

Abstract
Context:
Excessive knee valgus during dynamic tasks is thought to contribute to lower extremity overuse and traumatic injuries. Clinically, assessments of frontal-plane knee motion typically include measures of the distance between the knees during landing. However, it is not clear how this clinical assessment relates to knee-abduction angle or how it is influenced by the position of the lower extremities in the transverse and frontal planes.
Objective:
To determine whether normalized knee separation distance (NKSD) is a predictor of knee-abduction angles and to assess the influence of lower extremity transverse-plane and frontal-plane angles on NKSD during a drop land.
Design:
Cross-sectional study.
Setting:
Motion analysis laboratory.
Patients or Other Participants:
Twenty-five healthy female athletes.
Intervention(s):
The frontal-plane distance between the 2- dimensional coordinates of markers over the greater trochanters (intertrochanteric distance), lateral femoral epicondyles (knee separation distance), and lateral malleoli (stance width) bilaterally was calculated during a drop land. The knee separation distance was normalized by intertrochanteric distance (NKSD). Concurrently, 3-dimensional lower extremity transverse-plane and frontal-plane kinematics were obtained.
Main Outcome Measure(s):
We assessed NKSD, stance width, and bilateral average knee and hip transverse plane and frontal-plane angles and ankle frontal-plane angles. Linear regression was used to determine the association between NKSD and bilateral average knee frontal-plane angles. Stepwise multiple regression was used to identify the best predictors of NKSD during the drop land.
Results:
After we controlled for stance width, NKSD explained 52% of the variance in the knee frontal-plane angle. When we took lower extremity kinematics into account, after controlling for stance width, the average hip frontal-plane angle was the best predictor of NKSD, explaining 97% of the variance.
Conclusions:
Although NKSD is a predictor of knee- abduction angle, frontal-plane hip angle and stance width are strongly related to NKSD. Caution must be taken when interpreting NKSD as knee abduction.
Keywords: anterior cruciate ligament injuries, injury prevention, screening, lower limb alignment
Key Points.
Assessment techniques measuring knee separation distance during a bilateral landing task can provide useful information about the frontal-plane posture of the lower extremities.
When associating these measures with knee-abduction angles, one must keep in mind that frontal-plane hip angle and stance width are strongly related to knee separation distance.
Excessive knee valgus during dynamic tasks is thought to contribute to lower extremity overuse and traumatic injuries.1–3 Observational assessments have been found to be only moderately reliable4 and sensitive,5 so objective assessment techniques have been developed to screen for excessive frontal- plane knee motion during dynamic tasks.5–7 Three-dimensional (3-D) motion analysis techniques are the gold standard for quantifying lower extremity joint motion during dynamic tasks. However, because these assessments are time consuming and require expensive equipment, alternative screening methods have been developed. In particular, techniques assessing the extent to which the knees collapse medially during landing have been adopted clinically and used in several research studies.6,8–11 The distance between the knees is thought to reflect the degree to which the knees move medially and, in turn, knee frontal-plane motion. Although this method has been used to identify sex differences8 and to assess the effects of training,6 the relationship of the distance between the knees in the frontal- plane and knee-abduction angle is not clear.
The use of 2-dimensional (2-D) measures of knee-abduction angle during dynamic tasks to screen for excessive motion is supported by previous studies. Moderate correlations between 2-D and 3-D knee-abduction angles suggest that less expensive 2-D techniques may be adequate for screening.12,13 However, these authors used a 2-D technique that measured the angle between the lines formed by points representing the hip and knee joint centers and the knee and ankle joint centers from digitized still frames. In contrast to these methods, knee separation distance is commonly measured as the distance between single points on the knees in the frontal plane. Data relating knee separation distance and knee-abduction angle are needed to support the use of this technique for clinical screening. Therefore, the primary aim of our study was to determine whether 2-D measures of knee separation distance can predict knee-abduction angles identified with 3-D motion analysis during a drop land.
