

Abstract
Background:
The purpose of this study was to investigate the effects of two types of rehabilitation techniques, including aerobic and strengthening exercises on patients with knee rheumatoid arthritis (RA).
Methods:
48 male patients with knee RA were randomly assigned into 3 groups, including aerobic exercises, strengthening exercise, and control. The two first groups completed their treatment protocol for 8 weeks, 3 days per week. Visual Analogue Scale, WOMAC questionnaire, 6-minute walking test, standard goniometer were used to assess pain severity, functional ability, walking ability, knee joint ROM respectively at baseline and after applying therapeutic interventions. The data were analyzed using one-way analysis of variance (ANOVA) at P < 0.05 significant level.
Results:
Participants had a mean ± SD age of 58.6 ± 7.8 years (height 1.72 ± 0.07 m, weight 81.0 ± 6.4 kg) with no significant difference between three groups. Both therapeutic interventions reduced pain significantly (P < 0.001) compared to the control group, without significant difference between the two experimental groups. The patients fulfilled aerobic exercise attained higher levels of function and walking ability compared to strengthening group significantly (P < 0.001). The knee range of motion (ROM)wassignificantly (P < 0.001) improved in the two experimental groups in comparison to controls, the strengthening group had more significant (P < 0.001) improvement.
Conclusions:
It can be concluded that an aerobic exercise program improves functional and walking ability in patients with knee RA, and strengthening exercise has more efficient effect on knee ROM, both aerobic and strengthening exercises can equally relieve pain.
Keywords: Aerobic exercise, knee joint, rheumatoid arthritis, strengthening exercise
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic inflammatory disorder affecting the joints and presenting with multiple systemic manifestation.[1] RA involves 1% of population in the world and can result in severe disability.[2] Many studies indicate the high incidence of this disease,[3–6] although the others confirm the reduction of RA prevalence among people.[7,8]
Alternative periods of improvement and exacerbation occur during this disease.[9,10] Morning stiffness, pain, swelling, joint erosion, muscle weakness, and reducing aerobic capacity are common signs and symptoms for RA.[11–14] Previous studies declare that RA can cause reduction in the level of physical activity, muscle contractures, and atrophy. This condition may lead to poor physical fitness.[15–17] Hsieh et al. (1987) indicated that weakness of Hamstring and Quadriceps muscles can occur as the results of RA.[18] Furthermore, decreasing isotonic strength and endurance may arise because of immobilization with casts, bandages, or curing by traction techniques.[19] Muscle weakness usually results in joint stiffness and decreasing ROM that involves daily activities and quality of life.[20,21] However, due to fear of increasing joint inflammation and accelerating cartilage subversion in patients with RA, they prefer to perform assisted exercises gently.[22,23] On the other hand, it has been suggested that strengthening exercises have appropriate effects for patients with RA.[24,25]
Aerobic exercise is a non-specific activity with the aim of improving physical function, alleviating pain and increasing respiratory capacity.[26,27] Most of these exercises are simple to carry out and can be followed by some activities including; walking, cycling, and going up and down the stairs. Aerobic exercises can reduce pain and fatigue and can improve function in individuals with RA.[28,29] Despite the proper influence of this kind of training, aerobic exercise is neglected by therapists in the rehabilitation management.
Due to increasing pain, reducing ROM, walking ability and physical activity as the complications of RA, it is absolutely essential to inquire about this rheumatologic disorder. Thus, the aim of this study was to investigate the effects of strengthening and aerobic exercises on function, knee ROM, pain, and walking ability in patients with RA and then comparing them to each other.
METHODS
Patients
We conducted a supervised quasi-experimental and perspective design study with a non-randomized, pretest-posttest control group. 54 accessible patients with unilateral knee RA were selected. The exclusion criteria were knee osteoarthritis, fracture of lower limb bones, epilepsy, cardiac and respiratory conditions, and no satisfaction of individual to participate in the study. Regarding these criteria, 6 persons were eliminated, then 48 participants (mean ± SD: age 58.6 ± 7.8 years, height 1.72 ± 0.07 m, weight 81.0 ± 6.4 kg) were considered as the sample for this study. The subjects were randomly assigned into 3 groups (each group consisting of 16 individuals). The first group (group A) (mean ± SD: age 59.4 ± 8.1 years, height 1.74 ± 0.08 m, weight 83.0 ± 6.0 kg) were treated by aerobic exercise. The second group (group B) (mean ± SD: age 57.0 ± 7.4 years, height 1.71 ± 0.07 m, weight 78.6 ± 5.8 kg) followed the strengthening exercise protocol. The third group (group C) (mean ± SD: age 59.6 ± 8.3 years, height 1.72 ± 0.06 m, 81.4 ± 7.0 kg), called control group, did not receive any treatment and were beseeched to follow their ordinary life style.
