

Abstract
Aims: To examine the influence of country-level characteristics and individual socio-economic status (SES) on individual alcohol-related consequences. Methods: Data from 42,655 men and women collected by cross-sectional surveys in 25 countries of the Gender, Alcohol and Culture: An International Study study were used. The individual SES was measured by the highest attained educational level. Alcohol-related consequences were defined as the self-report of at least one internal or one external consequence in the last year. The relationship between individuals’ education and alcohol-related consequences was examined by meta-analysis. In a second step, the individual level data and country data were combined in multilevel models. As country-level indicators, we used the purchasing power parity of the gross national income (GNI), the Gini coefficient and the Gender Gap Index. Results: Lower educated men and women were more likely to report consequences than higher educated men and women even after controlling for drinking patterns. For men, this relation was significant for both internal and external problems. For women, it was only significant for external problems. The GNI was significantly associated with reporting external consequences for men such that in lower income countries men were more likely to report social problems. Conclusion: The fact that problems accrue more quickly for lower educated persons even if they drink in the same manner can be linked to the social or environmental dimension surrounding problems. That is, those of fewer resources are less protected from the experience of a problem or the impact of a stressful life event.
INTRODUCTION
A variety of factors besides alcohol consumption can account for differences in prevalence rates of alcohol problems. These include: the social norms of alcohol use (Room and Mäkela, 2000), the level of case-finding and structural factors such as availability of public transportation (which could serve to reduce drinking and driving). An additional influence on the identification of alcohol-related problems and mental health problems in general is socio-economic status (SES). It is well known that those of lower SES are more likely to receive a psychiatric diagnosis than those of higher SES (Dohrenwend et al., 1992).
In high-income countries, drinking patterns tend to vary by SES. Those of higher SES are more likely to consume alcohol and tend to drink more frequently than those of lower status, but those of lower status who do drink consume more alcohol in total (e.g. Marmot, 1997; Van Oers et al., 1999; Bloomfield et al., 2000). Moreover, there is recent evidence from the USA that those with higher incomes are more likely to engage in hazardous drinking according to DSM-IV criteria (Keyes and Hasin, 2008). But when it comes to alcohol-related problems, drinkers of lower status consistently have a higher prevalence of problems than those of higher status (e.g. van Oers et al., 1999; Hasin et al., 2007). Furthermore, previous research has shown that given the same level of consumption, drinkers of lower SES experience more alcohol-related consequences than those of higher status (e.g. Mäkelä et al., 2003; Mäkelä and Paljärvi, 2008).
Others have focused on differences with respect to gender in alcohol problems (e.g. Plant et al., 2000; Wilsnack et al., 2000), variations in how society reacts to drinking and alcohol-related harms (Olafsdottír et al., 2009), drinking patterns (Bobak et al., 2004) and/or country development (e.g. Graham et al., 2011). Some have examined the relationship between the SES and alcohol-related problems internationally. A Brazilian study (Almeida-Filho et al., 2005) found that higher SES was associated with higher rates of dependence as well as consumption among both men and women. Among outpatients screened for alcohol dependence at a primary health-care clinic in Kampala, Uganda, differences by SES were found (Kullgren et al., 2009). And a recent study investigating alcohol use in Beijing found that those with lower education were more likely to receive a diagnosis of alcohol dependence than were those of higher education (Xiang et al., 2009).
Cook et al. (2011) examined scores on the Alcohol Use Disorders Identification Test (AUDIT) questionnaire in a representative sample of men in a Russian city. They found that the level of education, scores on an amenity index (having a car and/or central heating) and being employed were inversely associated with scores on the problem dimension of the AUDIT. Batty et al. (2011) investigated socio-economic disadvantage in relation to alcohol-related problems in a population-representative cohort in Western Scotland. They found that employment status, income, occupational class and car ownership were negatively associated with CAGE scores (Mayfield et al., 1974; Ewing, 1984) among men. Among women, the only significant result was that a higher CAGE score was associated with being employed. Bloomfield et al. (2006) examined social inequalities in scores on the AUDIT problem items in five European countries (Sweden, Finland, Switzerland, Czech Republic and Hungary). In Finland, the Czech Republic and Hungary, men of lower education were more likely to report problems than men of higher education. Among women only those of lower education in Finland reported a higher prevalence of problems.
Given these mixed results and the general lack of international comparative studies, it is a relevant question for the international alcohol health policy to examine the relationship of social inequalities to the prevalence of self-reported alcohol-related consequences among low- and middle-income countries as well as high-income countries. It is also important to examine social inequalities by gender since previous research suggests that the link between social status and alcohol-related problems differs between men and women. The present study examines the relationship between social status (measured as the relative educational attainment) and alcohol-related problems in 25 countries on the basis of surveys collected through the GENACIS project (Wilsnack et al., 2009).
