

Abstract
The objective of this study was to determine the complication rate and evaluate factors affecting the outcome of olecranon osteotomy in dogs. Medical records were searched to identify dogs that had undergone olecranon osteotomy (stabilized with 2 Kirschner wires and a figure-of-8 wire) during internal fixation of a supracondylar or condylar humeral fracture. Signalment, description of the fracture, parameters regarding the osteotomy and its repair, and radiographic outcome were recorded. A logistic regression model compared patient and technical parameters with the osteotomy outcome. Of the 19 dogs, 7 (37%) had complications of the osteotomy, including osteomyelitis, loss of reduction, and improper placement and migration of the Kirschner wires. Olecranon osteotomy is associated with a high complication rate in dogs; however, there was no correlation between patient-related or technical parameters and the development of complications. Further clinical and biomechanical investigations are warranted to improve the results of olecranon osteotomy and its repair.
Introduction
Olecranon osteotomy is often performed in dogs to improve surgical exposure during the repair of distal (supracondylar or condylar) humeral fractures, to facilitate open reduction of elbow luxation, and to simplify exposure and implant application during elbow arthrodesis (1,2,3,4,5,6,7,8). In humans, olecranon fracture or osteotomy repair is frequently associated with complications, including pin migration, osteomyelitis, and failure of the tension-band mechanism (9,10,11,12,13,14,15,16,17,18). Olecranon osteotomy in dogs is purportedly associated with similar complications (1,2,3,4,5,19). Palmer, Aron and Chambers (2) reported that 9 of 16 dogs with olecranon osteotomies that were repaired with pin and tension-band wire fixation had complications, 6 of the dogs requiring a 2nd operation to replace or remove the implants (2). There have not been any published reports assessing outcome of and risk factors for olecranon osteotomy repairs in dogs. The objectives of this study were to determine the incidence of, and evaluate risk factors for, complications of olecranon osteotomy repair during internal fixation of distal humeral fractures in dogs.
Materials and methods
Medical records of all dogs with humeral fractures presented to the University of Florida, the Louisiana State University Veterinary Medical Teaching Hospitals, and the Northern Sydney Veterinary Specialist Center, New South Wales, Australia, between 1994 and 2000, were reviewed to identify dogs that had undergone open surgical reduction and stabilization of a supracondylar or condylar humeral fracture. Dogs were included in the study if an olecranon osteotomy had been performed and repaired by pin and tension-band fixation during repair of the humeral fracture and if there had been radiographic follow-up for at least 12 wk or until there was radiographic evidence of union of the osteotomy.
The following information was obtained from medical records: signalment, including body weight; classification of the fracture as supracondylar, intercondylar, or unicondylar; whether the fracture was open or closed; the duration of surgery; and whether antibiotics had been administered perioperatively or postoperatively. Objective parameters pertaining to the olecranon osteotomy and its repair were obtained from the mediolateral radiograph obtained immediately after the operation. The length of the olecranon segment was calculated by measuring the distance from the most proximal aspect of the olecranon to the midpoint of the osteotomy site (Figure 1a). The width of the olecranon segment was measured at the osteotomy site (Figure 1b). The width of the ulnar diaphysis was measured at a point equivalent to twice the distance from the proximal aspect of the olecranon to the lateral coronoid process of the ulna (Figure 1c). The olecranon segment length was then normalized for variations in patient size by dividing the length of the olecranon segment by the width of the ulnar diaphysis (a/c). Tension-band wire length (Figure 2a) was obtained by measuring the distance between the most proximal extent of the wire and the drill hole that accommodated the wire. The olecranon-to-drill-hole distance (Figure 2b) was ascertained by measuring the distance from the most proximal aspect of the olecranon to the center of the drill hole. An osteotomy ratio was then calculated by dividing the olecranon segment length by the olecranon-to-drill-hole distance. The implanted and total Kirschner wire lengths (Figure 3a and Figure 3b) were determined by measuring the mean length of Kirschner wire that was implanted in bone and the mean total length of the 2 implants, respectively. The position of the Kirschner wires from the cranial margin of the olecranon (Figure 4) was expressed as a percentage of the total width of the olecranon segment, such that the lower the percentage, the more cranially the Kirschner wires were positioned. The osteotomy reduction (Figure 5a) was defined as the cranial or caudal displacement (step) of the olecranon segment along the cranial surface of the olecranon. The osteotomy gap (Figure 5b) was measured at its greatest width. The superimposition of the osteotomy and the implants used to stabilize the humeral fracture limited the subjective assessment of the position of the Kirschner wires from the craniocaudal radiographic projections.
