

Abstract
Context:
Methicillin-resistant Staphylococcus aureus (MRSA) infections are increasingly common in athletic settings. The MRSA knowledge and infection-control practices of certified athletic trainers (ATs) and the cleanliness of the athletic training room are important factors in preventing MRSA infections.
Objective:
To assess knowledge of MRSA and the use of common disinfectants among ATs and to explore their infection-control practices.
Design:
Cross-sectional study.
Setting:
High school and collegiate athletic training rooms.
Patients or Other Participants:
A total of 163 ATs from National Collegiate Athletic Association Divisions I, II, and III and high schools, representing all 10 National Athletic Trainers' Association districts.
Main Outcome Measure(s):
Frequencies, analyses of variance, and χ2 tests were used to assess current practices and opinions and relationships between factors.
Results:
Methicillin-resistant Staphylococcus aureus was perceived as a national problem by 92% of respondents; 57% perceived MRSA as a problem in their practice setting. Most respondents had treated general infections (88%), staphylococcal infections (75%), and MRSA infections (57%). Male sex was associated with treating all 3 types of infections (χ2 test, P < .05). Noncurriculum education was associated with a lack of recognition of environmental issues as risk factors and with the use of isopropyl alcohol for disinfection (χ2 test, P < .05). For example, 10% of respondents did not recognize that contaminated whirlpools can be a source of MRSA infection. Respondents also incorrectly identified effective cleaning solutions. Thirty percent of respondents cleaned their hands frequently or sometimes before treating each athlete and 35% cleaned their hands sometimes, occasionally, or never after seeing each athlete.
Conclusions:
The majority of ATs were informed about MRSA and made correct disinfection choices. However, improvements are still needed, and not all ATs were using proper disinfection practices.
Keywords: infection control, communicable diseases, cleaning habits
Key Points.
Although many athletic trainers were informed about methicillin-resistant Staphylococcus aureus and taking appropriate steps, some lacked the necessary knowledge.
Athletic trainers need to improve their hand-washing hygiene, cleaning their hands before and after every contact with a patient or athlete.
In order to reduce the risk of methicillin-resistant Staphylococcus aureus, athletic trainers must be familiar with the most current evidence-based guidelines and implement those recommendations accordingly.
Every year, methicillin-resistant Staphylococcus aureus (MRSA) infects approximately 100 000 people in the United States.1 Authors1 of a recent study estimated that MRSA is responsible for approximately 18 650 in-hospital deaths annually. It was once considered an exclusively hospital-acquired infection,2 but community-associated rates of MRSA have risen steadily.2–4 Community-associated MRSA, which is more applicable to athletic environments, occurs in otherwise healthy people who have not been hospitalized in the past year or had medical procedures such as dialysis, surgery, or catheter placement. The condition usually presents as a skin infection such as an abscess, boil, or other pus-filled lesion, but it may lead to a more serious illness, such as pneumonia.5 Hospital-acquired MRSA is more common in hospitalized patients with weak immune systems and may also affect people in long-term care facilities and those receiving kidney dialysis.6
Athletes and athletic staff are particularly affected by community-associated MRSA,7–15 with MRSA infections occurring at all levels of sport across the United States and abroad,16 although not in greater proportions than in the general population.17 Several student-athletes have died from MRSA infections, including 4 high school football players.18–21 In each case, the MRSA infection was attributed to the student's sport-related activities.
Athletes are more likely than the general public to develop MRSA infections because of both personal and environmental conditions.16,22 The disinfectant practices in the athletic training room, where athletes receive health care from certified athletic trainers (ATs), may affect MRSA infection rates. Several groups11,19–24 have implicated improper cleaning and disinfection of the athletic training room as contributing factors to MRSA infections. Proper use of disinfectants is essential for infection control.25,26 In order to decrease the occurrence of MRSA, ATs should have access to up-to-date information on MRSA prevention in the sports medicine facility.
However, ATs and athletic training students may be unaware of proper disinfection practices. The National Athletic Trainers' Association (NATA) has released an official statement on MRSA,27 but the statement does not discuss proper disinfection techniques. The Centers for Disease Control and Prevention (CDC) and the Association for Professionals in Infection Control and Epidemiology, Inc (APIC), have also released guidelines on MRSA, including general disinfection practices.28–30
Many disinfectant products exist, some of which are unsuitable for preventing MRSA infections in athletic training rooms. However, a comprehensive examination of disinfection practices and disinfectant knowledge among ATs has not been completed, and some ATs may not be fully aware of the choices for effective MRSA disinfection. Therefore, the purpose of our study was to investigate ATs' self-reported behaviors regarding disinfectant practices and their perceived knowledge of MRSA and common disinfectants and to assess whether perceived knowledge, sex, or institutional level affected the reported incidence of MRSA.
METHODS
Participants were randomly chosen from a list provided by the NATA of 1000 ATs from National Collegiate Athletic Association (NCAA) Division I, II, and III institutions and high schools. The resulting list (N = 250) was examined to determine whether multiple individuals were selected from the same institution in order to eliminate redundant sites. No redundancy was identified, and the sample pool was then input into the electronic survey instrument.
Instrumentation
We designed the questionnaire using a combination of original questions, questions selected from a previous study, and CDC recommendations.5,6,31–35 The questionnaire consisted of a welcome page with the consent form, followed by 7 sections: (1) “Knowledge of MRSA,” (2) “Knowledge of Common Disinfectants,” (3) “Reported Practices–Hard Surface Disinfectants,” (4) “Reported Practices–Personal Habits,” (5) “Experiences with MRSA,” (6) “Education and Awareness,” and (7) “Demographics.” Four experts in the field (a microbiologist, a health care educator, and 2 ATs; mean age = 42 years, mean years of experience = 14) assessed the questionnaire for content validity. Content changes were minimal and focused on vernacular, style, and grammar. Two of the investigators examined the usability of the study to determine the functionality of the electronic questionnaire before the survey was initiated.