The subjects took no medicine and did not perform any other regular exercise or sport during the treatment period.
Exercise protocol
The therapist clarified all the tests and procedures of management for the whole patients. Each subject in group A ran on the treadmill for about 30 minutes, while the speed was set according to the patient ability.[30] In group B, 1 RM (the maximum load an individual is able to displace without any fatigue) was determined for Hamstring and Quadriceps muscles. Then, the patients followed the strengthening exercise progressively. All the therapeutic exercises were done based on training scientific principles such as, intensity, frequency, time, specificity, and overload. However, the therapist perpended to all the complementary and trick movements of patients and tried to avoid them.
All the participants in experimental groups perused their own specific protocol for 8 weeks, 3 days per week, and for approximately 30 to 45 minutes in each therapeutic session.
Data collection
The pain intensity at rest was graded according to Visual Analogue Scale (VAS), and functional ability was assessed by Western Ontario and McMaster Osteoarthritis Index (WOMAC).[31,32] In order to appraise walking ability, 6-minute walking test was utilized.[33,34] In addition, we used standard goniometer to measure knee flexion and extension ROMs.[35]
Statistical analysis
Using SPSS statistical analysis package, version 19, the data were analyzed. We used non-parametric tests to avoid potential errors from non-normal distribution of the data. One-way ANOVA was used for differences between the groups. Statistical significance was set at P < 0.05.
RESULTS
Pain intensity
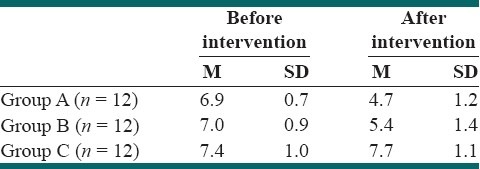
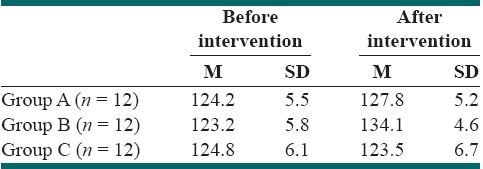
Statistical analysis revealed that there is significant (P < 0.001, F = 26.4) difference in pain intensity between the 3 groups after treatment. The patients’ pain in both A and B groups decreased significantly (P < 0.001) in comparison to group C, although there was no significant (P > 0.05) difference between these 2 experimental groups [Table 1].
Table 1.
Pain intensity before and after treatment (mean ± SD)
Functional ability
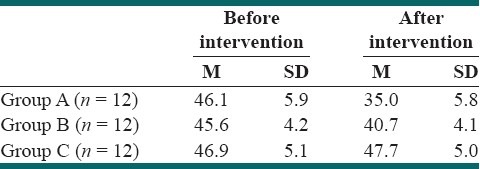
The level of functional ability was significantly (P < 0.001, F = 327.2) different between the 3 groups after 8 weeks. Further analysis indicated that both A and B groups had better functional ability than the group C significantly (P < 0.001). However, we noticed that group A had more improvement in functional ability in comparison to group C significantly (P < 0.001) [Table 2].
Table 2.
Functional ability before and after treatment (mean ± SD)
Walking ability
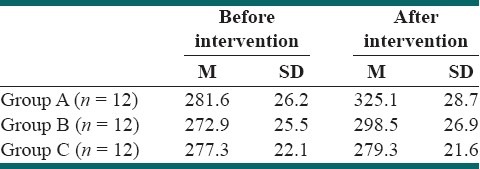
There was significant (P < 0.001, F = 156.7) difference in the walking distance between the 3 groups. While walking ability was significantly (P < 0.001) increased in both experimental groups compared to group C, group A had more progression than group B (P < 0.001) [Table 3].
Table 3.
