

Abstract
Introduction
We assessed the correlation between intimate partner violence (IPV) and health behaviors, including seat belt use, smoke alarm in home, handgun access, body mass index, diet, and exercise. We hypothesized that IPV victims would be less likely to have healthy behaviors as compared to women with similar demographics.
Methods
All adult female patients who presented to 3 Atlanta-area emergency department waiting rooms on weekdays from 11AM to 7PM were asked to participate in a computer-based survey by trained research assistants. The Universal Violence Prevention Screen was used for IPV identification. The survey also assessed seatbelt use, smoke alarm presence, handgun access, height, weight, exercise, and diet. We used chi-square tests of association, odds ratios, and independent t-tests to measure associations between variables.
Results
Participants ranged from 18 to 68 years, with a mean of 38 years. Out of 1,452 respondents, 155 patients self-identified as white (10.7%), and 1,218 as black (83.9%); 153 out of 832 women who were in a relationship in the prior year (18.4%) screened positive for IPV. We found significant relationships between IPV and not wearing a seatbelt (p<0.01), handgun access (p<0.01), and eating unhealthy foods (p<0.01).
Conclusion
Women experiencing IPV are more likely to exhibit risky health behaviors than women who are not IPV victims.
INTRODUCTION
Intimate partner violence (IPV) is a serious and commonly encountered public health issue in the United States (U.S.). Studies have shown that almost one-fourth of U.S. women have been victimized by an intimate partner at some point in their lives, with higher rates in low-income and black populations.1–3
IPV is associated with several health problems and behaviors. Victims of IPV have been shown to have 2 to 5 times the risk of family and social problems, depression, anxiety, and sexually transmitted diseases when compared to never-abused women in age-adjusted models.4 Additionally, women victimized by IPV have been shown to engage in more negative health behaviors, such as cigarette smoking, binge drinking, and failing to have a checkup with a doctor within the past one year.5
While it is reasonable to assume that IPV victims who have been shown to endorse negative health behaviors would similarly report less healthy behaviors, very little research has been performed to link IPV with a decrease in these healthy behaviors, such as seat belt use and eating a healthy diet. This link is important; as it demonstrates how likely IPV victims are to engage in behaviors that can result in personal injury and development of chronic disease, in addition to the conditions and injuries that directly result from their abuse. This association may also help explain why certain populations are more susceptible to IPV by qualifying some women as greater risk-takers in multiple behavioral areas, such as in personal relationships as well as their health. Finally, these results will highlight areas of behavioral modification that healthcare providers can screen for and address when treating women who have experienced IPV.
Our goal was to study the relationship between IPV and commonly practiced health behaviors among at-risk patients in the emergency department (ED), using data generated from a computer-based survey of female patients who presented to three urban EDs. We specifically looked at associations with seat belt use, handgun access, smoke alarm presence, body mass index (BMI), diet, and exercise. While these particular variables were selected from a preexisting dataset, they were all chosen due to their requirement of personal effort for successful behavior performance. As they are all highly dependent on individual action, these behaviors demonstrate high potential for future modification.
We hypothesized that women who had experienced IPV would be more likely to engage in unhealthy behaviors and less likely to endorse healthy behaviors.
METHODS
Study Design, Setting and Population
This study was a correlational analysis of a preexisting dataset. We obtained the dataset from a study that was based in 3 EDs in a large city in the southeastern U.S. Most participants were patients at a Level I trauma hospital in this city, which sees approximately 105,000 ED patients annually. This main study location conducted 969 patient screenings from June 2008 to August 2009. Ninety-nine patients were screened at a tertiary and quarternary care hospital that has an annual ED census of over 30,000 patients, from March 2009 through December 2009. The third hospital is a community-based hospital with 50,000 ED patients annually. This location screened 449 participants between July 2008 and March 2009. All three hospitals are academically affiliated with a nationally prominent university, with residents from various services and medical students rotating through each ED.
Study Protocol
Research assistants asked all adult female patients who presented to these 3 ED waiting rooms on weekdays from 11AM to 7PM to participate in a computer-based survey. These assistants had received training in following protocol and documentation, patient interaction, and working in the ED. Participants were excluded if they were not fluent in English, showed evidence of intoxication, or were critically ill, currently taking anti-psychotics, or unable to complete a 20-minute questionnaire.
Women who agreed to participate were taken to a private kiosk in the ED to complete a computer survey. Women who screened positive for IPV received printed educational information and a list of community resources for IPV. Research assistants then consented them to participate in the study and administered a short survey regarding any relationship issues and general health status.
The data collected through the surveys and follow-up interviews were entered into a computer database and cleaned by research assistants.
Measures
The main study outcomes were comparisons of health maintenance behaviors to the incidence of IPV. The health maintenance behaviors studied were seatbelt use, smoke alarm presence in home, handgun access, BMI, daily healthy or unhealthy diet, and weekly exercise frequency.