Two-dimensional kinematic assessments are limited by their inability to capture out-of-plane movement. During landing, frontal-plane motion at the knee is influenced primarily by frontal-plane movement at the hip and ankle. However, knee and hip joint rotations in the transverse plane are thought to influence 2-D frontal-plane angle projections.14 For example, hip internal rotation is thought to project on the frontal plane and appear as knee valgus in 2-D measures.12,13 Therefore, an appreciation of the relationship between the frontal-plane and trans-verse-plane angles of the lower extremities and knee separation distance is important for interpreting the results of clinical screenings. The secondary aim of our study was to determine the best predictors of knee separation distance when considering hip, knee, and ankle frontal-plane angles and hip and knee transverse-plane angles during a drop land.
Given that 2-D measures of knee-abduction angles are correlated with 3-D knee-abduction angles, we hypothesized that 2-D measures of normalized knee separation distance (NKSD) would predict bilateral knee-abduction angles. In addition to knee frontal-plane angles, hip frontal-plane and transverse-plane angles and ankle frontal-plane angles are believed to-contribute to 2-D measures of NKSD, so we hypothesized that these angles would correlate with NKSD and that the best predictors of NKSD would be knee frontal-plane and hip frontal-plane and transverse-plane angles.
METHODS
Participants
Twenty-five female soccer players between the ages of 11 and 23 years (age = 16.5 ± 3.8 years, height = 162.4 ± 7.7 cm, mass = 57.7 ± 10.6 kg) participated in this study. Volunteers were healthy with no history of previous knee injury. Exclusion criteria were history of previous lower extremity surgery; previous injury that resulted in ligamentous laxity at the ankle, hip, or knee; or presence of any medical or neurologic condition that would impair the ability to perform athletic maneuvers. Before participation, all procedures were explained to each person, and informed consent and parental assent were obtained as required by the Investigational Review Board for University Health Sciences Campus, which approved the study.
Instrumentation
Kinematic data were collected using an 8-camera 3-D motion analysis system (Vicon 612; Oxford Metrics Ltd, Oxford, United Kingdom) at a sampling frequency of 250 Hz. The cameras were interfaced to a microcomputer and placed around a force plate (model OR6-6-1; Advanced Mechanical Technologies, Inc, Newton, MA) embedded in the floor. The force plate (1500 Hz) was interfaced to the same microcomputer used for kinematic data collection via an analog-to-digital converter, allowing synchronization of kinematic and force-plate data. The force-plate data were used in this study to identify foot contact during the drop land.
Reflective markers (14-mm spheres) were placed bilaterally over the first and fifth metatarsal heads, medial and lateral malleoli, medial and lateral femoral epicondyles, greater trochanters, and iliac crests. A single marker was placed on the joint space between the fifth lumbar and the first sacral spinous processes. In addition, triads of rigid reflective tracking markers were securely placed bilaterally on the lateral surfaces of the participant's thigh, leg, and heel counter of the shoe. To control for the potential influence of different types of footwear, participants were fitted with the same style of cross-training shoe (New Balance, Inc, Boston, MA).
Procedures
Testing took place in the Jacquelin Perry Musculoskeletal Biomechanics Research Laboratory at the University of Southern California. Participants stepped off a 36-cm platform (leading with the dominant limb, which was identified by asking the participant which leg she would use to kick a ball), landed on both feet, and immediately performed a maximum vertical jump.8,9 They were not given any verbal cues for landing or jumping technique. Four practice trials were allowed for familiarization of procedures and instrumentation, and 3 trials were collected for analysis.
Data Analysis
Coordinate data were digitized in Vicon Workstation software (Oxford Metrics Ltd). Kinematic data were filtered using a fourth-order, zero-lag Butterworth 12-Hz low-pass filter. Visual3D software (version 3.90; C-Motion, Inc, Rockville, MD) was used to quantify 3-D ankle, knee, and hip kinematics. Joint kinematics were calculated using a joint coordinate system approach14 and were reported relative to a static standing trial. During the dynamic trials, the positions of the right and left greater trochanter, lateral epicondyle, and lateral malleolus markers were recreated based on the original position of the markers in the static trial.
The landing cycle was identified as the period from foot contact to toe-off, as determined by vertical ground reaction force values greater than and equal to 10 N, respectively. We studied only the deceleration phase of the drop land because this phase is most commonly evaluated during clinical assessments.7,9 The deceleration phase was defined as foot contact to peak knee flexion.