Based on the literature to date and its complex and mixed evidence, we pose the following hypotheses:
- Drinkers of lower SES will have a higher prevalence of alcohol-related problems than those of higher SES;
- this relationship will persist even after controlling for alcohol consumption levels, and
- this relationship will hold across genders.
When taking country development into account, social inequalities in the prevalence of alcohol-related problems will be greater in higher-income countries.
METHODS
Survey data from 42,655 individuals in 25 countries participating in the GENACIS project were used (www.genacis.org). About 3.5% (n = 1642) of individuals had to be excluded from the analysis because of missing information on education or missing information about alcohol problems.
In 16 of the countries, the data come from national representative survey samples. In nine countries only regional data were available (Table 1). Additional details about the surveys and samples are reported elsewhere (Wilsnack et al., 2009). The age range was restricted to 25–69 years. For this study, we analysed data from drinkers, meaning only those who had consumed any alcohol in the past year. Data were collected between the years 1997 and 2007. The mean age of the respondents was 43.4 years (SD: 11.6) and 53.2% of the respondents were male.
Table 1.
Study countries by year of survey, number of individuals surveyed and GNI (in international USD)
| Country (ordered according to GNI) | Survey year | nb | GNI per capita, (2000) |
|---|---|---|---|
| Ugandaa | 2003 | 546 | 670 |
| Nigeriaa | 2003 | 608 | 1130 |
| Indiaa | 2003 | 407 | 1500 |
| Nicaraguaa | 2005 | 274 | 1780 |
| Sri Lankaa | 2002 | 306 | 2660 |
| Kazakhstana | 2002/3 | 682 | 4480 |
| Belize | 2005 | 1040 | 4630 |
| Costa Rica | 2003 | 458 | 6810 |
| Brazila | 2001/2 | 387 | 7730 |
| Argentina | 2003 | 656 | 8950 |
| Uruguay | 2004 | 535 | 8860 |
| Hungary | 2001 | 1435 | 14,640 |
| Czech Republic | 2002 | 1813 | 19,430 |
| New Zealand | 2007 | 1529 | 21,120 |
| Spaina | 2003 | 785 | 21,480 |
| Australiaa | 2007 | 869 | 24,920 |
| Finland | 2000 | 1148 | 25,470 |
| UK | 2000 | 1330 | 25,590 |
| Japan | 2001 | 1713 | 25,910 |
| Sweden | 2002 | 3531 | 27,500 |
| Canada | 2004 | 7783 | 27,630 |
| Iceland | 2001 | 1503 | 28,030 |
| Denmark | 2003 | 1490 | 28,180 |
| Switzerland | 1997 | 8187 | 34,020 |
| USA | 2000 | 3640 | 35,190 |
aRegional sampling frame employed.
bSample size based on drinkers with information about education and information about at least one of the consequence areas.
Individual-level indicators
As a measure of the individual's SES, we used the highest educational level the person achieved. The education variable from each country was recoded into a three-category variable based on years of schooling (low: ≤10 years; middle:>10 years and ≤13 years; high: bachelor, masters or equivalent). For the present analysis, these three categories were employed in the multilevel analyses. For the meta-analyses, the three groups were collapsed into two (low: ≤10 years of education and high: more than 10 years).
We used two versions of problem consequences scales constructed by Graham et al. (2011) which were based on a longer list of questions regarding alcohol-related problems in the GENACIS-study. We selected the five most commonly asked items from the first set of Graham et al. (2011). These represent consequences experienced by the individual including dependence symptoms. These items, asked in 25 countries, included questions on ‘guilt or remorse; unable to remember the night before; failing to do what was normally expected; unable to stop drinking once started; and needing a drink in the morning to get going after a heavy drinking session’.
The second grouping is composed of eight items that reflect the social or external problems related to drinking. The grouping includes harmful effects of drinking on: ‘finances; housework or chores around the house; work, studies or employment; marriage/intimate relationship; family relationships including children; and friendships or social life’. It also includes: ‘getting into a fight while drinking; the drinker himself/herself or someone else injured as a result of drinking’.
Regarding the latter item set, all eight questions were asked in 17 countries (Denmark, Canada, Japan, Australia, Spain, New Zealand, Czech Republic, Argentina, Uruguay, Costa Rica, Belize, Kazakhstan, Sri Lanka, Nicaragua, India, Nigeria and Uganda); seven of the eight items were asked in Brazil, UK and Sweden; six were asked in the USA. For each set, we constructed prevalence scores of one or more reported alcohol problems to be used in the analyses. In this paper, we refer to the first set of problems as ‘internal’ consequences and the latter set of problems as ‘external’ consequences (Bloomfield et al., 2010).