The questionnaire consisted of 39 questions on 8 screen pages. The 10 demographic items consisted of age, sex, employment setting, credentials, public or private institution, supervising entity, number of athletes, patient contacts, socioeconomic status of institution state, and years certified. The “Knowledge of MRSA” section contained 2 questions. One item included 7 variables assessed on a 5-point Likert scale for perceptions and was treated as continuous data. The other item measured the perception of MRSA risk factors with 12 variables assessed on a 3-point scale of categorical answers: primary risk factor, secondary risk factor, and not a risk factor. The “Knowledge of Common Disinfectants” section asked 2 questions, and the “Reported Practices” sections asked 10 questions with discrete categorical answers. The “Experiences with MRSA” section was extensive, with 7 discrete areas of inquiry. The “Education and Awareness” section included 6 discrete answer questions. All questions were categorical except 2: 1 item each in “Knowledge of MRSA” and “Reported Practices” used a continuous Likert scale to measure perceptions. Several questions were numeric fill in the blanks, including the number of athletes with MRSA, number of athletes in the institution, number of athlete contacts in a week, and number of years as an AT.
Procedures
The study was approved by the institutional review board before the survey was disseminated. Survey Monkey (Survey-Monkey.com, Portland, OR) was used to deliver the instrument and collect the data in a closed survey, such that only the randomly selected applicants had access to the survey through an e-mail invitation. Once the participant completed the survey, he or she was prevented from taking it again. Potential respondents were e-mailed a request for participation; clicking on the survey link indicated consent to participate. Three weeks after the initial e-mail, follow-up reminder invitations were sent to those who had not completed the survey, and thank-you e-mails were sent to those who had completed the survey. The survey remained open for 60 days, and respondents completed the survey on a computer of their choice.
Once respondents navigated to the site and began the survey, information about their participation was anonymous, securely stored on the SurveyMonkey.com servers, and downloaded to a password-protected computer for analysis. Analysis was completed using SPSS (version 16.0; SPSS Inc, Chicago, IL). Descriptive statistics (means, SDs, frequencies, and percentages) were used to assess demographics and describe respondents' perceived knowledge of MRSA risk factors, disinfectant efficacy, and self-reported cleaning practices. We performed χ2 testing to determine whether associations were present between variables such as sex and disinfectant used and between institution level and frequency of whirlpool cleaning. Two analyses of variance were conducted to assess ATs' perceptions of MRSA with the number of infections and the number of MRSA infections with frequency of table cleaning.
RESULTS
Demographics
Of 927 valid e-mail addresses sent invitations, 163 participants (17.5%) completed the survey and 109 of these (67%) answered every question. Responses from participants who did not answer all questions were included, with no response recorded for unanswered questions. Respondents consisted of 81 men (50%), 70 women (43%), and 12 individuals (7%) who did not self-identify sex. Athletic training experience ranged from 1 to 33 years, with a mean of 11.23 ± 8.10 years. A total of 69% of respondents (n = 113) had a master's degree in athletic training or a related field. Two participants (1%) reported having a doctorate in a related field. Respondents represented all 10 NATA districts. Districts 2 (19%, n = 31) and 4 (17%, n = 28) had the most respondents. Institution levels represented included high school (37%, n = 60), NCAA Division I (21%, n = 35), NCAA Division III (19%, n = 31), NCAA Division II (6%, n = 10), National Association of Intercollegiate Athletics (4%, n = 7), and junior colleges (4%, n = 6).
ATs' Experiences with MRSA
A total of 88% of respondents (n = 143) reported treating an athlete with a skin or limb infection during their career: 75% (n = 123) with a staphylococcal infection and 57% (n = 94) with a MRSA infection that was validated by a physician. Ten respondents (n = 6%) were unsure whether they had treated an athlete with a MRSA infection. The number of athletes with MRSA infections per respondent ranged from 0 to 50 athletes, with a mean of 5.13 ± 7.88.
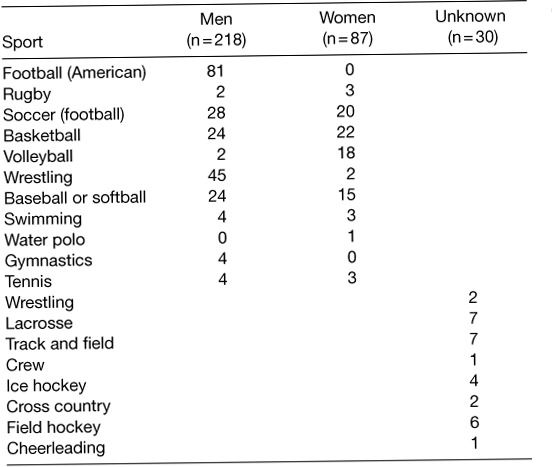
The most common sport of athletes treated for MRSA infections was American football (50%, n = 81) (Table 1). According to the ATs' reports, more than twice as many male athletes (n = 218) as female athletes (n = 87) had been treated by a physician for a MRSA infection.
Table 1.
Methicillin-Resistant Staphylococcus aureus Infections by Sport
The most common locations identified by the ATs for MRSA infections were the lower leg or feet (42%, n = 69), knee (29%, n = 47), lower arm or hand (28%, n = 45), upper leg (26%, n = 43), and upper arm (21%, n = 35). Most MRSA infections were initially diagnosed and confirmed by a physician as a general skin infection, including Staphylococcus (33%, n = 54) or MRSA (31%, n = 51). Twenty-four percent of reported infections were initially misdiagnosed as an ingrown hair (14%, n = 22) or spider bite (10%, n = 17).