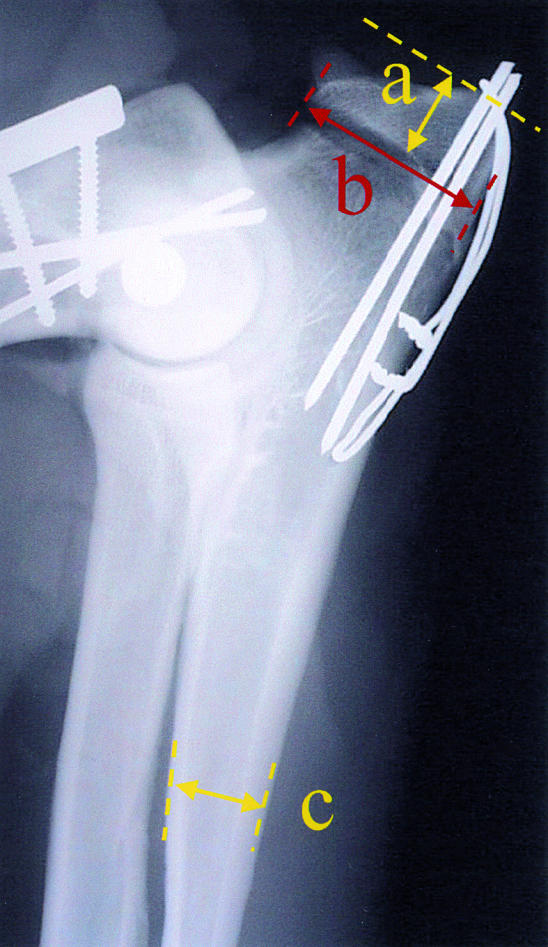
Figure 1. Postoperative mediolateral radiograph of an olecranon osteotomy repaired with pin and tension-band wire fixation, demonstrating the olecranon segment length (a) and width (b), the ulnar width (c), and the corrected olecranon length (a/c).
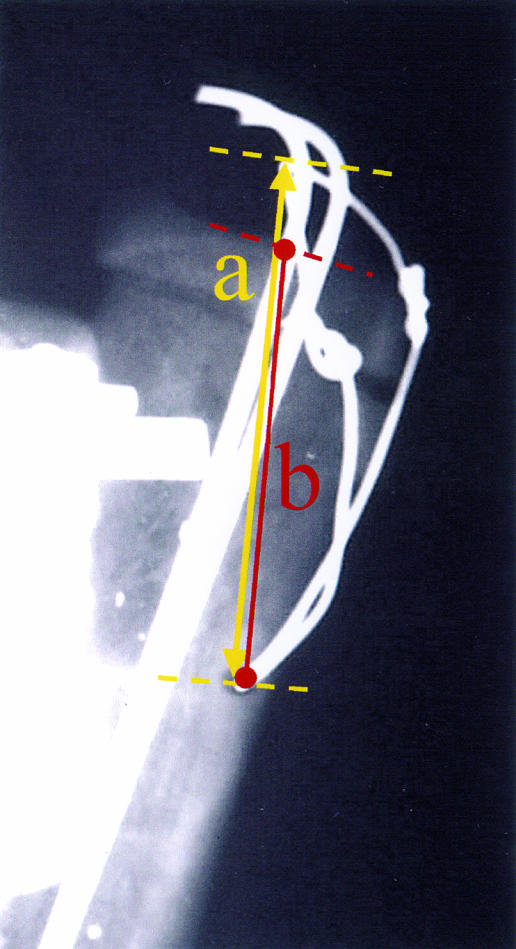
Figure 2. Postoperative mediolateral radiograph of an olecranon osteotomy repaired with pin and tension-band wire fixation, demonstrating the wire length (a) and the olecranon-to-drill-hole distance (b).