To control for alcohol consumption we created a drinking pattern variable to distinguish between four different groups of alcohol consumers:
moderate drinkers: those who are not monthly risky single occasion drinkers (RSOD) and not heavy drinkers (≤10/20 g of pure alcohol per day for women/men);
heavier drinkers (>10/20 g of pure alcohol for women/men per day);
monthly RSO drinkers and
those who are both: heavy drinkers and monthly RSO drinkers.
RSOD was defined differently for the different countries. For most countries, it is consuming 60 g or more of pure alcohol on one occasion. However, the range extends from 50 to 90 g of pure alcohol.
Additional control variables were gender and age.
Indicators on country level
To describe the socio-economic development of the countries, we chose purchasing power parity, a measure of gross national income (GNI) per capita in current international dollars (World Bank, 2008a, b), and the Gini coefficient, an indicator of income disparity within a country (United Nations Development Programme, 2002, 2007). With regard to gender equality, the Gender Gap Index (Hausmann et al., 2006) was chosen. To examine the relationship of each country-level indicator to drinking behaviour, we analysed each indicator separately, controlling for individual level factors. Later analyses tested all three country-level variables simultaneously in multivariate models.
Statistical analysis
In a first step, we calculated age-adjusted odds ratios (ORs) for the probability of reporting a problem for middle-or higher-level educated versus lower-level educated men or women by country. We combined the country-specific estimates according to the DerSimonian-Laird procedure (DerSimonian and Laird, 1986) (Figs. 1 and 2). The I2 statistic is the proportion of the total variation in the relation of alcohol-related problems and the SES that is due to heterogeneity between studies (Higgins et al., 2003; Higgins and Thompson, 2004). Although there can be no absolute rule for when heterogeneity becomes important, Higgins et al. (2003) suggest categories of ‘low’ for I2 values between 25 and 50%, ‘moderate’ for 50 and 75% and ‘high’ for ≥75%.
Fig. 1.

Age-adjusted ORs for middle and higher education versus lower education (drinkers only) men (left), women (right). Outcome: one or more internal consequences at least once in the past year.
Fig. 2.

Age-adjusted ORs for middle and higher education versus lower education (drinkers only) men (left), women (right). Outcome: one or more external consequences at least once in the past year.
In a second step, we combined individual-level and country-level analyses in a multilevel logistic model. In separate models, we first tested the relationship of the GNI, the Gini Index and the Gender Gap Index to alcohol-related consequences after adjusting for individual characteristics. In later models, we included all significant individual characteristics and the GNI simultaneously and tested also an interaction term for individual education and the GNI.
RESULTS
Table 1 displays survey characteristics and the GNI per capita for each country. Table 2 displays the percentages of people who reported at least one internal consequence or one external consequence by sex and educational level. When looking at external consequences, the prevalence tends to decrease as the GNI increases. The trend appears also for internal consequences, but is not as striking. For almost all countries, compared with their female counterparts with the same educational achievement, men are more likely than women to experience both types of problems.
Table 2.
Prevalences of at least one internal or one external consequence last year by gender, education and country
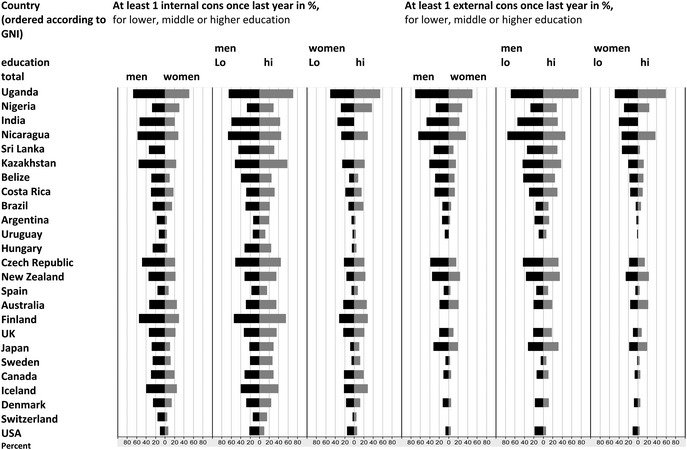 |
Figure 1 illustrates for each country the ORs of reporting at least one internal problem for higher educated men or women (compared with lower educated men or women). Lower educated men are more likely to report internal alcohol-related problems than men of higher education. The summary ORs for both low- to middle-income countries and high-income countries as well as the overall OR lie around 0.80. However, there is more variation in the relationship between education and alcohol problems among the low- to middle-income countries than in the high-income countries as indicated by the I2 statistic (63% for low- to upper-middle-income countries, 54% for higher-income countries). For women, educational status was not significantly associated with internal problems, although this relationship approached significance for high-income countries with a lower risk for women with higher education [OR: 0.87, 95% confidence interval (CI): 0.73–1.03].