Participants responded “yes” or “no” to the questions, “When you are in a car, do you always use a seatbelt?”, “Does your home have a working smoke alarm (by working we mean installed and with a working battery in it)?,” and “Do you have access to a handgun?” In order to assess diet habits, participants responded “yes” or “no” to the questions, “Do you eat foods like whole grain bread, cereal, fresh fruits or vegetables every day?”, and “Do you eat foods like fatty meat, cheese, fried foods, or eggs everyday?” To assess exercise frequency, participants were asked, “In an average week, how many times do you engage in physical activity (exercise or work which lasts at least 20 minutes without stopping and which is hard enough to make you breathe heavier and your heart beat faster)?”, to which they could answer, “At least 3 times per week,” “1–2 times per week,” or “Less than 1 time per week.” Participants self-reported their height and weight, which were used to calcuate a BMI for each woman.
The computerized survey used the Universal Violence Prevention Screening Protocol (UVPSP), a 6-item, previously validated instrument initially developed by the ED at George Washington University. This tool identifies IPV victimization by assessing any physical, sexual, and verbal violence with yes or no responses. A positive answer to any one question causes the respondent to screen positive for IPV. This tool has been validated in other studies; one study published in 2003 showed that women who were victims of IPV were more likely to answer affirmatively to each screening question on the UVPSP.6
Data Analysis
This project was a secondary analysis of a preexisting dataset from a cross-sectional multisite study. This initial study assessed the impact of educational brochures on patient contact with support resources and patient harm-reduction strategies. This study was reviewed and approved by the institutional review board of the university associated with the main study location and the hospital research oversight committee.
We undertook all analyses using SPSS (SPSS Inc.; v. 19.0; Chicago, IL). Simple descriptive statistics were calculated and are reported as counts, percentages, means, SDs, and ranges, as appropriate. We compared seatbelt use, smoke alarm access, handgun access, exercise frequency, and daily consumption of healthy and unhealthy foods between IPV victims and non-victims using chi-square tests of association and odds ratios. We also used chi-square tests of association to analyze differences in exercise frequency between victims and non-victims, using those who reported exercising less than once per week as the reference group to compare against women who exercised 1 to 2 times per week and those who exercised at least 3 times weekly. We used an independent t-test to assess for significant differences in BMI between IPV victims and non-victims. Standard assumptions for chi-square tests of association and t-tests were verified. We did not conduct power analyses, as this was a retrospective analysis.
RESULTS
Of 3,381 women approached, 1,474 (43.6%) agreed to participate in the survey and comprised our study population for the general comparisons of IPV associations with health measures. One hundred and fifty-three women out of the 832 women in a recent relationship (18.4%) were positive for IPV.