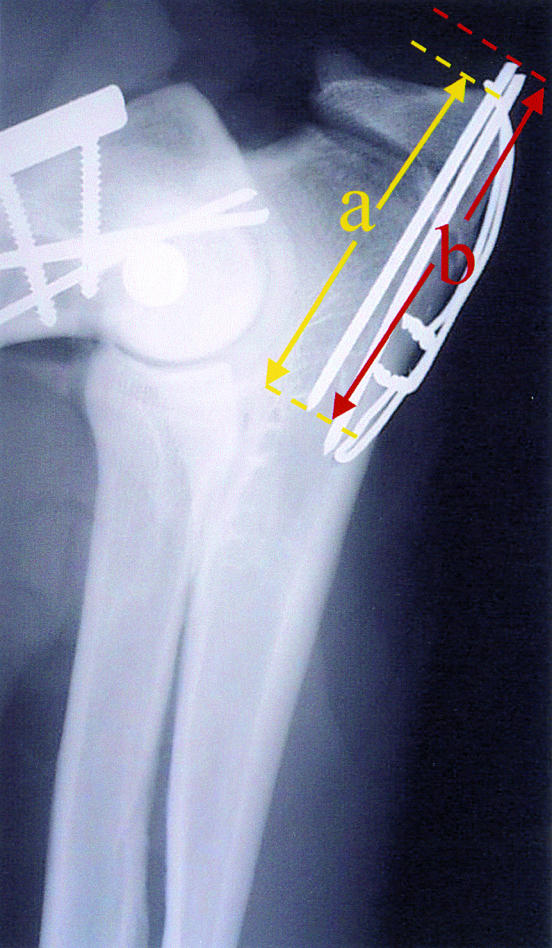
Figure 3. Postoperative mediolateral radiograph of an olecranon osteotomy repaired with pin and tension-band wire fixation, demonstrating the implanted (a) and total (b) Kirschner wire length.

Figure 4. Postoperative mediolateral radiograph of an olecranon osteotomy repaired with pin and tension-band wire fixation, demonstrating the Kirschner wire position (a/b × 100).

Figure 5. Postoperative mediolateral radiograph of an olecranon osteotomy repaired with pin and tension-band wire fixation, demonstrating the osteotomy reduction (a) and osteotomy gap (b).
Follow-up radiographs were used to assess outcome, on the basis of the width and definition of the osteotomy gap, the extent and character of callus formation and bone remodeling, and any change in the position of or lucency surrounding the implants. The outcome was defined according to whether the olecranon osteotomy healed uneventfully or with complications. A healed outcome was defined as having radiographic union of the osteotomy within 12 wk of surgery without developing complications. A complication with the olecranon osteotomy was defined as a failure to achieve radiographic union within 12 wk of surgical repair, loss of reduction of the olecranon segment, migration or failure of the Kirschner or tension band wires, irregular proliferative new bone formation or osseous radiolucencies suggestive of osteomyelitis, or the need for a second surgery to reposition or remove one or more of the tension band implants. Follow-up radiographs were similarly evaluated to determine whether the humeral fracture had healed uneventfully or there had been complications.
For the clinical and radiographic parameters, statistical differences between the dogs in which the osteotomy had healed with or without complications were evaluated by using a logistical regression model. Statistical analyses were performed with a standard software package (SAS Statistical Software, SAS Institute, Cary, North Carolina, USA). For all analyses, significance was defined as P < 0.05.
Results
Twenty-six dogs, in which supracondylar or condylar humeral fractures were surgically approached by using an olecranon osteotomy, were identified; for 19, there was adequate follow-up information for inclusion in the study. A summary of signalment and outcome for the 19 dogs is provided in Table 1. Both purebred and mixed-breed dogs were represented; 5 (26%) were cocker spaniels. Ages ranged from 4 mo to 10 y (mean: 3.9 y; median: 4.5 y). Body weights ranged from 4 kg to 36 kg (mean: 18 kg; median: 15 kg). Fifteen (79%) of the dogs had had closed fractures and 4 (21%) open fractures. The fixation method used to stabilize all of the osteotomies had consisted of 2 Kirschner wires and a figure-of-8 tension-band wire applied according to the traditional technique (6,7,8). Perioperatively, cefazolin, 22 mg/kg body weight, IV, q90 min, had been administered routinely to all the dogs; antibiotic administration was continued following surgery in the dogs with open fractures.