Walking distance before and after treatment (mean ± SD) (Meter)
Knee extension ROM
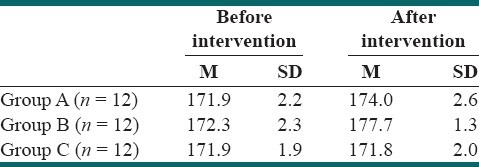
Knee extension ROM was significantly (P < 0.001, F = 36.8) different between the groups. As we realized that both A (P < 0.05) and B (P < 0.001) had more increase in knee extension ROM after therapeutic interventions compared to group C. Comparing the 2 experimental groups, the improvement was significantly (P < 0.001) more in group B [Table 4].
Table 4.
Knee extension ROM before and after treatment (mean ± SD) (Degree)
Knee flexion ROM
Knee flexion ROM was significantly different between the 3 groups (P < 0.001). While both groups performed therapeutic exercises had more improvement in knee extension ROM than the group C (P < 0.00), this parameter was significantly increased in group B in comparison to group A (P < 0.001) [Table 5].
Table 5.
Knee flexion ROM before and after treatment (mean ± SD) (Degree)
DISCUSSION
The aim of this study was to investigate the effects of aerobic and strengthening exercises on pain intensity and function of patients with rheumatoid arthritis of knee joint. We found that both therapeutic techniques decreased pain and improved function. In addition, it was obvious that both therapeutic interventions can improve walking ability, but aerobic exercise had more drastic effects. Finally, we understood that while both methods are effective to increase knee ROM, strengthening exercise was superior to the other one.
Previous studies show controversial results about the effects of exercise in patients with RA.[36–39] Barbara et al. (2011), after applying a combined exercise program including strength and endurance training on 40 patients with RA, found that such therapeutic protocol can improve functional ability of these patients.[40]
However, Baillet et al. (2009) indicated that 4 weeks dynamic exercise program is effective on aerobic fitness and quality of life in RA patients.[41] In a systemic review study, Baillet et al. (2010) concluded that cardiorespiratory aerobic exercise appears to be efficient for individuals with RA, and can decrease pain and improve functional status in the RA patients. However, the authors expressed that the degree of the effect of aerobic exercise on the above parameters is small.[42] In a Meta – analysis review, Kelly et al. (2011) studied the data sources consisted of 6 electronic databases and noted the efficiency of communicated – deliverable exercise for RA patients. They realized that this kind of exercise can improve physical function and alleviate pain in patients with RA.[43]
The results of present study confirm the above-mentioned studies. Although our results are promising, there were some limitations in this study, including; (1) the activities of daily living were different either in control or in experimental groups’ patients. Then, this difference could influence our results, interfere with them, (2) although the therapist made any endeavor to encourage subjects in both experimental groups to follow their own specific exercise with the best attempt accurately, there was discrepancy in self-patients’ motivation. However, the whole patients completed their exercise protocols for 8 weeks.
In this study, we observed that both type of therapeutic interventions can improve walking ability, as regards the individuals treated by aerobic exercise experienced higher levels of walking ability compared to strengthening exercise. The nature of aerobic exercise executed by subjects was relatively similar to walking pattern. Thus, the authors believe that further effect of aerobic exercise on walking ability is possibly contributed to such resemblance mentioned in the above. The desirable effect of aerobic exercise on walking ability is supported in previous studies.
These data indicate the efficiency of aerobic and strengthening for increasing knee joint ROM in patients with RA although the knee flexion and extension ROMs were increased more in patients who pursued aerobic exercise than strengthening exercise. As decreasing muscular strength is one of the complications associated to RA,[18] it can result in loosing ROM. Regarding this fact, we presumably assume that increasing knee joint flexion and extension ROMs is related to improvement in muscle strength achieved by strengthening exercise.