Knee separation distance was quantified using previously described methods.9,11 Using 2-D coordinates, we defined knee separation distance as the distance (in centimeters) between the right and left lateral femoral epicondyle markers in the frontal plane. In addition, stance width and intertrochanteric distance were defined as the distances (in centimeters) between the right and left lateral malleolus and the greater trochanter markers in the frontal plane, respectively (Figure). To account for the effects of body type, knee separation distance was normalized to intertrochanteric distance.8 The smallest distance between the femoral epicondyle markers (minimum NKSD) was used for analysis.
Figure.
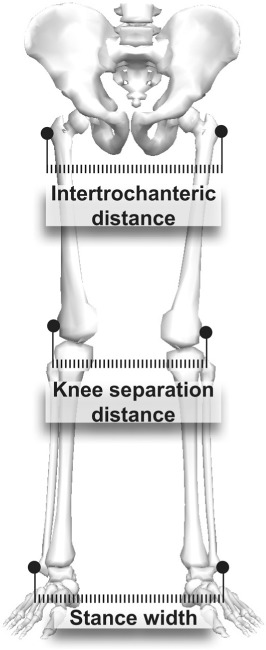
Using 2-dimensional coordinates, intertrochanteric distance was defined as the distance between the right and left greater trochanter markers; knee separation distance was defined as the distance between the right and left lateral femoral epicondyle markers; and stance width was defined as the distance between the right and left lateral malleolar markers in the frontal plane.
Stance width and lower extremity transverse-plane and frontal-plane angles bilaterally were identified at the time of minimum NKSD. Right and left angular data were averaged to account for the contribution from each lower extremity to the knee separation distance. Data were averaged across 3 trials for each participant.
Statistical Analysis
To determine whether 2-D measures of NKSD predicted bilateral average knee-abduction angles, we used a simple linear regression model. Next, Pearson product correlations were calculated to determine whether a relationship existed between the independent variables (bilateral average knee and hip frontal-plane and transverse-plane and ankle frontal-plane angles) and NKSD. To identify the best predictors of NKSD during a drop land, we considered the independent variables that were significantly correlated with NKSD in a stepwise multiple regression model (entry and removal thresholds of P ≤ .05 and P ≥ .10, respectively). To control for the effects of foot position, we considered stance width an independent variable first in both of the regression models. Statistical analyses were performed using SPSS software (version 15; SPSS Inc, Chicago, IL). Significance levels were set at P ≤ .05.
RESULTS
Kinematic data at the time of minimum knee separation distance are presented in Table 1. Average knee separation distance normalized to intertrochanteric width was 0.89 ± 0.15 (range, 0.68 to 1.26). After we accounted for stance width, NKSD explained 52% of the variance in bilateral average knee-abduction angle (R2 = 0.52, P < .001). Stance width, entered into the model to account for the effects of foot position, did not significantly contribute to the model (R2 = 0.02, P = .56). Together, these variables explained 53% of the variance in bilateral knee-abduction angle (R2 = 0.53, P < .001).
Table 1.
Kinematic Data at the Time of Minimum Normalized Knee Separation Distance, °
| Anglea | Minimum | Maximum | Mean ± SD |
| Knee | |||
| Frontal planeb | −5.4 | 12.9 | 3.2 ± 4.0 |
| Transverse planec | −12.7 | 5.0 | −4.1 ± 4.9 |
| Hip | |||
| Frontal plane | −4.9 | 13.6 | 1.2 ± 4.5 |
| Transverse plane | −7.8 | 6.0 | −0.8 ± 3.8 |
| Ankle | |||
| Frontal plane | −5.8 | 7.4 | 0.5 ± 3.7 |
a Values represent average angular data from the right and left limbs.
b Frontal-plane angles: (+) = abduction, (−) = adduction.
c Transverse-plane angles: (+) = internal rotation, (−) = external rotation.
The Pearson correlations are presented in Table 2. Bilateral average hip and knee frontal-plane angles were correlated with NKSD. A significant positive correlation was found between bilateral average hip frontal-plane angles and NKSD (r = 0.98, P < .001). A significant negative correlation was found between bilateral average knee frontal-plane angles and NKSD (r = −0.67, P < .001). Knee transverse-plane, hip transverse-plane, and ankle frontal-plane angles did not correlate significantly with NKSD (P > .05).