Table 1.

Twelve (63%) of the dogs had uneventful healing of the osteotomy. There were complications in the other 7 dogs (37%): osteomyelitis of the osteotomy site in 2 (11%), both dogs requiring a 2nd operation to remove the implants (Figure 6); loss of reduction in 1 (5%); osteomyelitis at the osteotomy site, with subsequent implant loosening and loss of reduction, in 1 (5%); loss of reduction, necessitating a 2nd operation to replace the pin and tension-band wire in 1 (5%), in which osteomyelitis subsequently developed (Figure 7); malposition of the Kirschner wire, necessitating a 2nd operation to reposition the implant, in 1 (5%); and migration of the Kirschner wire during the early postoperative period, necessitating surgical removal of the implant, in 1 (5%).

Figure 6. Immediate postoperative (a) and 5-wk follow-up (b) radiographs of dog no. 3, in which osteomyelitis developed at both the osteotomy and the humeral fracture sites.

Figure 6. Continued.

Figure 7. Immediate postoperative (a) and 5-wk follow-up (b) mediolateral elbow radiographs of dog no. 4, in which osteomyelitis developed at both the osteotomy and humeral fractures sites following a 2nd operation to restabilize the failed pin and tension-band mechanism.

Figure 7. Continued.
Although 3 of the 4 dogs with open fractures had complications with the olecranon osteotomy, only 4 of the 15 dogs with closed fractures developed complications; the difference was not significant different [odds ratio (OR) = 7.25; P = 0.24). Of the 5 dogs in which osteomyelitis of the humeral fracture developed, 4 also had osteomyelitis of the osteotomy (Figures 6 and 7); however, this association was not significant (OR = 2.53; P = 0.59). Logistic regression analysis did not identify a significant association between outcome and any patient-related parameter, the duration of surgery, or technical aspects of the osteotomy repair (Table 2).
Table 2.

Discussion
Our results corroborate previous observations (1,2,3,4,5,19) that dogs that have an olecranon osteotomy stabilized with pin and tension-band fixation frequently have complications. Our 37% complication rate may be somewhat inflated, as adequate postoperative evaluations were not available for 7 of the 26 dogs initially identified. We suspect that dogs with complications were more likely to be returned for follow-up evaluation than were dogs with uneventful healing. In addition, some of the dogs that by our definition had a complication may not have had any substantial morbidity. The outcome of the osteotomy repair was based principally on radiographic assessment and to a lesser extent on notes in the medical record. Four of the 7 dogs with complications ultimately had union of the osteotomy. The multi- institutional and retrospective nature of this study made it difficult to assess accurately to what extent, if any, elbow joint or forelimb function was compromised and to ascertain whether any compromise of function was due to the humeral fracture or to the olecranon osteotomy. Our 37% complication rate, however, is less than the 56% rate reported by Palmer et al (2) in their retrospective report on olecranon osteotomy repairs in dogs and comparable to that reported in association with olecranon osteotomy and fracture repair in humans (9,10,11,12,13,14,15,16,17,18). Also, in a retrospective study evaluating internal fixation of proximal ulnar fractures in dogs, implant failure was found to have occurred in 3 of 4 repairs in which a pin and tension-band wire technique was used (20).
Palmer et al (2) ascribed 25% (4/16) of the complications in their study to poorly positioned implants. Kirschner-wire migration or protrusion of implants into the soft tissues, producing disability, has been observed in up to 80% of humans with an olecranon fracture or osteotomy repaired by means of pin and tension-band fixation (9,12,17,18); however, these were infrequent problems in our study.
Among the 7 dogs with complications, 4 had osteomyelitis at the osteotomy site, which resulted in delayed union of the osteotomy in 3 and subsequent implant loosening and loss of reduction in 1. All 4 of these dogs had concurrent osteomyelitis of the fracture, which suggests that the osteotomy was secondarily involved. Internal fixation of distal humeral fractures is often technically difficult and may be associated with a prolonged operative time, so intraoperative contamination may have contributed to the high incidence of osteomyelitis. However, prophylactic antibiotic was routinely administered perioperatively to all the dogs, and the duration of surgery was not significantly associated with the osteotomy outcome. Further, 2 of the 4 cases of osteotomy osteomyelitis were in dogs with open fractures, which were likely contaminated when the fracture occurred.