CONCLUSION
It can be concluded that both aerobic and strengthening exercises can reduce pain, improve functional status, walking ability, and flexion and extension ROMs of the knee joints in patients with knee RA. Due to more appropriate effects of aerobic treatment protocol on functional ability, use of aerobic exercise as a fundamental part of rehabilitation program can be recommended for individuals with feeble physical ability. In addition, we suggest to exert strengthening exercises in order to increase knee joint ROM, or at least for maintaining the available ROM.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Hahn BH. Systemic lupus erythematosus. In: Braunwald E, Fauci A, Kasper D, Hauser SL, Longo DL, Jameson JL, editors. Harrison's principle of internal medicine. 17th ed. New York: McGraw-Hill; 2008. pp. 2075–83. [Google Scholar]
- 2.Schellekens G, Visser H, Jong B, Hoogen F, Hazes J, Breedveld F, et al. The diagnostic properties of rheumatoid arthritis antibodies recognizing a cycle Citruccinated Peptid. Arthritis Rheum. 2000;43:155–63. doi: 10.1002/1529-0131(200001)43:1<155::AID-ANR20>3.0.CO;2-3. [DOI] [PubMed] [Google Scholar]
- 3.Symmons D, Turner G, Webb R, Asten P, Barrett E, Lunt M, et al. The prevalence of rheumatoid arthritis in the United Kingdom: New estimate for a new century. Rheumatology. 2002;41:793–800. doi: 10.1093/rheumatology/41.7.793. [DOI] [PubMed] [Google Scholar]
- 4.Kaipiainen-Seppanen O, Kautiainen H. Declining trend in the incidence of rheumatoid factor-positive rheumatoid arthritis in Finland 1980–2000. J Rheumatol. 2006;33:2132–8. [PubMed] [Google Scholar]
- 5.Alamanos Y, Voulgari P, Drosos A. Incidence and prevalence of rheumatoid arthritis, based on the 1987 American College of Rheumatology criteria: A systematic review. Semin Arthritis Rheum. 2006;36:182–8. doi: 10.1016/j.semarthrit.2006.08.006. [DOI] [PubMed] [Google Scholar]
- 6.Drosos A, Alamanos I, Voulgari V, Psychos N, Katsaraki A, Paradopoulos I, et al. Epidemiology of adult rheumatoid arthritis in northwest Greece 1987–1995. J Rheumatol. 1997;24:2129–33. [PubMed] [Google Scholar]
- 7.Helmick C, Felson D, Lawrence D, Gabriel S, Hirsch R, Kwoh K, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part I. Arthritis Rheum. 2008;58:15–25. doi: 10.1002/art.23177. [DOI] [PubMed] [Google Scholar]
- 8.Wiles N, Symmons D, Harrison B, Barrett E, Barrett J, Scott D, et al. Estimating the incidence of rheumatoid arthritis: Trying to hit a moving target? Arthritis Rheum. 1999;42:1339–46. doi: 10.1002/1529-0131(199907)42:7<1339::AID-ANR6>3.0.CO;2-Y. [DOI] [PubMed] [Google Scholar]
- 9.Anderson RJ. Rheumatoid arthritis: Clinical and laboratory features. In: Klippel JH, editor. Primer on the Rheumatic Diseases. 12th ed. Atlanta: Arthritis Foundation; 2001. p. 218. [Google Scholar]
- 10.Boissonnault WG, Goodman CC. Bone, joint, and soft tissue disorders. In: Goodman CC, Fuller KS, Boissonnault WG, editors. Pathology: Implications for the Physical Therapist. 2nd ed. Philadelphia: WB Saunders; 2003. p. 929. [Google Scholar]
- 11.Arnett F, Edworthy S, Bloch D, Mschane D, Fries J, Cooper N, et al. The American Rheumatism Association 1987 revised criteria for the classification of rheumatoid arthritis. Arthritis Rheum. 1988;31:315–24. doi: 10.1002/art.1780310302. [DOI] [PubMed] [Google Scholar]
- 12.Ekdahl C, Broman G. Muscle strength, endurance, and aerobic capacity in rheumatoid arthritis: A comparative study with healthy subjects. Ann Rheum Dis. 1992;51:35–40. doi: 10.1136/ard.51.1.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Lechner D, McCarthy C, Holden M. Gait Deviations in Patients with Juvenile Rheumatoid Arthritis. Phys Ther. 1987;67:1335–41. doi: 10.1093/ptj/67.9.1335. [DOI] [PubMed] [Google Scholar]