ATs' Perceived Knowledge of MRSA
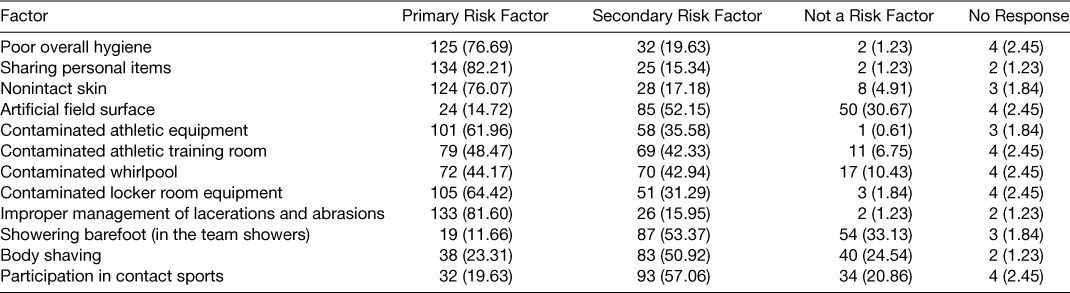
Most respondents (92%, n = 150) agreed that MRSA was a national problem, yet only a little more than half (57%, n = 94) perceived that MRSA was a problem in their practice setting (Table 2). The number who perceived MRSA as a problem in their practice setting and treated more athletes with a physician-validated MRSA infection was significant (F4,126 = 3.183, P = .016). The most common primary risk factors for MRSA selected by respondents were sharing personal items, improper management of lacerations and abrasions, poor overall hygiene, and nonintact skin. Showering barefoot in team showers, artificial turf, body shaving, and participation in contact sports were not thought to be risk factors. Just over 10% of respondents (n = 17) perceived that contaminated whirlpools were not risk factors in developing a MRSA infection (Table 3).
Table 2.
Perceptions of Athletic Trainers Regarding Methicillin-Resistant Staphylococcus aureus (MRSA)
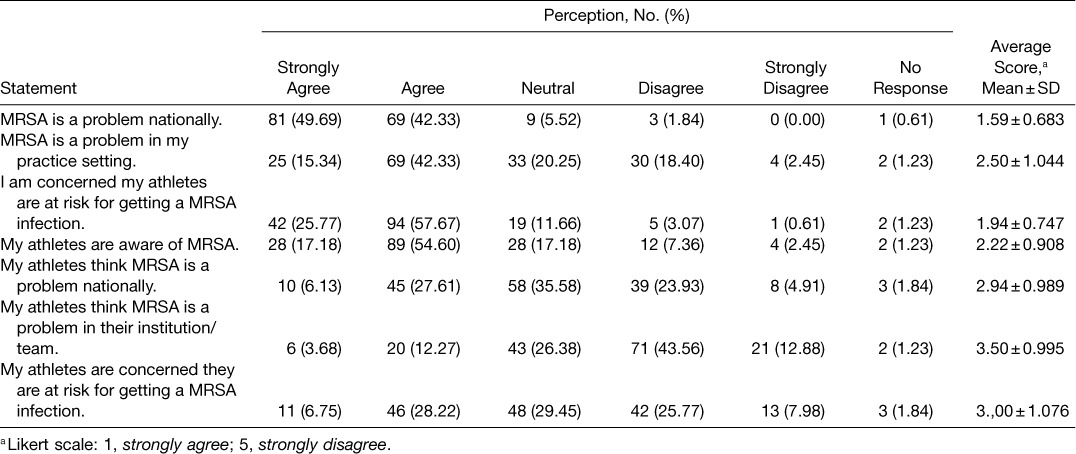
Table 3.
Athletic Trainers' Perceptions of Risk Factors for Methicillin-Resistant Staphylococcus aureus Infections, No. (%)
ATs' Perceived Knowledge of Disinfectants and Disinfectant Practices
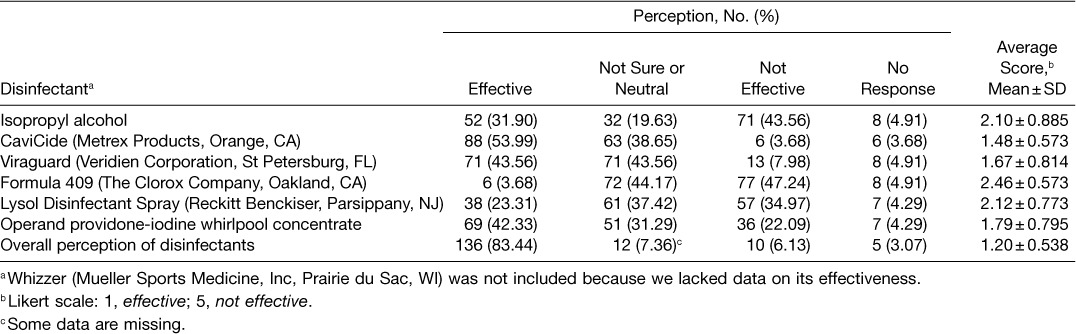
Many respondents had difficulty identifying which disinfectants were effective against MRSA. Nearly half were not sure whether Formula 409 (The Clorox Company, Oakland, CA) (44.2%, n = 72) and Viraguard (Veridien Corporation, St Petersburg, FL) (43.6%, n = 71) were effective. Forty-two percent (n = 69) incorrectly identified an operand povidone-iodine whirlpool concentrate as an effective disinfectant (Table 4). Respondents indicated that frequency of use (88%, n = 144), product choice (69%, n = 113), and soaking time (66%, n = 108) were important factors in achieving disinfection.
Table 4.
Athletic Trainers' Perceptions of Effectiveness of Disinfectants Against Methicillin-Resistant Staphylococcus aureus, No. (%)
Sixty-five percent of respondents (n = 106) reported using a product designed for disinfecting whirlpools. The most popular products designed for disinfection were Whizzer (Mueller Sports Medicine, Inc, Prairie du Sac, WI) (20%, n = 24) and CaviCide (Metrex Products, Orange, CA) (22%, n = 26) (some data were missing). Nine respondents (6%) indicated that they used an iodine solution as their primary method of cleaning whirlpools. Whirlpool cleaning frequency ranged from after every athlete (14%, n = 23) to yearly (1%, n = 2). The largest group of respondents (66%, n = 107) indicated that they cleaned their whirlpools daily (Figure 1). Whizzer and CaviCide were also the most popular products designed for disinfecting treatment tables (20%, n = 24 and 22%, n = 26, respectively; some data were missing). Cleaning frequency for taping and treatment tables ranged from after every athlete (27%, n = 44) to monthly (0.6%, n = 1), with the largest group (54%, n = 88) cleaning daily. The number of athletes with MRSA infections was greater (F17,125 = 3.286, P < .001) when the treatment tables were cleaned less often.