We attempted to identify patient parameters that might have contributed to the development of postoperative complications. Patient-related factors, such as age, breed, and body weight, did not significantly influence the outcome of the osteotomy repair. This suggests that the complications are not simply a function of longer healing times in older dogs or the increased biomechanical demands of larger dogs. The dogs with open fractures had a 75% incidence of osteotomy complications, whereas the dogs with closed fractures had only a 27% incidence. Although this difference was not significant, the small number of dogs with open fractures may have precluded identification of this parameter as a significant risk factor.
We also attempted to identify technical parameters pertaining to the osteotomy and its repair that might have contributed to the development of complications. Owing to the size variability of both the implants and the patients, an effort was made to normalize the size of the olecranon segment by using a ratio of the length of the segment to the width of the ulnar diaphysis. Alternatively, body weight could have been used for this purpose; however, we felt that this would have been a less accurate reflection of the relative size of the olecranon. In humans, osteotomy configuration and reduction, as well as implant positioning and application technique, have been shown to be important in influencing the biomechanics and clinical success of olecranon osteotomy and fracture repair with pin and tension-band fixation (21,22,23,24).
Unfortunately, we were unable to establish a significant correlation between outcome and any of the technical parameters evaluated. In fact, while not statistically significant, the mean and median values for the osteotomy reduction were actually better in dogs with complications than in those with uneventful healing (Table 2). Our inability to establish a significant correlation between surgical technique and osteotomy outcome suggests that osteotomies repaired with tension-band fixation are predisposed to complications, despite apparently appropriate surgical fixation, and it may be that the curvature of the proximal region of the ulna makes it difficult to consistently tighten the figure-of-8 wire effectively.
Our results corroborate that olecranon osteotomy repaired by traditional pin and tension-band wire fixation has a high complication rate in dogs (2). The high rate suggests that it may be prudent to avoid performing an olecranon osteotomy unless it is absolutely necessary. Although the complexity of the fracture was not associated with the outcome of the osteotomy and its repair, 9 dogs, 5 with complications, had supracondylar or unicondylar fractures, which probably could have been exposed with other approaches that have a lower potential for morbidity (1,25,26,27,28,29,30,31,32,33). Our inability to identify patient-related or technical parameters that affected outcome demonstrates a need for further clinical and biomechanical investigation of pin and tension-band fixation of olecranon osteotomy and suggests that alternative methods of osteotomy stabilization (2,10,12,13,34,35) deserve further investigation. CVJ
Footnotes
Presented as an abstract at the 28th Annual Conference of the Veterinary Orthopedic Society, Lake Louise, Alberta, February 26, 2001, and as a poster at the 11th Annual Symposium of the American College of Veterinary Surgeons, Chicago, Illinois, USA, October 11, 2001.
College of Veterinary Medicine Journal Series Number 607.
Address correspondence to Dr. Krista B. Halling.
Reprints will not be available from the authors.
References
- 1.Guerin SR, Lewis DD, Lanz OI, Stallings JT. Comminuted supracondylar humeral fractures repaired with a modified type I external skeletal fixator construct. J Small Anim Pract 1998;39:525–532. [DOI] [PubMed]
- 2.Palmer RH, Aron DN, Chambers JN. A combined tension band and lag screw technique for fixation of olecranon osteotomies. Vet Surg 1988;17:328–332. [DOI] [PubMed]
- 3.Payne JT. Repair of complex elbow fractures. Proc Surgical Fixation of Fractures: a Course in AO/ASIF Techniques. Columbus, Ohio, 1999:9–10.
- 4.Denny HR. The humerus. In: Coughlan A, Miller A, eds. Manual of Small Animal Fracture Repair and Management. Cheltenham, England: British Small Animal Veterinary Association, 1998: 171–195.
- 5.De Haan JJ, Roe SC, Lewis DD, Renberg WC, Kerwin SC, Bebchuk TN. Elbow arthrodesis in twelve dogs. Vet Comp Orthop Traumatol 1996;9:115–118.
- 6.Birchard SJ, Bright RM. The tension band wire for fracture repair in the dog. Compend Cont Educ Pract Vet 1981;3:37–41.