- 14.Heijde D. Joint erosions and patients with early rheumatoid arthritis. Rheumatology. 1995;34(Suppl 2):74–8. [PubMed] [Google Scholar]
- 15.Hakkinen A, Hannonen P, Hakkinen K. Muscle strength in healthy people and in patients suffering from recent-onset inflammatory arthritis. Rheumatology. 1995;34:355–60. doi: 10.1093/rheumatology/34.4.355. [DOI] [PubMed] [Google Scholar]
- 16.Ekblom B, Lovgren O, Alderin M, Fridstrom M, Satterstrom G. Physical performance in patients with rheumatoid arthritis. Scand J Rheumatol. 1974;3:121–5. doi: 10.3109/03009747409097136. [DOI] [PubMed] [Google Scholar]
- 17.Minor MA, Hewett JE, Webel RR, Dreisinger TE, Kay DR. Exercise tolerance and disease related measures in patients with rheumatoid arthritis and osteoarthritis. J Rheumatol. 1988;15:905–11. [PubMed] [Google Scholar]
- 18.Hsieh LF, Didenko B, Schumacher HR, Torg JS. Isokinetic and isometric testing of knee musculature in patients with rheumatoid arthritis with mild knee involvement. Arch Phys Med Rehabil. 1987;68:294–7. [PubMed] [Google Scholar]
- 19.Nordjeso LO, Nordgren B, Wigren A, Kolstad K. Isometric strength and endurance in patients with severe rheumatoid arthritis or osteoarthrosis in the knee joints. Scandinavian J Rheumatol. 1983;12:152–6. doi: 10.3109/03009748309102902. [DOI] [PubMed] [Google Scholar]
- 20.Segal NA, Torner JC, Felson DT, Niu J, Sharma L, Lewis CE, et al. Knee extensor strength does not protect against incident knee symptoms at 30 months in the Multi center knee osteoarthritis (MOST) cohort. PM R. 2009;1:459–65. doi: 10.1016/j.pmrj.2009.03.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Keith K, Loretta W. A qualitive study on patients with knee osteoarthritis to evaluate the influence of different pain patterns on patient's quality of life and to find out patient's interpretation and coping strategic for the disease. Rheumatol Rep. 2011;3:9–15. [Google Scholar]
- 22.Helene A. Exercise effects in patients with adult idiopathic inflammatory myopathies. Curr Opin Rheumatol. 2009;21:158–63. doi: 10.1097/BOR.0b013e328324e700. [DOI] [PubMed] [Google Scholar]
- 23.Semble EL. Rheumatoid arthritis: New approaches for its evaluation and management. Arch Phys Med Rehabil. 1995;76:190–201. doi: 10.1016/s0003-9993(95)80029-8. [DOI] [PubMed] [Google Scholar]
- 24.Breedland I, Scheppingen C, Leijsma M, Verheij-Jansen N, Weert E. Effects of a Group-Based Exercise and Educational Program on Physical Performance and Disease Self-Management in Rheumatoid Arthritis: A Randomized Controlled Study. Phys Ther. 2011;91:879–93. doi: 10.2522/ptj.20090010. [DOI] [PubMed] [Google Scholar]
- 25.Karatepe A, Günaydin R, Türkmen G, Kaya T. Effects of home-based exercise program on the functional status and the quality of life in patients with rheumatoid arthritis: 1-year follow-up study. Rheumatol Int. 2011;31:171–6. doi: 10.1007/s00296-009-1242-7. [DOI] [PubMed] [Google Scholar]
- 26.Jun I, Yoshihiro S, Tsuyoshi T, et al. Effectiveness of exercise for osteoarthritis of the knee: A review of literature. World J Orthop. 2011;2:37–42. doi: 10.5312/wjo.v2.i5.37. [DOI] [PMC free article] [PubMed] [Google Scholar] [Retracted]
- 27.Brittary O, Nicole L, Terry L, Joseph M. Hip and knee muscle function following aerobic exercise in individuals with patellofemoral pain syndrome. Kinesiology. 2011;21:631–7. doi: 10.1016/j.jelekin.2011.04.006. [DOI] [PubMed] [Google Scholar]
- 28.Scarvell J, Elkins M. Aerobic exercise is beneficial for people with rheumatoid arthritis. Br J Sports Med. 2011;45:1008–9. doi: 10.1136/bjsports-2011-090388. [DOI] [PubMed] [Google Scholar]
- 29.Harkcom T, Lampman R, Banwell B, Castor W. Therapeutic value of graded aerobic exercise training in rheumatoid arthritis. Arthritis Rheum. 1985;28:32–9. doi: 10.1002/art.1780280106. [DOI] [PubMed] [Google Scholar]
