yearly prevalence of full threshold obesity averaged a constant 8% across adolescence. Most obese adolescents (85%) remained obese one year later, with 12% dropping to overweight and 3% moving to healthy weight. The higher maintenance of rates of obesity indicates a greater chronicity for obesity compared with overweight, which to our knowledge has not been studied previously. Obesity incidence increased significantly from zero at age 13 to just under 2% at age 19. It is notable that the majority (85%) of those who showed obesity onset were already overweight, while only 15% shifted from healthy weight, supporting the importance of BMI between 25 and 29.9 as a transitional category to obesity. Kim and colleagues (2005) found that remission from obesity was lower among older children, suggesting an increased chronicity with age. Our findings suggested that during adolescence the chronicity of female obesity was driven by greater likelihood of becoming obese with no greater likelihood of remitting.
Ethnic Differences in Developmental Trends
Average prevalence by ethnicity of overweight adolescent females in the present study was comparable to national figures from NHANES 2007-2008 (Blacks: 17%; Hispanics: 22%, Whites: 15%; Ogden et al., 2010). African American and Latina females had statistically higher prevalence of overweight than European American females, consistent with previous studies comparing African and European American females (Kimm et al., 2001), with rates dropping comparably across all three groups through age 19. The average prevalence of overweight among European American females was considerably lower than for the other ethnic groups with a tenth of European American females overweight at a given age compared with a quarter of African American females and a fifth of Latina females. Over two-thirds of overweight European American females (70%) remained overweight at one year follow-up compared with just over half of overweight African American (57%) and Latina (58%) females, indicating greater movement out of overweight for these two minority groups.
Obesity incidence for African American, Latina, and European American adolescents were similar to regional rates for the large Southwestern city from which the sample was drawn (Blacks: 20%, Hispanics: 17%, Whites: 14%; Park et al., 2001), which were somewhat lower than the national average (Ogden et al., 2010). As with overweight, ethnic differences in the prevalence of obesity were present by age 12, however rates were relatively constant for all groups through adolescence. The prevalence of obesity was lowest among European American females and highest among African American and Latina females. However, average year-to-year maintenance of obesity was similar for African American (86%), Latina (86%), and European American (83%) females indicating that the chronicity of adolescent obesity was comparable across all three groups.
One important finding was that the rates of overweight and obesity incidence were significantly higher among African American and marginally higher among Latina females, but the average rates of remission were comparable across all three groups. African American females had a four-fold greater odds of obesity onset compared with European American females, while there was a trend towards two-fold greater odds of obesity onset among Latina females. This implies that African American and Latina females were at higher risk for developing overweight and obesity during adolescence, but were no less likely to remit. Collectively, these results indicate that elevated incidence was driving the higher obesity prevalence for African American and Latina females rather than differences in maintenance. For obesity incidence only, there was a marginally-significant interaction between age and African versus European American ethnicity and time, suggesting that risk of onset increased more by age for African American than European American females.
The similar trends in obesity and overweight prevalence in African versus European American females found in the present investigation are consistent with a previous prospective study, which found that the African-European American ratio in overweight and obesity prevalence remained the same across adolescence (Kimm, Barton, et al., 2002). The higher prevalence by age 12 of overweight and obesity with African American versus European American females in the present study also supports research documenting the emergence of African-European American differences in adiposity by early adolescence (Kimm et al., 2001). These findings further build upon the developmental literature to suggest that, by early adolescence, Latina females also have higher prevalence of overweight than European American females.
Strengths and Limitations
To date, only a handful of studies (e.g., Park et al., 2001) have tracked the development of overweight and obesity across the entire adolescent period using prospective data. The strength of the present study was that it covered the entire period of adolescence, examined incidence and remission in order to understand changes in prevalence, and used direct measures of height and weight. Previous published studies examining ethnic differences in adolescent overweight and obesity have focused primarily on African American and European American adolescents so this investigation addresses an important gap in the literature by also including Latina adolescents.
Although this study had a number of strengths, it is important to consider its limitations. First, the smaller number of African American and Latina participants may have limited our ability to detect ethnic differences due to larger standard errors and confidence intervals for these groups. This limitation was most pronounced in the models examining ethnic differences in incidence and remission where the samples were further restricted to the subset transitioning into or out of overweight or obesity. Second, because of insufficient representation in the current sample, we were not able to examine ethnic differences in overweight and obesity among Asian Pacific Americans and Native Americans. Third, although BMI is the recommended measure of adiposity in epidemiologic research (Dietz & Robinson, 1998), it can reflect elevations in other aspects of body composition, such as muscle mass. Fourth, because the sample consisted exclusively of female adolescents, results may not generalize to male adolescents. In spite of these limitations, our findings offer important insight for clinicians and researchers seeking to understand the development of adolescent overweight and obesity.