Figure 2 displays ORs for the prevalence of external consequences among higher educated versus lower educated men and women, respectively. Again, lower educated men were significantly more likely to report external consequences than higher educated men. The summary ORs are 0.65 (95% CI: 0.47–0.90) for lower-income countries and 0.63 (95% CI: 0.52–0.77) for higher-income countries. Among the high-income countries, this result is relatively consistent (I2: 50%). Among the low- to middle-income countries, there is more variation in the relation between consequences and education (I2: 74%). For women, the results are in the same direction but the summary estimate in lower-income countries is not significant (OR: 0.92, 95% CI: 0.65–1.30). In high-income countries, it is more apparent that higher educated women reported less often external consequences than lower educated women (OR: 0.66, 95% CI: 0.52–0.84).
Table 3 displays the results of multilevel logistic regression when simultaneously examining individual and country-level predictors of reported internal or external problems. For internal problems, none of the country-level indicators was significant after adjusting for individual characteristics in the separate models. Even after adjusting for drinking patterns, lower educated men were more likely to report internal problems than higher educated men. At highest risk were men and women who were heavy consumers and monthly RSO drinkers. But those who were either ‘only’ heavy drinkers or monthly RSO drinkers were also at high risk. Younger persons were more likely overall to report internal problems. There was no interaction between individual education and country GNI with regard to internal alcohol-related problems.
Table 3.
Multilevel logistic models (random intercept) for at least one internal/external consequence item at least once in the past year, men and women separately, drinkers only, countries not included because of missing information about RSOD: Spain, UK, Sri Lanka
| Individual level | Internal problems |
External problems |
||||||
|---|---|---|---|---|---|---|---|---|
| Men (22 countries/20,364 cases) |
Women (22 countries/19,714 cases) |
Men (19 countries/15,195 cases) |
Women (19 countries/14,431 cases) |
|||||
| Separate modelsa OR (95% CI) | OR (95% CI) | Separate modelsa OR (95% CI) | OR (95% CI) | Separate modelsa OR (95% CI) | OR (95% CI) | Separate modelsa OR (95% CI) | OR (95% CI) | |
| Education (ref: high education) | ||||||||
| Low | 1.13 (1.02–1.26) | 1.11 (0.96–1.28) | 1.77 (1.54–2.04) | 1.45 (1.19–1.77) | ||||
| Middle | 1.07 (0.98–1.17) | 1.04 (0.93–1.17) | 1.32 (1.16–1.50) | 1.19 (1.01–1.41) | ||||
| Drinking pattern (ref: moderate) | ||||||||
| Monthly RSOD, not heavy drinking | 3.85 (3.51–4.23) | 4.30 (3.62–5.11) | 3.23 (2.86–3.66) | 3.95 (3.15–4.97) | ||||
| Heavy drinking (more than 10/20 g pure alcohol per day for women/men) | 3.02 (2.69–3.38) | 3.25 (2.87–3.68) | 2.87 (2.43–3.39) | 3.20 (2.67–3.82) | ||||
| Both: monthly RSOD and heavy drinking | 9.61 (8.70–10.60) | 13.41 (11.49–15.64) | 7.65 (6.80–8.61) | 12.08 (10.06–14.50) | ||||
| Age | ||||||||
| In decades (centred) | 0.75 (0.72–0.77) | 0.64 (0.62–0.67) | 0.79 (0.75–0.82) | 0.73 (0.69–0.78) | ||||
| Age squared | — | — | — | — | ||||
| Country level | ||||||||
| GNI (in 10,000$) | 0.88 (0.69–1.13) | 0.88 (0.69–1.13) | 0.96 (0.70–1.31) | 0.96 (0.70–1.31) | 0.66 (0.48–0.90) | 0.66 (0.48–0.90) | 0.73 (0.49–1.09) | 0.73 (0.49–1.09) |
| Gini Index (in 10) | 0.82 (0.61–1.09) | — | 0.81 (0.57–1.16) | — | 1.08 (0.70–1.64) | 0.92 (0.56–1.50) | — | |
| Gender Gap Index | 1.39 (0.83–2.34) | — | 1.74 (0.94–3.22) | — | 0.95 (0.88–1.02) | 0.96 (0.87–1.04) | — | |
| Cross-level interaction | ||||||||
| Low education × GNI (in 10,000$) | — | — | — | — | ||||
| Variance between countries | Beta (SE) | Beta (SE) | Beta (SE) | Beta (SE) | ||||
| 0.47 (0.15) | 0.70 (0.23) | 0.63 (0.22) | 1.00 (0.37) | |||||
aAdjusted for individual characteristics.