Figure 1.
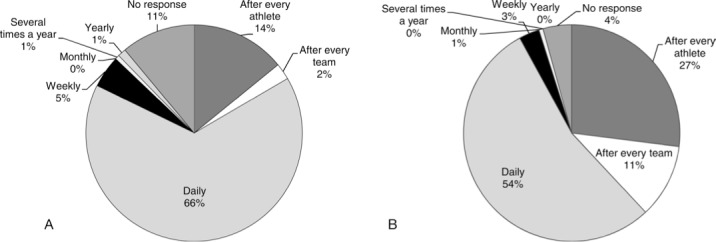
Athletic trainers' frequency of cleaning. A, Whirlpool. B, Treatment and taping tables.
A total of 52% of respondents (n = 85) specified that the reason they used certain cleaning products was conventional wisdom. Of the 26 respondents who specified other, 38% (n = 10) identified time and personnel constraints as reasons for cleaning in a particular fashion.
Personal cleaning habits varied from always cleaning one's hands before and after seeing an athlete to never cleaning one's hands (Table 5). Most respondents indicated that they washed their hands with soap and water before seeing each athlete frequently (35%, n = 57) or sometimes (32%, n = 52). Alcohol-based hand sanitizer was sometimes used before each athlete (29%, n = 47) and frequently (27%, n = 44) used after each athlete. The majority of respondents indicated that they had manual dispensers for soap (83%, n = 136), alcohol-based hand sanitizer (83%, n = 136), and gloves (90%, n = 146) (Figures 2, 3).
Table 5.
Athletic Trainers' Personal Cleaning Habits
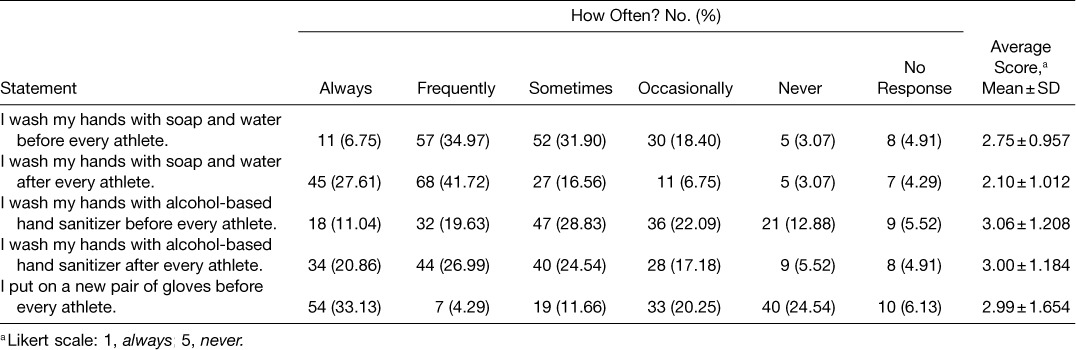
Figure 2.
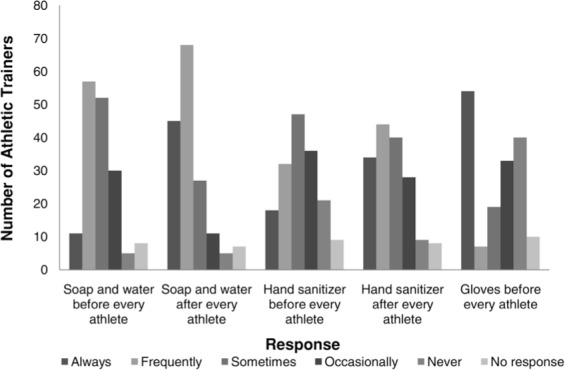
Personal cleaning practices of athletic trainers.
Figure 3.
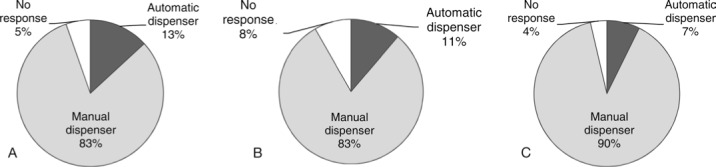
Manual and automatic dispenser availability. A, Soap and water. B, Alcohol-based hand sanitizer. C, Gloves. Percentages do not all add to 100 because of rounding.
Relationships Between Demographic Factors and MRSA
We used a χ2 test to assess relationships between sex, education, institution level, cleaning frequency, opinions on risk factors, disinfectant use, opinions about disinfection, and attitudes about MRSA. Significant relationships were typically identified when sex or education was included in the χ2 test. Sex played a dominant role in comparisons of MRSA infections within sports: Men were more likely to encounter and treat MRSA. Men were more likely to report MRSA infections in football (χ21 = 8.479, P = .004), men's basketball (χ21 = 5.621, P = .018), men's wrestling (χ21 = 8.791, P = .003), and baseball (χ21 = 8.951, P = .003). Men also identified poor overall hygiene (χ22 = 7.923, P = .019) and artificial field surface (χ22 = 7.042, P = .030) as MRSA risk factors more often than did women. Sex was associated with treatment of skin or limb infection (χ21 = 4.986, P = .026), staphylococcal infection (χ22 = 9.132, P = .010), and MRSA infection (χ22 = 9.871, P = .007). In all 3 infection-sex associations, men reported treating more infections than did women. Male sex was associated with an initial diagnosis of spider bite (χ21 = 3.897, P = .048) and general skin infection (χ21 = 6.183, P = .013). In addition, men reported being approached by an athlete's family member or guardian for information about MRSA more often than did women (χ21 = 5.342, P = .021). More than women did, men indicated that price was a factor in choosing a cleaning product (χ216 = 50.771, P < .001). Chi-square test findings suggested that sex was associated with considering frequency of use an important factor in using a disinfectant, as men selected frequency of use more often (χ21 = 4.04, P = .045).