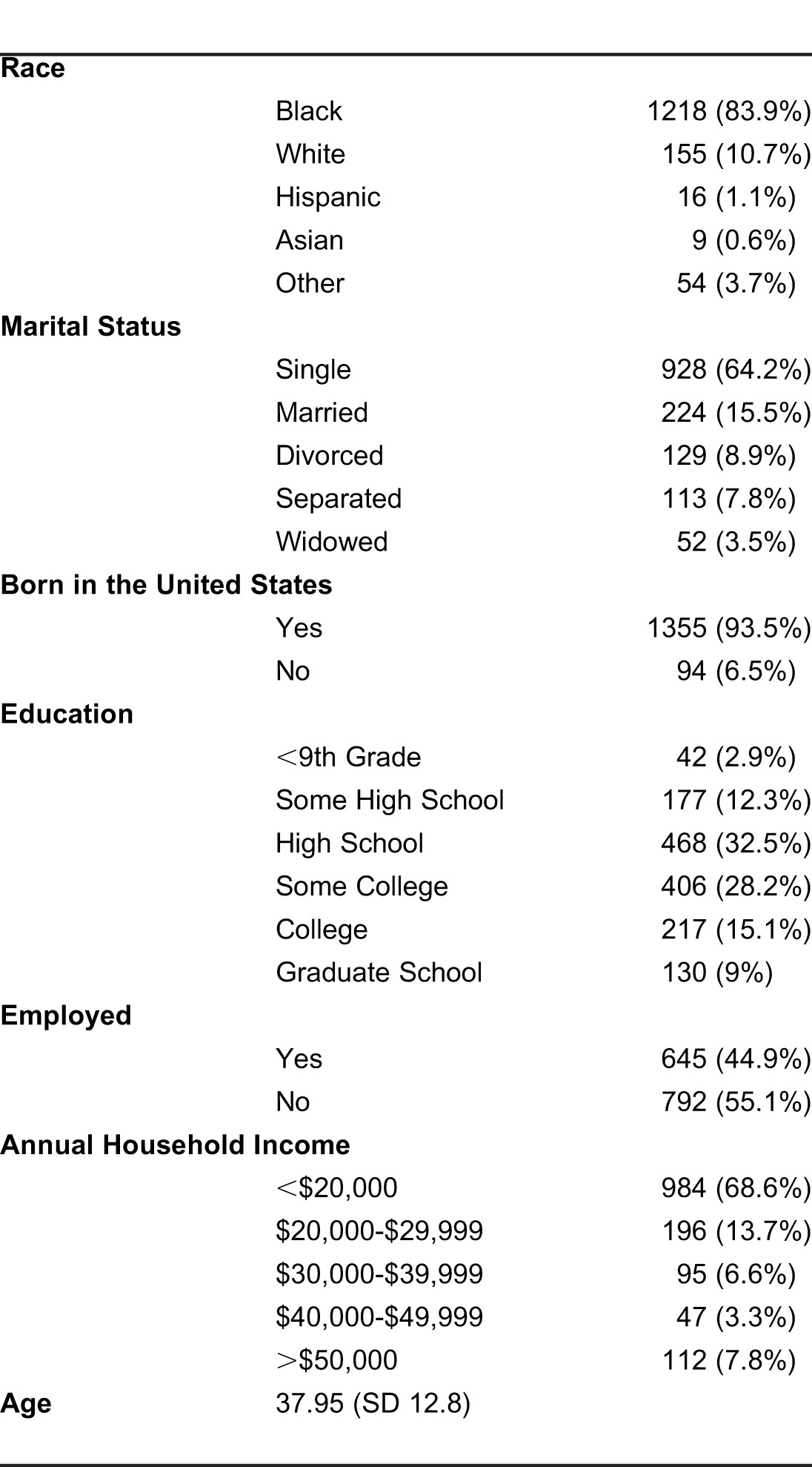
Our study sample was largely black (84%) and U.S.-born (94%). Most women were single (64%), and more than half were unemployed (55%). The average age of this sample was 38 years (SD 12.8). About half our sample had at least some college education (52.3%), and most women were poor, reporting an annual household income of less than $20,000 (69%). (Table 1)
Table 1.
Self-described demographic characteristics of study participants (n=1474).
Compared with nonvictims, IPV victims were about half as likely to wear seatbelts (OR=0.53, p=0.008), more than twice as likely to have access to a handgun (OR=2.27, p=0.002), and were 80% more likely to report daily consumption of unhealthy foods (OR=1.80, p=0.002). Women who screened positive for IPV were less likely than those with no IPV to have a working smoke alarm in their home, although this relationship was not statistically significant (OR=0.59, p=0.078). There was no significant relationship between IPV victimization and BMI, frequency of weekly exercise, or healthy food intake, although IPV victims were 23% less likely to endorse eating healthy foods on a daily basis (OR 0.77, p=0.158). (Table 2)
Table 2.
Frequencies (percentages) of health behaviors based on intimate partner violation victimization.

DISCUSSION
Women who experience IPV are more likely to engage in unhealthy behaviors; these findings show that women who experience IPV are at risk of adverse health outcomes from their increased negative health behaviors.
Women could be more likely to endorse negative health behaviors as a result of their increased stress from being IPV victims, resulting in having less time and effort to devote to eating healthy food. IPV has also been linked with depression, which can lead to decreased motivation to actively perform health behaviors, such as wearing a seatbelt and eating a healthy diet. 4 Additionally, when faced with the real and present threat of violence, avoiding seemingly less likely bodily injury through seatbelt use can have relatively decreased importance in the lives of IPV victims. The increased incidence of handgun access among IPV victims might be explained by their increased level of personal danger threat due to experienced violence. However, this finding is concerning given the increased risk of homicide for females by a partner when a gun is the home.7
While we found that IPV victims are more likely to endorse eating unhealthy foods everyday compared to nonvictims, these same women were no less likely to report eating healthy foods consistently than women who did not screen positive for IPV. An explanation for this finding could lie in the sample itself, a poor and urban population that likely does not have healthy eating habits at baseline. The BMIs between both groups were fairly similar, averaging just over 29 (which is widely considered to be at the end of the “overweight” spectrum, and close to the “obese” category), as were exercise habits, providing evidence for the argument that this population might not have healthy eating or exercise habits at baseline. The IPV victims who reported eating more unhealthy foods could be reacting to the increased stress in their lives by eating more “comfort” foods that might be unhealthy.