In countries of higher economic power men reported less often external consequences than men in countries of lower economic power even after adjusting for individual characteristics (as indicated by the significant coefficient of the GNI). For women this relation was not significant. After controlling for age and drinking patterns, both men and women of lower educational attainment were more likely to report external consequences than their higher educated counterparts. As in the regression for internal problems, those who engaged in both monthly RSOD and heavy drinking were at greatest risk followed by those who ‘only’ engage in monthly RSO drinking or ‘only’ in heavy drinking. Moderate drinkers had the lowest prevalence of reporting at least one external consequence. Younger persons were more likely to report external problems. There was no interaction between individual education and country GNI with regard to external alcohol-related problems.
DISCUSSION
This paper has examined social inequalities in the prevalence of self-reported alcohol consequences from a gender and international perspective. We have separately examined ‘internal’ and ‘external’ consequences of alcohol.
The fact that more men report problems than women given similar drinking patterns has been established in previous work of this study group (Bond et al., 2010; Graham et al., 2011). With specific regard to our first hypothesis, multilevel analyses revealed that in relation to internal problems, lower educated men were more likely to report internal problems than higher educated men even if they drank in the same manner. Likewise with external problems, lower educated men and also lower educated women were more likely to report consequences than higher educated men and women, even if they drank similarly. After adjusting for drinking patterns, the GNI was significantly associated with reporting external consequences for men such that, in countries with a lower GNI, men in general were more likely to report external problems than men in countries of higher GNI. Thus, our findings support our first hypothesis and sub-hypotheses to a large extent, that is, that those of a lower SES will report more alcohol-related problems even after controlling for level of consumption and that this holds for both genders (except reporting of internal problems among women).
The fact that problems accrue more quickly for lower educated persons could be linked to the social or environmental dimension surrounding both categories of problems, especially for external problems which, by definition, include interactions with the social environment. Previous research has demonstrated that those of fewer resources are less protected from the experience of a problem or the impact of a stressful life event (Thoits, 1982, 2010). Further, it has been shown that those of a lower SES are more likely to be exposed to sources of chronic stress which can accumulate over the life course (Baum et al., 1999; Hatch and Dohrenwend, 2007; Kopp et al., 2007). This, in turn, can lead to the increased likelihood of substance abuse and addiction (Cleck and Blendy, 2008; Hyman and Sinha, 2009; Enoch, 2010).
Our second hypothesis predicting that a social gradient would be stronger in higher income countries was not supported. Cross-level interactions of individual education and country-level economic indicators were not significantly associated with the reporting of problems. Moreover, it was countries of lower GNI that were more likely to report a higher prevalence of external problems among men after adjusting for drinking patterns. This finding, again, may well be related to a lack of resources that buffer a person from the negative external consequences of alcohol use.
The present study provides information about the relationship between educational achievement, alcohol consumption and negative consequences among drinkers from a diverse group of countries around the world. However, there are also some limitations. Firstly, some countries employed only regional samples; therefore, these results cannot necessarily be considered representative of countries (see http://www.genacis.org/overviews/overview_sampling_design.pdf for details). Secondly, all survey sampling methods have some selection bias, e.g. women were more likely than men to participate. For telephone surveys, persons who were institutionalized or did not feel comfortable speaking the language(s) of the country were generally not included. For the prevalence of external problems, we also included countries that had not included all questions from the complete item set. The overall estimates should be interpreted with caution in the light of the heterogeneity among the country-specific ORs regarding the relationship of education to problems (Fig. 2: I2 statistics). This is especially the case for men in lower-income countries.
In sum, our analyses reveal that those of lower educational achievement—especially men—appear to be more at risk of reporting negative alcohol consequences and this appears to occur generally regardless of drinking patterns. Additionally, our results point to a higher prevalence of external problems among men in lower-income countries. Policy-makers should take this information into account when formulating and specifying future national and international alcohol policy strategies.