Clinical Implications and Directions for Future Research
The trends in overweight and obesity documented in this study suggest that overweight is less chronic than obesity as remission from overweight outpaced onset to this condition for adolescent females. In comparison, obesity became increasingly chronic with age with escalating incidence accompanied by flat rates of remission. The peak of obesity onset during middle to late adolescence indicates that this period is an important developmental transition affecting the development of full threshold obesity. Dietary intake and physical activity both contribute to unhealthy weight gain when caloric intake exceeds energy expenditure (Weinsier et al., 2002). More African American and Latina females transitioned into overweight and obesity than transitioned out, a difference that may reflect greater declines in physical activity during adolescence in some minority groups (Kimm, Glynn, et al., 2002). Additionally, lower intake of healthy (e.g., fruits and vegetables; Delva et al., 2007) and increased intake of unhealthy (e.g., high fat) foods during adolescence may also contribute to the ethnic differences in the chronicity of overweight and obesity observed in this study.
Ethnic differences in overweight and obesity may also reflect disparities in treatment. Analyses of pediatric records indicate that obesity is under diagnosed among Latina children relative to their European American counterparts (Dorsey, Wells, Krumholz, & Concato, 2005) and that counseling children to exercise occurs half as often for African American children during routine health maintenance visits (Cook, Weitzman, Auinger, & Barlow, 2005). These findings support calls for targeting obesity prevention programs during childhood (National Task Force on Prevention and Treatment of Obesity, 1994), particularly for African American and Latina children. Because ethnic differences in overweight and obesity are present by age 12, childhood prevention programs might reduce the ethnic disparity in these conditions.
Our findings indicate several directions for research on adolescent overweight and obesity. First, given the emergence of African American, Latina, and European American differences in overweight and obesity by early adolescence, a prospective study tracking the maturational trends in prevalence, incidence, and remission beginning in childhood would be particularly valuable. Second, since data on individuals of Asian Pacific and Native American descent are scarce, a developmental examination of overweight and obesity for these groups alongside African Americans, Latinas, and European Americans would represent an important contribution to the literature. Third, comparing developmental trends in overweight and obesity for males versus females would help elucidate potential gender differences in the emergence of these conditions. Finally, the present study provides the first comprehensive comparison of prevalence, onset and remission among African American, Latina, and European American adolescents, one that future prospective studies can build upon with larger samples of ethnic minority groups to assess developmental trends with increasing precision. A clearer developmental understanding of adolescent overweight and obesity will provide valuable information to inform clinical decision-making.
Acknowledgments
This study was supported by a career award (MH01708) and research grant (MH64560) from the National Institute of Mental Health.
Thanks go to project research assistants, Sarah Kate Bearman, Emily Burton, Melissa Fisher, Natalie McKee, and Katy Whitenton, our undergraduate volunteers, the Austin Independent School District, and the participants who made this study possible.
Biographies
David Huh, M.S. is a doctoral candidate in clinical psychology at the University of Washington. He conducts research on longitudinal statistical methods for evaluating behavioral health interventions.
Eric Stice, Ph.D. is a Senior Scientist at Oregon Research Institute. He conducts research on risk factors for eating disorders, obesity, and depression, as well as evaluating prevention programs for these conditions.
Heather Shaw, Ph.D. is a Senior Research Associate at Oregon Research Institute. She conducts research on risk factors and prevention of eating disorders, obesity, and depression.
Kerri Boutelle, Ph.D., is an Associate Professor in the Departments of Pediatrics and Psychiatry at University of California, San Diego, and Adjunct Professor, Department of Pediatrics and Division of Epidemiology and Community Health, University of Minnesota. She conducts research on risk factors for obesity and eating disorders, and develops and evaluates treatment programs for obesity and binge eating.
Contributor Information
David Huh, Email: dhuh@uw.edu.
Eric Stice, Email: estice@ori.org.
Heather Shaw, Email: hshaw@ori.org.
Kerri Boutelle, Email: kboutelle@ucsd.edu.