Table 2.
Univariate Correlations Between Variables of Interest
| Normalized Knee Separation Distance | Stance Width | Knee Frontal-Plane Angle | Knee Transverse-Plane Angle | Hip Frontal-Plane Angle | Hip Transverse-Plane Angle | Ankle Frontal-Plane Angle | |
| Normalized knee separation distance | . . . | 0.558, P = .004 | −0.665, P < .001 | 0.157, P = .453 | 0.982, P < .001 | −0.262, P = .207 | 0.113, P = .592 |
| Stance width | 0.558, P = .004 | . . . | −0.124, P = .555 | −0.008, P = .969 | 0.594, P = .002 | 0.005, P = .980 | 0.593, P = .002 |
| Knee frontal-plane angle | −0.665, P < .001 | −0.124, P = .555 | . . . | −0.188, P = .368 | −0.643, P = .001 | −0.171, P = .415 | 0.084, P = .690 |
| Knee transverse-plane angle | 0.157, P = .453 | −0.008, P = .969 | −0.188, P = .368 | . . . | 0.148, P = .481 | 0.289, P = .162 | −0.400, P = .047 |
| Hip frontal-plane angle | 0.982, P < .001 | 0.594, P = .002 | −0.643, P = .001 | 0.148, P = .481 | . . . | −0.289, P = .161 | 0.158, P = .452 |
| Hip transverse-plane angle | −0.262, P = .207 | 0.005, P = .980 | −0.171, P = .415 | 0.289, P = .162 | −0.289, P = .161 | . . . | 0.166, P = .427 |
| Ankle frontal-plane angle | 0.113, P = .592 | 0.593, P = .002 | 0.084, P = .690 | −0.400, P = .047 | 0.158, P = .452 | 0.166, P = .427 | . . . |
aFrontal-plane angles: (+) = abduction, (−) = adduction.
bTransverse-plane angles: (+) = internal rotation, (−) = external rotation.
When bilateral average hip and knee frontal-plane angles were considered in a stepwise multiple regression model that controlled for the influence of stance width, bilateral average hip frontal-plane angle was the only predictor of NKSD, explaining 66% of the variance (R2 = 0.66, P < .001). Stance width, entered into the model to account for the effects of foot position, was a significant predictor of NKSD, explaining 31% of the variance (R2 = 0.31, P = .004). Together, these variables explained 97% of the variance in NKSD (R2 = 0.97, P < .001). Knee frontal-plane angle did not enter into the model based on the entry and removal criteria of the stepwise regression.
DISCUSSION
Our results support our primary hypothesis that measures of NKSD can predict bilateral average knee-abduction angle. After accounting for stance width, we found a moderate relationship between 2-D measures of NKSD in the frontal-plane and 3-D bilateral average frontal-plane angles of the knee. The 2 variables were negatively correlated, indicating that participants with smaller knee separation distances had greater bilateral average knee-abduction angles. This finding is consistent with that of previous authors12,13 who reported moderate correlations between measures of 2-D and 3-D knee-abduction angles during single-limb and double-limb tasks. These data suggest that measures of distance between the knees in the frontal plane may provide some information about knee frontal-plane angle during a drop land.
A further understanding of the association between 3-D lower extremity transverse-plane and frontal-plane angles and 2-D NKSD is important in interpreting the results of clinical screening techniques that assess NKSD. In contrast to our secondary hypothesis, only 2 kinematic variables correlated with NKSD. In the frontal plane, a significant correlation between hip angle and NKSD was noted. A positive correlation between bilateral average hip frontal-plane angle and NKSD indicates that greater hip adduction was associated with a smaller distance between the knees. This finding is logical because hip adduction brings the distal femurs closer together in the frontal plane. A significant negative correlation between frontal-plane knee angle and NKSD suggests that greater knee-abduction angles were associated with smaller NKSDs. Distally, no relationship between bilateral average ankle frontal-plane angle and NKSD was noted. However, stance width was positively correlated with NKSD: those who landed with a wider stance had a greater distance between their knees. It may be important to consider that NKSD can be influenced by foot placement during double-limb landing tasks. Surprisingly, transverse-plane angles at the hip and knee were not correlated with NKSD in our study. Hip internal rotation is thought to affect 2-D measures of knee-abduction angle by projecting knee flexion angle into the frontal plane.13 However, to date, the extent to which hip internal rotation is associated with 2-D knee abduction during double-limb tasks has not been assessed. Data in the current study suggest that out-of-plane motion in the transverse plane does not influence 2-D measures of NKSD during a drop-land task.