Funding
Support for aspects of the project comes from the World Health Organization, the Quality of Life and Management of Living Resources Programme of the European Commission (Concerted Action QLG4-CT-2001-0196), the U.S. National Institute on Alcohol Abuse and Alcoholism/National Institutes of Health (grants R21 AA012941 and R01 AA015775), the German Federal Ministry of Health, the Pan American Health Organization and Swiss national funds. Support for individual country surveys was provided by government agencies and other national sources. The study leaders and funding sources for data sets used in this report are: Argentina: Myriam Munné, M.S., World Health Organization; Australia: Paul Dietze, Ph.D., National Health and Medical Research Council (grant 398500); Belize: Claudina Cayetano,M.D., Pan American Health Organization; Brazil: Florence Kerr-Corréa, M.D., Ph.D., Foundation for the Support of Sao Paulo State Research (Fundação de Amparo a Pesquisa do Estado de São Paulo, FAPESP) (grant 01/03150-6); Canada: K.G., Ph.D., Canadian Institutes of Health Research (CIHR); Costa Rica: Julio Bejarano, M.Sc., World Health Organization; Czech Republic: Ladislav Csémy, Ph.D., Ministry of Health (grant MZ 23752); Denmark: Kim Bloomfield, Dr P.H., Sygekassernes Helsefond, Danish Medical Research Council; Finland: Pia Mäkelä, Ph.D., National Institute for Health and Welfare (THL); Great Britain: Martin Plant, Ph.D. and Moira Plant, Ph.D., Alcohol Education and Research Council, European Forum for Responsible Drinking, University of the West of England, Bristol; Hungary: Zsuzsanna Elekes, Ph.D., Ministry of Youth and Sport; Iceland: Hildigunnur Ólafsdóttir, Ph.D., Alcohol and Drug Abuse Prevention Council, Public Health Institute of Iceland, Reykjavík, Iceland; India: Vivek Benegal, M.D.,World Health Organization; Japan: Shinji Shimizu, Ph.D., Japan Society for the Promotion of Science (grant 13410072); Kazakhstan: Bedel Sarbayev, Ph.D., World Health Organization; New Zealand: Jennie Connor, Ph.D., Otago University Research Grant; Nicaragua: José Trinidad Caldera Aburto, M.D., Ph.D., Pan American Health Organization; Nigeria: Akanidomo Ibanga, M.Sc., World Health Organization; Spain: Juan Carlos Valderrama, M.D., Dirección General de Atención a la Dependencia, Conselleria de Sanidad, Generalitat Valenciana; Comisionado do Plan de Galicia sobre Drogas, Conselleria de Sanidade, Xunta de Galicia; Dirección General de Drogodependencias y Servicios Sociales, Gobierno de Cantabria; Sri Lanka: Siri Hettige, Ph.D., World Health Organization; Sweden: Karin Helmersson Bergmark, Ph.D., Ministry for Social Affairs and Health, Sweden; Switzerland: Gerhard Gmel, Ph.D., Swiss Federal Office for Education and Science (Contract 01.0366); Swiss Federal Statistical Office; University of North Dakota (Subcontract no. 254, Amendment No.2, UND Fund 4153- 0425); Uganda: M. Nazarius Tumwesigye, Ph.D., World Health Organization; USA: Thomas Greenfield, Ph.D., National Institute on Alcohol Abuse and Alcoholism/ National Institutes of Health (grant P50 AA05595); Uruguay: Raquel Magri, M.D., World Health Organization.
Acknowledgements
The data used in this paper are from the project, Gender, Alcohol and Culture: An International Study (GENACIS). GENACIS is a collaborative international project affiliated with the Kettil Bruun Society for Social and Epidemiological Research on Alcohol and coordinated by GENACIS partners from the University of North Dakota, Aarhus University, the Alcohol Research Group/Public Health Institute, the Centre for Addiction and Mental Health, the University of Melbourne and the Swiss Institute for the Prevention of Alcohol and Drug Problems. We thank Gerhard Gmel, Richard Wilsnack, Ludek Kubicka, the anonymous reviewers and the editor Jonathan Chick for their careful read and thoughtful comments on previous draft.