Work setting had no association with number of reported MRSA cases, disinfectants used, or reported practices or knowledge. The institution type (public or private) and institution level (high school or college) were not associated with respondents' opinions or practices.
Lower education (bachelor's degree versus master's degree or higher) was associated with treating more MRSA infections, using isopropyl alcohol-water solution to clean whirlpools and taping and treatment tables, and poor hand-hygiene behaviors (eg, occasionally or never washing hands with soap and water before every athlete) (data not shown).
DISCUSSION
Respondents appeared to have mixed positions on MRSA infections and risk. Although they clearly perceived MRSA as a national problem, they did not all perceive that MRSA was a problem in their practice setting. This result may explain why some of the respondents used traditional disinfectants instead of newer, more effective disinfectants such as Whizzer or Bleach Rite (MarketLab, Inc, Caledonia, MI).34 Respondents were aware of MRSA and considered it a health problem, yet they did not engage in MRSA-prevention practices through proper disinfection.
Conflicting viewpoints about MRSA were mirrored in respondents' reported practices. The CDC32 and NATA27 both recommended washing with either soap and water or an alcohol-based hand sanitizer before and after every patient. Fewer than half of respondents followed these recommendations. A small percentage of respondents never cleaned their hands with soap and water or an alcohol-based hand sanitizer before or after each athlete. Surprisingly, never cleaning one's hands was not identified by ATs with higher rates of reporting MRSA infections. Good hand-hygiene practices reduce the spread of bacteria and viruses and are essential in preventing infection.4,5,32,33 Self-reported hand-hygiene practices were worse in this study than in a similar study.31 Across employment settings, respondents indicated a lower percentage of hand cleansing. Deteriorating hand-care practices could result from a decreasing fear of MRSA or a difference in the populations surveyed. The respondents' demographic factors in the Goding et al31 survey were similar to ours in terms of sex, experience, and work setting, but their respondents might have been more interested in MRSA and thus more attentive to hand hygiene. Goding et al conducted an open survey on the NATA Web site, which might have attracted people interested in MRSA, a self-selected population that was perhaps different from our sample. We selected random recipients who may not have had a particular interest in MRSA. Logically, respondents who were less concerned about MRSA might be less likely to practice good hygiene practices. Additionally, our randomized selection of participants might have affected the study's low response rate. The large percentage of participants who chose not to complete our survey may reflect ATs who are less comfortable discussing MRSA and their disinfection practices because of a perceived lack of knowledge or embarrassment about their practices. Therefore, perceived knowledge and disinfection practices may be more favorable in the Goding et al study than in ours. However, our study population represents only 1.5% of NATA members in the collegiate (n = 6341) and secondary school (n = 4542) settings, so general-izability may be limited. Additional investigations with larger samples are warranted.
The most common risk factors for developing a MRSA infection are poor personal hygiene, participation in a contact sport, nonintact or open skin, abrasions from artificial grass, body shaving, contaminated athletic equipment, contaminated athletic training rooms, and use of contaminated whirlpools.5,11,22–24,27,31 Respondents were largely accurate in identifying risk factors for MRSA infections. However, body shaving and participation in a contact sport were not considered risk factors by approximately 20% of respondents. Previous authors22–24 have associated body shaving and participation in contact sports with increased risk for MRSA infection. Athletic trainers are often a primary source of information for athletes about MRSA risk factors and therefore need to be well versed in current evidence-based practices.
The status of contaminated whirlpools as the top cited risk factor for MRSA infection led to specific survey questions about whirlpool-cleaning practices. A small percentage of ATs did not consider whirlpools a source of contamination, which, although encouraging, indicates that further education about the potential for MRSA contamination is needed. Most respondents used a commercial product designed for disinfection such as CaviCide, Viraguard, or Whizzer. However, some reported still using an isopropyl alcohol-water solution or an iodine solution to clean their whirlpools, neither of which kills MRSA.34 Additionally, many respondents did not clean the whirlpools frequently enough. The CDC recommended cleaning whirlpools after every patient.30 Only 14% of respondents adhered to the CDC recommendations. Athletic trainers must be aware of proper whirlpool-disinfection standards in order to prevent MRSA transmission. Respondents cleaned the treatment and taping tables more frequently than the whirlpools and were more likely to use a product designed for disinfection as recommended by the CDC28–30 than they did for whirlpools. Thus, respondents may be more concerned about the cleanliness of taping and treatment tables than the cleanliness of whirlpools, not understand the significance of MRSA transmission through improperly maintained whirlpools, have a traditional perspective on communal whirlpools, or not be motivated or lack adequate staff to attend to the cumbersome task of whirlpool cleaning after every patient or athlete.
Respondents cited conventional wisdom as their primary basis of knowledge about cleaning habits. A small percentage of respondents also cited budget constraints, advice from colleagues, product advertisements, or other factors as reasons for their cleaning habits. More than one-third of respondents who selected other as a response cited time and personnel constraints as reasons for infrequent cleaning. Administrators may need to reevaluate staffing situations, because limited staffing may contribute to MRSA infections. Some ATs may not have time to clean whirlpools and treatment tables after every athlete because of large patient loads. Hiring more ATs per institution may provide additional time to develop and implement more effective disinfection policies and practices. When asked why they chose a particular product, 63% of respondents cited research. Although this finding suggests that approximately two-thirds of ATs stayed current with the literature, it also suggests that roughly one-third did not. This is probably the reason why some respondents incorrectly identified effective disinfectants, did not identify MRSA risk factors, and did not use proper dis-infection techniques, all of which may reflect the time and personnel limitations previously discussed. In general, ATs need a more accurate understanding of disinfectant practices and how these practices affect exposure to MRSA. As athletic training focuses on evidence-based medicine in order to provide the best medical care,35 ATs need to constantly recheck the current research to ensure they are using the most effective techniques to prevent MRSA infection.