- 30.Kisner C, Colby LA. Therapeutic exercise: Foundation and techniques. 5th ed 2005. [Google Scholar]
- 31.Bellamy N, Buchanan WW, Goldsmith CH, et al. Validation of WOMAC: A health status measure for measuring clinically important patient relevant outcomes following total hip or knee arthroplasty in osteoarthritis. J Orthop Rheumatol. 1998;1:95–108. [PubMed] [Google Scholar]
- 32.Bellamy N, Buchanan WW, Goldsmith CH, Campbell J, Stitt LW. Validation study of WOMAC: A health status instrument for measuring clinically important patient relevant outcomes to antirheumatic drug therapy in patients with osteoarthritis of the hip or knee. J Rheumatol. 1988;15:1833–40. [PubMed] [Google Scholar]
- 33.Ulla E, Signy R. The six-minute walk test in outpatients with obesity: Reproducibility and known group validity. Physiother Int. 2008;13:84–93. doi: 10.1002/pri.398. [DOI] [PubMed] [Google Scholar]
- 34.Du H, Newton PJ, Salamonson Y, Carrieri-Kohlman VL, Davidson PM. A review of the six-minute walk test: Its implication as a self-administered assessment tool. Eur J Cardiovasc Nurs. 2009;8:2–8. doi: 10.1016/j.ejcnurse.2008.07.001. [DOI] [PubMed] [Google Scholar]
- 35.Coglianese D. Muscles: Testing and function with posture and pain. 5th ed (with Primal Anatomy CD-ROM) Phys Ther. 2006;86:304–5. [Google Scholar]
- 36.Häkkinen A, Sokka T, Kotaniemi A, Hannonen P. A randomized two year study of the effects of dynamic strength training on muscle strength, disease activity, functional capacity, and bone mineral density in early rheumatoid arthritis. Arthritis Rheum. 2001;44:515–22. doi: 10.1002/1529-0131(200103)44:3<515::AID-ANR98>3.0.CO;2-5. [DOI] [PubMed] [Google Scholar]
- 37.Ende C, Breedveld F, Cessie S, Dijkmans B, Mug A, Hazes J. Effect of intensive exercise on patients with active rheumatoid arthritis.A randomised clinical trial. Ann Rheum Dis. 2000;59:615–21. doi: 10.1136/ard.59.8.615. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Jong Z, Munneke M, Zwinderman A, Kroon H, Ronday K, Lems W, et al. Long term high intensity exercise and damage of small joints in rheumatoid arthritis. Ann Rheum Arthritis Dis. 2004;63:1399–405. doi: 10.1136/ard.2003.015826. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Jong Z, Munneke M, Zwinderman AH, Kroon H, Jansen A, Ronday K, et al. Is a longterm high-intensity exercise program effective and safe in patients with rheumatoid arthritis? Results of a randomized controlled trial. Arthritis Rheum. 2003;48:2415–24. doi: 10.1002/art.11216. [DOI] [PubMed] [Google Scholar]
- 40.Barbara S, Leeb G, Strehblow C, Schobersberger W, Haber P, Cauza E. The effects of strength and endurance training in patients with rheumatoid arthritis. Clin Rheumatol. 2011;30:623–32. doi: 10.1007/s10067-010-1584-2. [DOI] [PubMed] [Google Scholar]
- 41.Baillet A, Payraud E, Niderprim V, Nissen M, Allenet B, François P, et al. A dynamic exercise programme to improve patients’ disability in rheumatoid arthritis: A prospective randomized controlled trial. Rheumatology (Oxford) 2009;48:410–15. doi: 10.1093/rheumatology/ken511. [DOI] [PubMed] [Google Scholar]
- 42.Baillet A, Zeboulon N, Gossec L, Combescure C, Bodin LA, Juvin R, et al. Efficacy of cardiorespiratory aerobic exercise in rheumatoid arthritis: Meta-analysis of randomized controlled trials. Arthritis Care Res. 2010;62:984–92. doi: 10.1002/acr.20146. [DOI] [PubMed] [Google Scholar]
- 43.Kelley G, Kelley K, Hootman J, Jones D. Effects of Community-deliverable exercise on pain and physical function in adults with arthritis and other rheumatic diseases: A Meta-analysis. Arthritis Care Res. 2011;63:79–93. doi: 10.1002/acr.20347. [DOI] [PubMed] [Google Scholar]