Violence and resulting increased stress have been linked to somatic disorders, such as fibromyalgia, chronic fatigue syndrome, and irritable bowel syndrome.8,9 Stress has similarly been linked to chronic diseases, such as cardiovascular disease, asthma, diabetes, and gastrointestinal disorders.8,10 It is widely accepted that certain health behaviors, such as poor diet and exercise, are related to higher risk of chronic diseases, such as obesity and hypertension; similarly, certain risk behaviors, such as not wearing a seatbelt, having a smoke alarm, and handgun access, put people at increased risk of personal injury. Subsequently, this study's demonstration of associations between IPV and certain negative health behaviors is concerning, as IPV already puts women at risk of chronic disease and personal injury, a risk which is further increased by adoption of unhealthy behaviors.
LIMITATIONS
This study is limited by using patients seeking care at EDs and not the general population. In addition, our patients were largely black and all the sites were in the same region. While this may limit generalizability, our findings provide data about a vulnerable population that is at particularly high risk for IPV and highlights the need for studying the health behaviors of other populations.
Another limitation is the use of a survey that relied on self-reported information. While previously validated survey instruments were used to address this limitation, data still could be misrepresented due to inaccurate recall or social desirability bias for self-reported measures, such as weight, diet, and exercise. Also, this cross-sectional study provides measures of association, but do not address causality; it is difficult to say whether the decreased adoption of health behaviors puts women at risk for IPV or vice versa. Finally, as this was a retrospective analysis of an existing dataset, the health behaviors we studied were limited to those initially surveyed. The survey did not assess frequency and context of IPV experienced, which could have influenced the association between IPV and certain health behaviors.
CONCLUSION
These findings highlight the need for interventions that identify and provide counseling for common health behaviors, particularly for women who disclose IPV. Adherence to these health behaviors can have a significant impact upon injury prevention and chronic disease development and progression. Healthcare providers should address the role of violence in women's lives and how it affects their ability to adhere to health maintenance regimens. Finally, future IPV interventions should focus on significant health behaviors, as well as ending abusive relationships when addressing the needs of women who experience IPV in order to improve their overall health outcomes.
Footnotes
Supervising Section Editor: Monica H. Swahn, PhD, MPH
Reprints available through open access at http://escholarship.org/uc/uciem_westjem
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. Funding for the initial study from which this analysis obtained its data was made possible by a grant from the Avon Foundation. The authors have no other conflicts of interest to disclose.
REFERENCES
- 1.Tjaden P, Thoennes N. Extent, nature, and consequences of intimate partner violence: findings from the National Violence Against Women Survey. National Institute of Justice and the Centers for Disease Control and Prevention. 2000 Jul; [Google Scholar]
- 2.Vest JR, Catlin TK, Chen JJ, et al. Multistate analysis of factors associated with intimate partner violence. Am J Prev Med. 2002;22:156–64. doi: 10.1016/s0749-3797(01)00431-7. [DOI] [PubMed] [Google Scholar]
- 3.Field CA, Caetano R. Ethnic differences in intimate partner violence in the US general population: the role of alcohol use and socioeconomic status. Trauma Violence Abuse. 2004;5:303–17. doi: 10.1177/1524838004269488. [DOI] [PubMed] [Google Scholar]
- 4.Bonomi A, Anderson M, Reid R, et al. Medical and psychosocial diagnoses in women with a history of intimate partner violence. Arch Intern Med. 2009;169:1692–7. doi: 10.1001/archinternmed.2009.292. [DOI] [PubMed] [Google Scholar]
- 5.Breiding M, Black M, Ryan G. Chronic disease and health risk behaviors associated with intimate partner violence - 18 US states/territories. Ann Epidemiol. 2005;18:538–44. doi: 10.1016/j.annepidem.2008.02.005. [DOI] [PubMed] [Google Scholar]
- 6.Heron S, Thompson M, Jackson E, et al. Do responses to an intimate partner violence screen predict scores on a comprehensive measure of intimate partner violence in low-income black women? Ann Emerg Med. 2003;42:483–91. doi: 10.1067/s0196-0644(03)00718-2. [DOI] [PubMed] [Google Scholar]
- 7.Bailey J, Kellermann A, Somes G, et al. Risk factors for violent death of women in the home. Arch Int Med. 1997;157:777–82. [PubMed] [Google Scholar]
- 8.Crofford L. Violence, stress, and somatic syndromes. Trauma Violence Abuse. 2007;8:299–313. doi: 10.1177/1524838007303196. [DOI] [PubMed] [Google Scholar]
- 9.Leserman J, Drossman D. Relationship of abuse history to functional gastrointestinal disorders and symptoms. Trauma Violence Abuse. 2007;8:331–43. doi: 10.1177/1524838007303240. [DOI] [PubMed] [Google Scholar]
- 10.Black P, Garbutt L. Stress, inflammation, and cardiovascular disease. J Psychosom Res. 2002;52:1–23. doi: 10.1016/s0022-3999(01)00302-6. [DOI] [PubMed] [Google Scholar]