When the variables that were significantly correlated with NKSD and knee and hip frontal-plane angles were considered in a stepwise regression analysis that controlled for the influence of stance width, the only variable to enter the model was bilateral average hip frontal-plane angle. Stance width explained 31% of the variance in NKSD. Together with stance width, hip frontal-plane angle explained 97% of the variance in NKSD. Predictably, a moderate correlation between knee and hip frontal-plane angles was found. Given the constraints of a task that entails bilateral foot contact, we expected that motion at the hip and knee in the same plane would be related. Knee frontal-plane angle was not included in the stepwise regression model after stance width and hip frontal-plane angle were entered; thus, the contribution of knee frontal-plane angle to the variance in NKSD was attenuated by the inclusion of these variables. These data indicate that although a relationship between knee frontal-plane angle and NKSD may exist, frontal-plane angle at the hip may be a stronger indicator of NKSD.
Despite the associations between 2-D measures of knee separation distance and 3-D joint angles, one must consider the inherent limitations of using measures of knee separation distance for clinical analyses. Specifically, a drop jump is a bilateral task; in order to account for the contribution of each limb to knee separation distance, joint angles of the right and left limbs were averaged. Clinically, it would not be possible to determine the individual contribution of each limb to NKSD. Therefore, these measures can assess only overall lower extremity posture and may not be sensitive to unilateral deficits. Furthermore, we measured 2-D knee separation distance from coordinate measures of reflective markers using high-speed motion capture cameras. This technique has been used in previous research studies9,10 assessing sex differences in valgus knee motion during drop landings. However, clinical screening of knee separation distance typically relies on still frame photos taken from standard video camera recordings, so clinical techniques may result in less accurate measures of knee separation distance than those assessed in the current study. Therefore, the association between 2-D knee separation distance measured clinically and 3-D lower extremity angles may differ from the relationships we report.
The use of 2-D NKSD measures during landing has been advocated6,8,11 for clinical screening of valgus lower extremity alignment. Our data suggest that NKSD during a drop land can provide information about the medial collapse of the lower extremities. Yet how this information can be interpreted with respect to identifying faulty patterns or assessing risk for injury is unclear. Although sex differences in NKSD were identified in prepubescent athletes using this technique,8 no differences were noted in a larger cohort of 536 athletes between the ages of 9 and 17 years.15 These disparate results indicate that knee separation distance may not be sensitive enough to identify relevant sex-related differences in landing postures. Moreover, no data have related knee separation distance to injury. Still, this method may be a useful tool for assessing changes in overall landing posture after an intervention: Noyes et al6 detected improvement in NKSD after a jump-training program in a cohort of young female athletes.
Agreement among clinicians using traditional observational methods has been only fair,16 suggesting that more objective measures are needed for clinical assessment. Our data indicate that assessment techniques measuring knee separation distance during a bilateral landing task can provide information about the frontal-plane posture of the lower extremities during landing. However, caution must be taken when relating these measures to knee-abduction angles because frontal-plane hip angle and stance width are strongly related to knee separation distance.
Acknowledgments
The National Institutes of Health (R01 AR053073-02) funded this study.