References
- Barlow SE. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: Summary report. Pediatrics. 2007;120:S164–S192. doi: 10.1542/peds.2007-2329C. [DOI] [PubMed] [Google Scholar]
- Burke GL, Bild DE, Hilner JE, Folsom AR, Wagenknecht LE, Sidney S. Differences in weight gain in relation to race, gender, age and education in young adults: the CARDIA study. Ethnicity & Health. 1996;1:327–335. doi: 10.1080/13557858.1996.9961802. [DOI] [PubMed] [Google Scholar]
- Centers for Disease Control and Prevention. Overweight among students in grades K-12--Arkansas, 2003-04 and 2004-05 school years. Morbidity and Mortality Weekly Report. 2006;55(1):5–8. [PubMed] [Google Scholar]
- Cole TJ. Establishing a standard definition for child overweight and obesity worldwide: International survey. British Medical Journal. 2000;320:1240–1240. doi: 10.1136/bmj.320.7244.1240. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole TJ, Faith MS, Pietrobelli A, Heo M. What is the best measure of adiposity change in growing children: BMI, BMI %, BMI z-score or BMI centile? European Journal of Clinical Nutrition. 2005;59:419–425. doi: 10.1038/sj.ejcn.1602090. [DOI] [PubMed] [Google Scholar]
- Cook S, Weitzman M, Auinger P, Barlow SE. Screening and counseling associated with obesity diagnosis in a national survey of ambulatory pediatric visits. Pediatrics. 2005;116:112–116. doi: 10.1542/peds.2004-1517. [DOI] [PubMed] [Google Scholar]
- Delva J, Johnston LD, O’Malley PM. The epidemiology of overweight and related lifestyle behaviors: racial/ethnic and socioeconomic status differences among American youth. American Journal of Preventive Medicine. 2007;33(4 Suppl):S178–S186. doi: 10.1016/j.amepre.2007.07.008. [DOI] [PubMed] [Google Scholar]
- Diggle P, Heagerty P, Liang K-Y, Zeger SL. Analysis of longitudinal data. 2. New York: Oxford University Press; 2002. [Google Scholar]
- Dorsey KB, Wells C, Krumholz HM, Concato JC. Diagnosis, evaluation, and treatment of childhood obesity in pediatric practice. Archives of Pediatrics and Adolescent Medicine. 2005;159:632–638. doi: 10.1001/archpedi.159.7.632. [DOI] [PubMed] [Google Scholar]
- Flegal KM, Carroll MD, Ogden CL, Curtin LR. Prevalence and Trends in Obesity Among US Adults, 1999-2008. Journal of the American Medical Association. 2010;303:235–241. doi: 10.1001/jama.2009.2014. [DOI] [PubMed] [Google Scholar]
- Flegal KM, Ogden CL, Carroll MD. Prevalence and trends in overweight in Mexican-American adults and children. Nutrition Reviews. 2004;62:S144–S148. doi: 10.1111/j.1753-4887.2004.tb00085.x. [DOI] [PubMed] [Google Scholar]
- Freedman DS, Kettel-Khan L, Srinivasan SR, Berenson GS. Black/white differences in relative weight and obesity among girls: The Bogalusa Heart Study. Preventive Medicine. 2000;30:234–243. doi: 10.1006/pmed.1999.0611. [DOI] [PubMed] [Google Scholar]
- Goodman E, Hinden BR, Khandelwal S. Accuracy of teen and parental reports of obesity and body mass index. Pediatrics. 2000;106:52–58. doi: 10.1542/peds.106.1.52. [DOI] [PubMed] [Google Scholar]
- Kim J, Must A, Fitzmaurice GM, Gillman MW, Chomitz V, Kramer E, McGowan R, et al. Incidence and remission rates of overweight among children aged 5 to 13 years in a district-wide school surveillance system. American Journal of Public Health. 2005;95:1588–1594. doi: 10.2105/AJPH.2004.054015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimm SY, Glynn NW, Kriska AM, Barton BA, Kronsberg SS, Daniels SR, Crawford PB, et al. Decline in physical activity in black girls and white girls during adolescence. The New England Journal of Medicine. 2002;347:709–715. doi: 10.1056/NEJMoa003277. [DOI] [PubMed] [Google Scholar]
- Kimm SY, Barton BA, Obarzanek E, McMahon RP, Kronsberg SS, Waclawiw MA, Morrison JA, et al. Obesity development during adolescence in a biracial cohort: The NHLBI Growth and Health Study. Pediatrics. 2002;110:e54. doi: 10.1542/peds.110.5.e54. [DOI] [PubMed] [Google Scholar]
- Kimm SY, Barton BA, Obarzanek E, McMahon RP, Sabry ZI, Waclawiw MA, Schreiber GB, et al. Racial divergence in adiposity during adolescence: The NHLBI Growth and Health Study. Pediatrics. 2001;107:e34. doi: 10.1542/peds.107.3.e34. [DOI] [PubMed] [Google Scholar]