The CDC recommends using disinfectants registered by the Environmental Protection Agency (EPA) according to each manufacturer's directions.28,29 The use of off-brands, such as generic household bleach instead of Clorox bleach, is discouraged, but this leads to cost concerns for some ATs. Several respondents indicated that they used bleach to clean their whirlpools, treatment tables, and taping tables. Although bleach is currently registered by the EPA as effective against MRSA, its efficacy has been in doubt since several groups36–39 identified bleach as ineffective. Clorox bleach was not approved by the EPA until November 21, 2007.34 Clorox bleach was deemed effective at killing MRSA, and although this claim was not supported by evidence available at the time of the survey, it is now known to be correct. The APIC26 recommended bleach at a dilution of 1:10 (5000–6150 parts per million of available chorine) or 1:100 (500–615 parts per million of available chlorine) for cleaning hard surfaces. A variety of Lysol products were also approved in late 2007, including Foaming Disinfectant Basin Tub and Tile Cleaner II (November 15, 2007), Direct Multi-purpose Cleaner (October 17, 2007), and S. A. Cleaner (August 9, 2007).34 Many of Lysol's consumer products, such as their kitchen and bathroom cleaner, are not EPA registered.34 Whizzer and CaviCide are both EPA registered; however, Whizzer was registered in 1968 as a general disinfectant and is not on the EPA's list as effective against MRSA.34 Essentially, Whizzer is not recommended for killing MRSA, yet 22% of respondents who indicated using a product designed for disinfection specified Whizzer as their disinfectant of choice. Many ATs are currently using povidone-iodine and isopropyl alcohol to disinfect whirlpools, although neither is effective against MRSA. Athletic trainers' use of a product that is not registered as effective against MRSA may mean that both they and their athletes are being exposed to infection. Therefore, ATs must evaluate their choice of cleaning product to determine whether it is EPA registered as effective against MRSA. If ATs cannot accurately identify which products are effective against MRSA, they may choose ineffective products, thereby decreasing the cleanliness and safety of the athletic training room and increasing the risk of MRSA infection.
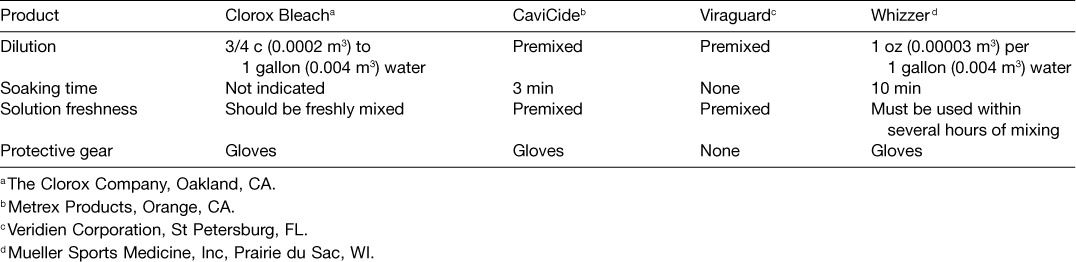
Using disinfectants improperly may be another problem. For example, many products require long soaking times and freshly mixed solutions to maximize their effectiveness (Table 6). Solutions must also be mixed with the correct dilution. Dilution was considered an important factor in disinfectant use by only 55% of respondents. Soaking time was considered an important factor by 66% of respondents. Athletic trainers need to read the manufacturer's instructions on proper usage in order to ensure correct use of the product.
Table 6.
Manufacturer's Instructions for Common Disinfectants
Citing of contaminated environments as risk factors was associated with sex. Men were more likely to consider contaminated environments as risk factors. They also reported more general, staphylococcal, and physician-validated MRSA infections and more infections in men's sports. These findings may have occurred because men may typically be assigned to men's sports, and male athletes were more than twice as likely to have a MRSA infection as female athletes. Why male athletes were more likely to develop MRSA infections as reported by ATs is unknown. The most probable reasons include a lack of personal hygiene, more cuts and scrapes (from increased contact), more time spent in group whirlpools, and a generally “dirtier” existence, such as laundering clothes less frequently and leaving equipment in lockers or gym bags for long periods of time. These reasons do not apply to all male athletes and do not constitute a complete or confirmed list, only a potential list. Male respondents also considered poor personal hygiene a risk factor more often than did female respondents. Furthermore, women were more likely to report that they were unsure whether they had treated a MRSA infection. One might assume there is a sex bias in education, but a sex bias in sport assignments is more plausible. Female ATs may not be exposed to MRSA infections as often as are male ATs because women are typically not assigned to men's sports such as football, which has a much higher infection rate than most women's sports. Male respondents indicated that they were approached by their athletes' families for information about MRSA more than were female respondents. Female ATs may not encounter athletes from sports with a high risk of MRSA (eg, football) as often as men do, accounting for a lower rate of reported MRSA infections. Interestingly, male respondents chose frequency of use as an important factor in using a disinfectant (ie, they based their frequency of use on the disinfectant they were using) but did not clean more frequently than female respondents. The data from this study suggest that male ATs may be more knowledgeable about MRSA risk factors, have more experience with them, and possess greater knowledge about disinfectants. However, male ATs may be no more likely to implement proper disinfection techniques than are female ATs.
Sex was also associated with inaccurate diagnoses of MRSA infections before confirmation by a physician. Male respondents reported more misdiagnoses of general skin infection or spider bite than did female respondents. Other studies22,39 have indicated that misdiagnosis of MRSA infections is somewhat common. Most MRSA infections were initially diagnosed as skin infections. Overall, the number of MRSA infections reported by respondents was comparable with that of other studies31; a very slight increase may be due to different respondent demographics or to an actual increase in MRSA infections.