REFERENCES
- 1.Hewett TE, Myer GD, Ford KR. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament injury risk in female athletes: a prospective study. Am J Sports Med. 2005;33(4):492–501. doi: 10.1177/0363546504269591. et al. [DOI] [PubMed] [Google Scholar]
- 2.Powers CM. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther. 2003;33(11):639–646. doi: 10.2519/jospt.2003.33.11.639. [DOI] [PubMed] [Google Scholar]
- 3.Powers CM. The influence of abnormal hip mechanics on knee injury: a biomechanical perspective. J Orthop Sports Phys Ther. 2010;40(2):42–51. doi: 10.2519/jospt.2010.3337. [DOI] [PubMed] [Google Scholar]
- 4.Chmielewski T, Tillman S, Hodges MJ, Horodyski M, Bishop MD, Conrad BP. Investigation of clinician agreement in evaluating movement quality during unilateral lower extremity functional tasks: a comparison of 2 rating methods. J Orthop Sports Phys Ther. 2007;37(3):122–129. doi: 10.2519/jospt.2007.2457. [DOI] [PubMed] [Google Scholar]
- 5.Ekegren CL, Miller WC, Celebrini RG, Eng JJ, Macintyre DL. Reliability and validity of observational risk screening in evaluating dynamic knee valgus. J Orthop Sports Phys Ther. 2009;39(9):665–674. doi: 10.2519/jospt.2009.3004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Noyes FR, Barber-Westin SD, Fleckenstein C, Walsh C, West J. The drop-jump screening test: difference in lower limb control by gender and effect of neuromuscular training in female athletes. Am J Sports Med. 2005;33(2):197–207. doi: 10.1177/0363546504266484. [DOI] [PubMed] [Google Scholar]
- 7.Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE, Jr, Beutler AI. The Landing Error Scoring System (LESS) is a valid and reliable clinical assessment tool of jump-landing biomechanics: the JUMP-ACL Study. Am J Sports Med. 2009;37(10):1996–2002. doi: 10.1177/0363546509343200. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Barber-Westin SD, Galloway M, Noyes FR, Corbett G, Walsh C. Assessment of lower limb neuromuscular control in prepubescent athletes. Am J Sports Med. 2005;33(12):1853–1860. doi: 10.1177/0363546505278257. [DOI] [PubMed] [Google Scholar]
- 9.Ford KR, Myer GD, Hewett TE. Valgus knee motion during landing in high school female and male basketball players. Med Sci Sports Exerc. 2003;35(10):1745–1750. doi: 10.1249/01.MSS.0000089346.85744.D9. [DOI] [PubMed] [Google Scholar]
- 10.Hewett TE, Myer GD, Ford KR. Decrease in neuromuscular control about the knee with maturation in female athletes. J Bone Joint Surg Am. 2004;86(8):1601–1608. doi: 10.2106/00004623-200408000-00001. [DOI] [PubMed] [Google Scholar]
- 11.Sigward SM, Ota S, Powers CM. Predictors of frontal plane knee excursion during a drop land in young female soccer players. J Orthop Sports Phys Ther. 2008;38(11):661–667. doi: 10.2519/jospt.2008.2695. [DOI] [PubMed] [Google Scholar]
- 12.McLean SG, Walker K, Ford KR, Myer GD, Hewett TE, van den Bogert AJ. Evaluation of a two dimensional analysis method as a screening and evaluation tool for anterior cruciate ligament injury. Br J Sports Med. 2005;39(6):355–362. doi: 10.1136/bjsm.2005.018598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Nagano Y, Sakagami M, Ida H, Akai M, Fukubayashi T. Statistical modelling of knee valgus during a continuous jump test. Sports Biomech. 2008;7(3):342–350. doi: 10.1080/14763140802233223. [DOI] [PubMed] [Google Scholar]
- 14.Grood ES, Suntay WJ. A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng. 1983;105(2):136–144. doi: 10.1115/1.3138397. [DOI] [PubMed] [Google Scholar]
- 15.Barber-Westin SD, Noyes FR, Galloway M. Jump-land characteristics and muscle strength development in young athletes: a gender comparison of 1140 athletes 9 to 17 years of age. Am J Sports Med. 2006;34(3):375–384. doi: 10.1177/0363546505281242. [DOI] [PubMed] [Google Scholar]
- 16.Chmielewski TL, Hodges MJ, Horodyski M, Bishop MD, Conrad BP, Tillman SM. Investigation of clinician agreement in evaluating movement quality during unilateral lower extremity functional tasks: a comparison of 2 rating methods. J Orthop Sports Phys Ther. 2007;37(3):122–129. doi: 10.2519/jospt.2007.2457. [DOI] [PubMed] [Google Scholar]