- Lewinsohn PM, Hops H, Seeley JR, Andrews JA. Adolescent psychopathology: I. Prevalence and incidence of depression and other DSM-III-R disorders in high school students. Journal of Abnormal Psychology. 1993;102:133–144. doi: 10.1037//0021-843x.102.1.133. [DOI] [PubMed] [Google Scholar]
- Liang K-Y, Zeger SL. Longitudinal data analysis using generalized linear models. Biometrika. 1986;73:13–22. [Google Scholar]
- Merten MJ, Wickrama KAS, Williams AL. Adolescent obesity and young adult psychosocial outcomes: Gender and racial differences. Journal of Youth and Adolescence. 2008;37:1111–1122. [Google Scholar]
- Must A, Strauss RS. Risks and consequences of childhood and adolescent obesity. International Journal of Obesity. 1999;23:2–11. doi: 10.1038/sj.ijo.0800852. [DOI] [PubMed] [Google Scholar]
- Mustillo S, Worthman C, Erkanli A, Keeler G, Angold A, Costello EJ. Obesity and psychiatric disorder: Developmental trajectories. Pediatrics. 2003;111:851–859. doi: 10.1542/peds.111.4.851. [DOI] [PubMed] [Google Scholar]
- National Task Force on Prevention and Treatment of Obesity. Toward prevention of obesity: Research directions. Obesity Research. 1994;2:571–584. doi: 10.1002/j.1550-8528.1994.tb00108.x. [DOI] [PubMed] [Google Scholar]
- Neumark-Sztainer D, Wall M, Eisenberg ME, Story M, Hannan PJ. Overweight status and weight control behaviors in adolescents: Longitudinal and secular trends from 1999 to 2004. Preventive Medicine. 2006;43:52–59. doi: 10.1016/j.ypmed.2006.03.014. [DOI] [PubMed] [Google Scholar]
- Ogden CL, Carroll MD, Curtin LR, Lamb MM, Flegal KM. Prevalence of high body mass index in US children and adolescents, 2007-2008. Journal of the American Medical Association. 2010;303:242–249. doi: 10.1001/jama.2009.2012. [DOI] [PubMed] [Google Scholar]
- Park MK, Menard SW, Schoolfield J. Prevalence of overweight in a triethnic pediatric population of San Antonio, Texas. International Journal of Obesity. 2001;25:409–416. doi: 10.1038/sj.ijo.0801550. [DOI] [PubMed] [Google Scholar]
- Pesa JA, Syre TR, Jones E. Psychosocial differences associated with body weight among female adolescents: the importance of body image. Journal of Adolescent Health. 2000;26:330–337. doi: 10.1016/s1054-139x(99)00118-4. [DOI] [PubMed] [Google Scholar]
- Reilly JJ, Kelly J. Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: Systematic review. International Journal of Obesity. 2010 doi: 10.1038/ijo.2010.222. Retrieved from http://dx.doi.org/10.1038/ijo.2010.222. [DOI] [PubMed]
- Stice E, Shaw H, Marti CN. A meta-analytic review of obesity prevention programs for children and adolescents: The skinny on interventions that work. Psychological Bulletin. 2006;132:667–691. doi: 10.1037/0033-2909.132.5.667. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Terrell DF. Overweight and obesity prevalence rates among youth in the Carolinas. North Carolina Medical Journal. 2002;63:281–286. [PubMed] [Google Scholar]
- Thompson DR, Obarzanek E, Franko DL, Barton BA, Morrison J, Biro FM, Daniels SR, et al. Childhood Overweight and Cardiovascular Disease Risk Factors: The National Heart, Lung, and Blood Institute Growth and Health Study. The Journal of Pediatrics. 2007;150:18–25. doi: 10.1016/j.jpeds.2006.09.039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Troiano RP, Flegal KM. Overweight children and adolescents: Description, epidemiology, and demographics. Pediatrics. 1998;101:497–504. [PubMed] [Google Scholar]
- U.S. Census Bureau. Census Bureau estimates nearly half of children under age 5 are minorities. 2009 May 24; Retrieved from http://www.census.gov/newsroom/releases/archives/population/cb09-75.html.
- Weinsier RL, Hunter GR, Desmond RA, Byrne NM, Zuckerman PA, Darnell BE. Free-living activity energy expenditure in women successful and unsuccessful at maintaining a normal body weight. The American Journal of Clinical Nutrition. 2002;75(3):499–504. doi: 10.1093/ajcn/75.3.499. [DOI] [PubMed] [Google Scholar]
- World Health Organization. Obesity: Preventing and managing the global epidemic. Geneva: Author; 2000. WHO Technical Report Series No. 894. [PubMed] [Google Scholar]