CONCLUSIONS
The NATA has released an official statement on MRSA,27 but the statement does not discuss proper disinfection techniques. The CDC and APIC also have released several guidelines on disinfection practices.25,28–30 Unfortunately, many ATs may not have the time to read such publications or to research proper disinfectants or the resources to hire dedicated cleaning professionals to manage their environments. These factors may affect ATs' knowledge about MRSA and common disinfectants and therefore affect their disinfection practices.
Athletic trainers are taking many steps to eradicate MRSA infection in athletes. However, some ATs still lack knowledge about disinfectants and MRSA. It is vital that ATs be aware of current research and recommendations on disinfectant use, products, and practices. Furthermore, ATs must improve their hand hygiene: Fewer than half cleaned their hands before and after contact with every athlete. These questions were not included in this study because of concern about the survey's length.
Future researchers should include more participants so that the statistical analyses have more power and the risks of type I and type II errors are minimized. Recommendations may change over time, and studies should be conducted to evaluate the dissemination of those changes and ATs' adherence to those changes. As time passes and new evidence is revealed, the role of the AT in MRSA infection prevention will not diminish. Awareness, comprehension, and practice of evolving disinfection standards will remain important parts of preventing MRSA infections.
REFERENCES
- 1.Klevens RM, Morrison MA, Nadle J. Invasive methicillin- resistant Staphylococcus aureus infections in the United States. JAMA. 2007;298(15):1763–1771. doi: 10.1001/jama.298.15.1763. et al. [DOI] [PubMed] [Google Scholar]
- 2.Chambers HF. The changing epidemiology of Staphylococcus aureus? Emerg Infect Dis. 2001;7(2):178–182. doi: 10.3201/eid0702.010204. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Wyllie DH, Crook DW, Peto TEA. Mortality after Staphylococcus aureus bacteraemia in two hospitals in Oxfordshire, 1997– 2003: cohort study. BMJ. 2006;333(7562):281. doi: 10.1136/bmj.38834.421713.2F. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Drews TD, Temte JL, Fox BC. Community-associated methicillin-resistant Staphylococcus aureus: review of an emerging public health concern. WMJ. 2006;105(1):52–57. [PubMed] [Google Scholar]
- 5.Centers for Disease Control and Prevention. Community-associated MRSA information for the public. http://www.cdc.gov/ncidod/dhqp/ar_mrsa_ca_public.html. Accessed May 1, 2010.
- 6.Centers for Disease Control and Prevention. Hospital-associated MRSA information for the public. http://www.cdc.gov/ncidod/dhqp/ar_mrsa_ca_clinicians.html#7. Accessed May 1, 2010.
- 7.Redziniak DE, Diduch DR, Turman K. Methicillin-resistant Staphylococcus aureus (MRSA) in the athlete. Int J Sports Med. 2009;30(8):557–562. doi: 10.1055/s-0029-1214382. et al. [DOI] [PubMed] [Google Scholar]
- 8.Rogers SD. A practical approach to preventing CA-MRSA infections in the athletic setting. Athl Ther Today. 2008;13(4):37–41. [Google Scholar]
- 9.Lindenmayer JM, Schoenfeld S, O'Grady R, Carney JK. Methicillin-resistant Staphylococcus aureus in a high school wrestling team and the surrounding community. Arch Intern Med. 1998;158(8):895–899. doi: 10.1001/archinte.158.8.895. [DOI] [PubMed] [Google Scholar]
- 10.Stacey AR, Endersby KE, Chan PC, Marples RR. An outbreak of methicillin-resistant Staphylococcus aureus infection in a rugby football team. Br J Sports Med. 1998;32(2):153–154. doi: 10.1136/bjsm.32.2.153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Kazakova SV, Hageman JC, Matava M. A clone of methicillin-resistant Staphylococcus aureus among professional football players. N Engl J Med. 2005;352(5):468–475. doi: 10.1056/NEJMoa042859. et al. [DOI] [PubMed] [Google Scholar]
- 12.Centers for Disease Control and Prevention (CDC) Methicillin-resistant Staphylococcus aureus among competitive sports participants: Colorado, Indiana, Pennsylvania, and Los Angeles Country, 2002– 2003. MMWR Morb Mortal Wkly Rep. 2003;52(33):793–795. [PubMed] [Google Scholar]
- 13.ABC News. Athletes vulnerable to dangerous staph infection. http://abcnews.go.com/WNT/Health/story?id=1580657. Accessed May 1, 2010.
- 14.ABC News. Superbug MRSA worries doctors, athletes. http://abcnews.go.com/Health/Primetime/story?id=410908&page=1. Accessed November 8, 2010.
- 15.CBS News. MRSA: fighting the superbug. http://www.cbsnews.com/stories/2007/11/08/60minutes/main3474157.shtml. Accessed May 1, 2010.
- 16.Withers T. Staph infections rise among athletes. Washington Post. http://www.washingtonpost.com/wp-dyn/content/article/2006/11/25/AR2006112500385.html. Accessed November 8, 2010.
- 17.Rackman MD, Ray SM, Franks AS, Bielak KM, Pinn TM. Community- associated methicillin-resistant Staphylococcus aureus nasal carriage in a college student athlete population. Clin J Sport Med. 2010;20(3):185–188. doi: 10.1097/JSM.0b013e3181dba80d. [DOI] [PubMed] [Google Scholar]
- 18.Tomaselli KP. New CDC report, recent events add to MRSA's infamy. Am Med News. http://www.ama-assn.org/amednews/2007/11/12/hlsc1112.htm. Accessed November 8, 2010.
- 19.Rao M, Langmaid T. Bacteria that killed Virginia teen found in other schools. CNN. http://articles.cnn.com/2007-10-18/health/mrsa.cases_1_mrsa-ashton-bonds-staphylococcus?_s=PM:HEALTH. Accessed November 8, 2010.