References
- Almeida-Filho N, Lessa I, Magalhaes L, et al. Social inequality and alcohol consumption-abuse in Bahia, Brazil—interactions of gender, ethnicity and social class. Soc Psychiatry Psychiatr Epidemiol. 2005;40:214–22. doi: 10.1007/s00127-005-0883-4. [DOI] [PubMed] [Google Scholar]
- Batty GD, Bhaskar A, Emslie C, et al. Association of life course socioeconomic disadvantage with future problem drinking and heavy drinking: gender differentials in the west of Scotland. Int J Public Health. 2011 doi: 10.1007/s00038-011-0270-8. Published online 03 July 2011, DOI 10.1007/s00038-011-0270-8. [DOI] [PubMed] [Google Scholar]
- Baum A, Garofalo AP, Yali AM. Socioeconomic status and chronic stress: does stress account for SES effects on health? Ann N Y Acad Sci. 1999;896:131–44. doi: 10.1111/j.1749-6632.1999.tb08111.x. [DOI] [PubMed] [Google Scholar]
- Bloomfield K, Augustin R, Kraus L. Social inequalities in alcohol use and misuse in the German general population. Zeitschrift für Gesundheitswissenschaften. 2000;8:230–42. [Google Scholar]
- Bloomfield K, Grittner U, Kramer S, et al. Social inequalities in alcohol consumption and alcohol-related problems in the study countries of the EU concerted action ‘gender and alcohol problems: a multi-national study’. Alcohol Alcohol Suppl. 2006;41:i26–i36. doi: 10.1093/alcalc/agl073. [DOI] [PubMed] [Google Scholar]
- Bloomfield K, Wicki M, Gustafsson N-K, et al. Changes in alcohol-related problems after alcohol policy changes in Denmark, Finland and Sweden. J Stud Alcohol Drugs. 2010;71:32–40. doi: 10.15288/jsad.2010.71.32. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bobak M, Room R, Pikhart H, et al. Contribution of drinking patterns to differences in rates of alcohol related problems between three urban populations. J Epidemiol Community Med. 2004;58:238–42. doi: 10.1136/jech.2003.011825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bond J, Greenfield T, Roberts SCM, et al. 36th Annual Epidemiological Symposium of the Kettil Bruun Society for Social and Epidemiological Study of Alcohol. .; Alcohol consumption and alcohol-related problems: a cross-national multilevel GENACIS analysis; 31 May–1 June 2010; Lausanne, Switzerland. 2010. [Google Scholar]
- Cleck JN, Blendy JA. Making a bad thing worse: adverse effects of stress on drug addiction. J Clin Invest. 2008;118:454–61. doi: 10.1172/JCI33946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cook S, De Stavola B, Saburova L, et al. Socio-demographic predictors of dimensions of the AUDIT score in a population sample of working-age men in Izhevsk, Russia. Alcohol Alcohol. 2011 doi: 10.1093/alcalc/agr076. Published online 03 July 2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials. 1986;7:177–88. doi: 10.1016/0197-2456(86)90046-2. [DOI] [PubMed] [Google Scholar]
- Dohrenwend BP, Levav I, Shrout PE, et al. Socioeconomic status and psychiatric disorders: the causation-selection issue. Science. 1992;255:946–52. doi: 10.1126/science.1546291. [DOI] [PubMed] [Google Scholar]
- Enoch MA. The role of early life stress as a predictor for alcohol and drug dependence. Psychopharmacology (Berl.) 2010;214:17–31. doi: 10.1007/s00213-010-1916-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ewing J. Detecting alcoholism: the CAGE questionnaire. J Am Med Assoc. 1984;252:1905–7. doi: 10.1001/jama.252.14.1905. [DOI] [PubMed] [Google Scholar]
- Graham K, Bernards S, Knibbe R, et al. Alcohol-related negative consequences among drinkers around the world. Addiction. 2011;106:1391–405. doi: 10.1111/j.1360-0443.2011.03425.x. doi:10.1111/j.1360-0443.2011.03425.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hasin DS, Stinson FS, Ogburn E, et al. Prevalence, correlates, disability and comorbidity of DSM-IV alcohol abuse and dependence in the United States: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Arch Gen Psych. 2007;64:830–42. doi: 10.1001/archpsyc.64.7.830. [DOI] [PubMed] [Google Scholar]
- Hatch SL, Dohrenwend BP. Distribution of traumatic and other stressful life events by race/ethnicity, gender SES and AGE: A review of the research. Am J Community Psychol. 2007;40:313–32. doi: 10.1007/s10464-007-9134-z. [DOI] [PubMed] [Google Scholar]
- Hausmann R, Tyson LD, Zahidi S. Geneva: World Economic Forum; 2006. THE Global Gender Gap Report 2006. [Google Scholar]
- Higgins JP, Thompson SG. Controlling the risk of spurious findings from meta-regression. Stat Med. 2004;23:1663–82. doi: 10.1002/sim.1752. [DOI] [PubMed] [Google Scholar]
- Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. Br Med J. 2003;327:557–60. doi: 10.1136/bmj.327.7414.557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hyman SM, Sinha R. Stress-related factors in cannabis use and misuse: implications for prevention and treatment. J Substance Abuse Treatment. 2009;36:400–13. doi: 10.1016/j.jsat.2008.08.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keyes KM, Hasin DS. Socio-economic status and problem alcohol use: the positive relationship between income and the DSM-IV alcohol abuse diagnosis. Addiction. 2008;103:1120–30. doi: 10.1111/j.1360-0443.2008.02218.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kullgren G, Alibusa S, Birabwa-Oketcho H. Problem drinking among patients attending primary healthcare units in Kampala, Uganda. Afr J Psychiatry (Johannesbg.) 2009;12:52–8. doi: 10.4314/ajpsy.v12i1.30279. [DOI] [PubMed] [Google Scholar]
- Mäkelä P, Paljärvi T. Do consequences of a given pattern of drinking vary by socioeconomic status? A mortality and hospitalisation follow-up for alcohol-related causes of the Finnish Drinking Habits Survey. J Epidemiol Community Health. 2008;62:728–33. doi: 10.1136/jech.2007.065672. [DOI] [PubMed] [Google Scholar]
- Mäkelä P, Jansson M, Keskimäki I, et al. What underlies the high alcohol-related mortality of the disadvantaged: high morbidity or poor survival? J Epidemiol Community Health. 2003;57:981–6. doi: 10.1136/jech.57.12.981. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marmot M. Inequality, deprivation and alcohol use. Addiction. 1997;92(Suppl):13–20. [PubMed] [Google Scholar]
- Mayfield D, Mcleod G, Hall P. The CAGE questionnaire: validation of a new alcoholism screening instrument. Am J Psychiatry. 1974;131:1121–3. doi: 10.1176/ajp.131.10.1121. [DOI] [PubMed] [Google Scholar]
- Olafsdottír H, Raitasalo K, Greenfield T, et al. Concern about family members’ drinking and cultural consistency: a Multi-Country GENACIS study. Contemp Drug Probl. 2009;36:59–83. [PMC free article] [PubMed] [Google Scholar]
- Plant M, Miller P, Thornton C, et al. Life stage, alcohol consumption patterns, alcohol-related consequences and gender. Subst Abuse. 2000;21:265–81. doi: 10.1080/08897070009511438. [DOI] [PubMed] [Google Scholar]
- Room R, Mäkela K. Typologies of the cultural position of drinking. J Stud Alcohol. 2000;61:475–83. doi: 10.15288/jsa.2000.61.475. [DOI] [PubMed] [Google Scholar]
- Thoits PA. Conceptual, methodological, and theoretical problems in studying social support as a buffer against life stress. J Health Soc Behav. 1982;23:145–59. [PubMed] [Google Scholar]
- Thoits PA. Stress and health: major findings and policy implications. J Health Soc Behav. 2010;51(Suppl):S41–53. doi: 10.1177/0022146510383499. [DOI] [PubMed] [Google Scholar]
- United Nations Development Programme. New York: Oxford University Press; 2002. Human Development Report 2002—Deepening democracy in a fragmented world. [Google Scholar]
- United Nations Development Programme. New York: Oxford University Press; 2007. Human Development Report 2007/2008—Fighting climate change: human solidarity in a divided world. [Google Scholar]
- Van Oers JA, Bongers IM, van de Goor LA, et al. Alcohol consumption, alcohol-related problems, problem drinking, and socioeconomic status. Alcohol Alcohol. 1999;34:78–88. doi: 10.1093/alcalc/34.1.78. [DOI] [PubMed] [Google Scholar]
- Wilsnack R, Vogeltanz N, Wilsnack S, et al. Gender differences in alcohol consumption and adverse drinking consequences : cross-cultural patterns. Addiction. 2000;95:251–65. doi: 10.1046/j.1360-0443.2000.95225112.x. [DOI] [PubMed] [Google Scholar]
- Wilsnack RW, Wilsnack SC, Kristjanson AF, et al. Gender and alcohol consumption: patterns from the multinational GENACIS project. Addiction. 2009;104:1487–500. doi: 10.1111/j.1360-0443.2009.02696.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- World Bank. International comparison program. 2008a. http://databank.worldbank.org/ddp/home.do?Step=2&id=4&DisplayAggregation=Y&SdmxSupported=N&CNO=1009&SET_BRANDING=YES#. [On-line]
- World Bank. World Development Indicators and Global Development Finance. 2008b. http://databank.worldbank.org/ddp/viewClassifications?HIERARCHY=Classification&DIMENSION=WDI_Ctry. [On-line]
- Xiang YT, Ma X, Lu JY, et al. Alcohol-related disorders in Beijing, China: prevalence, socio-demographic correlates, and unmet need for treatment. Alcohol Clin Exp Res. 2009;33:1111–8. doi: 10.1111/j.1530-0277.2009.00933.x. [DOI] [PubMed] [Google Scholar]