- 20.Cohen PR. Cutaneous community-acquired methicillin-resistant Staphylococcus aureus infection in participants of athletic activities. South Med J. 2005;98(6):596–602. doi: 10.1097/01.SMJ.0000163302.72469.28. [DOI] [PubMed] [Google Scholar]
- 21.Associated Press. PA football player, 17, dies of staph infection. WPVITV. http://abclocal.go.com/wpvi/story?section=news/local&id=6418291. Accessed February 24, 2011.
- 22.Cohen PR. Cutaneous community-acquired methicillin-resistant Staphylococcus aureus infection in participants of athletic activities. South Med J. 2005;98(6):596–602. doi: 10.1097/01.SMJ.0000163302.72469.28. [DOI] [PubMed] [Google Scholar]
- 23.Begier EM, Frenette K, Barrett NL. A high-morbidity outbreak of methicillin-resistant Staphylococcus aureus among players on a college football team, facilitated by cosmetic body shaving and turf burns. Clin Infect Dis. 2004;39(10):1446–1453. doi: 10.1086/425313. et al. [DOI] [PubMed] [Google Scholar]
- 24.Romano R, Lu D, Holtom P. Outbreak of community-acquired methicillin-resistant Staphylococcus aureus skin infections among a collegiate football team. J Athl Train. 2006;41(2):141–145. [PMC free article] [PubMed] [Google Scholar]
- 25.Rutala WA. APIC guideline for selection and use of disinfectants: 1994, 1995, and 1996 APIC Guidelines Committee. Association for Professionals in Infection Control and Epidemiology, Inc. Am J Infect Control. 1996;24(4):313–342. doi: 10.1016/s0196-6553(96)90066-8. [DOI] [PubMed] [Google Scholar]
- 26.Larson EL. Antiseptics. In: Olmstad RN, editor. APIC Infection Control and Applied Epidemiology: Principles and Practices. St. Louis, MO: Mosby-Year Book, Inc; 1996. pp. 19–11.pp. 19–17.pp. G11–G17. [Google Scholar]
- 27.National Athletic Trainers' Association. Official statement from the National Athletic Trainers' Association on community-acquired MRSA infections (CA-MRSA) http://www.nata.org/sites/default/files/MRSA.pdf. Accessed November 8, 2010.
- 28.Siegel JD, Rhinehart E, Jackson M, Chiarello L, Health Care Infection Control Practices Advisory Committee Management of multidrug-resistant organisms in healthcare settings. Am J Infect Control. 2007;35(10 suppl 2):S165–S193. doi: 10.1016/j.ajic.2007.10.006. [DOI] [PubMed] [Google Scholar]
- 29.Siegel JD, Rhinehart E, Jackson M, Chiarello L, Health Care Infection Control Practices Advisory Committee 2007 Guideline for isolation precautions: preventing transmission of infectious agents in health care settings. Am J Infect Control. 2007;35(10 suppl 2):S65–S164. doi: 10.1016/j.ajic.2007.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Sehulster LM, Chinn RYW, Arduino MJ. Guidelines for Environmental Infection Control in Health-Care Facilities: Recommendations from CDC and the Healthcare Infection Control Practices Advisory Committee (HICPAC) Chicago, IL: American Society for Healthcare Engineering/American Hospital Association; 2004. et al. [Google Scholar]
- 31.Goding AM, Rainisch KJ, Cochran RL, Hageman JC, National Athletic Trainers' Association College and University Athletic Trainers Committee Athletic trainers and MRSA infections: what's the score? NATA News. May 2007:12–15. [Google Scholar]
- 32.Boyce JM, Pittet D, Healthcare Infection Control Practices Advisory Committee; HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force Guideline for hand hygiene in health-care settings: recommendations of the Health-care Infection Control Practices Advisory Committee and the HICPAC/SHEA/APIC/IDSA Hand Hygiene Task Force. Society for Healthcare Epidemiology of America/Association for Professionals in Infection Control/Infectious Diseases Society of America. MMWR Recomm Rep. 2002;2551(RR-16):1–45. [PubMed] [Google Scholar]
- 33.Centers for Disease Control and Prevention. Hand hygiene guidelines fact sheet. http://www.cdc.gov/media/pressre/fs021025.htm. Accessed November 8, 2010.
- 34.Environmental Protection Agency. EPA's registered products effective against methicillin resistant Staphylococcus aureus (MRSA) and vancomycin resistant Enterococcus faecalis or faecium (VRE) http://www.epa.gov/oppad001/list_h_mrsa_vre.pdf. Accessed November 8, 2010.
- 35.Snyder AR, Parsons JT, Valovich McLeod TC, Curtis Bay R, Michener LA, Sauers EL. Using disablement models and clinical outcomes assessment to enable evidence-based athletic training practice, part I: disablement models. J Athl Train. 2008;43(4):428–436. doi: 10.4085/1062-6050-43.4.428. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Mbithi JN, Springthorpe VS, Sattar SA. Chemical disinfection of hepatitis A virus on environmental surfaces. Appl Environ Microbiol. 1990;56(11):3601–3604. doi: 10.1128/aem.56.11.3601-3604.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Sagripanti JL, Bonifacino A. Bacterial spores survive treatment with commercial sterilants and disinfectants. Appl Environ Microbiol. 1999;65(9):4255–4260. doi: 10.1128/aem.65.9.4255-4260.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Sagripanti JL, Bonifacino A. Comparative sporicidal effects of liquid chemical agents. Appl Environ Microbiol. 1996;62(2):545–551. doi: 10.1128/aem.62.2.545-551.1996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Dominguez TJ. It's not a spider bite, it's community-acquired methicillin-resistant Staphylococcus aureus. J Am Board Fam Pract. 2004;17(3):220–226. doi: 10.3122/jabfm.17.3.220. [DOI] [PubMed] [Google Scholar]