- 7.Brinker WO, Hohn RB, Prieur WD. Manual of Internal Fixation in Small Animals. Berlin: Springer-Verlag, 1984:33–55.
- 8.Muller ME, Allgower M, Schneider R, Willenegger H. Manual of Internal Fixation. Techniques Recommended by the AO Group. Berlin: Springer-Verlag, 1991:427–452.
- 9.Danziger MB, Abramowitz AJ, Covall DJ, Whitelaw GP. Postoperative complications in the treatment of olecranon fractures using tension band wiring technique. Proc Symp Am Acad Orthop Surg, Washington, DC, 1992.
- 10.Fyfe IS, Mossad MM, Holdsworth BJ. Methods of fixation of olecranon fractures. An experimental mechanical study. J Bone Joint Surg Am 1985;67:367–372. [DOI] [PubMed]
- 11.Gainor BJ, Moussa F, Schott T. Healing rate of transverse osteotomies of the olecranon used in reconstruction of distal humeral fractures. J South Orthop Assoc 1995;4:263–268. [PubMed]
- 12.Gullahorn LJ, Carlson D, Schneid K. Effectiveness of screw versus figure-of-eight tension band wire fixation of olecranon fractures. Proc Symp Am Acad Orthop Surg, Orlando, FL, 2000.
- 13.Hume MC, Wiss DA. Olecranon fractures: a clinical and radiographic comparison of tension band wiring and plate fixation. Clin Orthop 1992;285:229–235. [PubMed]
- 14.Macko D, Szabo RM. Complications of tension-band wiring of olecranon fractures. J Bone Joint Surg Am 1985;67:1396–1401. [PubMed]
- 15.McKee MD, Kim J, Kebaish K, Stephen DJ, Kreder HJ, Schemitsch EH. Functional outcome after open supracondylar fractures of the humerus. The effect of surgical approach. J Bone Joint Surg Br 2000;82:646–651. [DOI] [PubMed]
- 16.Murphy DF, Greene WB, Gilbert JA, Dameron TB. Displaced olecranon fractures in adults: biomechanical analysis of fixation methods. Clin Orthop 1987;224:210–214. [PubMed]
- 17.Murphy DF, Greene WB, Dameron TB. Displaced olecranon fractures in adults: clinical evaluation. Clin Orthop 1987;224: 215–223. [PubMed]
- 18.Wolfgang G, Burke F, Bush D, et al. Surgical treatment of displaced olecranon fractures by tension band wiring technique. Clin Orthop 1987;224:192–204. [PubMed]
- 19.McDonald DE. Question 125. In: Lewis DD, Parker RB, Bloomberg MS, eds. Self-Assessment Colour Review of Small Animal Orthopaedics. London: Manson Publ, 1998:129–130.
- 20.Muir P, Johnson KA. Fractures of the proximal ulna in dogs. Vet Comp Orthop Traumatol 1996;9:88–94.
- 21.Petraco DM, Koval KJ, Kummer FJ, Zuckerman JD. Fixation stability of olecranon osteotomies. Clin Orthop 1996;333:181–185. [PubMed]
- 22.Voor MJ, Sugita S, Seligson D. Traditional versus alternative olecranon osteotomy. Historical review and biomechanical analysis of several techniques. Am J Orthop 1995;Suppl:17–26. [PubMed]
- 23.Prayson MJ, Williams JL, Marshall MP, Scilaris TA, Lingenfelter EJ. Biomechanical comparison of fixation methods in transverse olecranon fractures: a cadaveric study. J Orthop Trauma 1997;11: 565–572. [DOI] [PubMed]
- 24.Wu CC, Tai CL, Shih CH. Biomechanical comparison for different configurations of tension band wiring techniques in treating an olecranon fracture. J Trauma 2000;48:1063–067. [DOI] [PubMed]
- 25.Lenehan TM, Nunamaker DM. Lateral approach to the canine elbow joint by proximal ulnar diaphyseal osteotomy. J Am Vet Med Assoc 1982;180:523–530. [PubMed]
- 26.Chalman JA, Slocum B. The caudolateral approach to the canine elbow joint. J Am Anim Hosp Assoc 1983;19:637–641.
- 27.Dueland R. Triceps tenotomy approach for distal fractures of the canine humerus. J Am Vet Med Assoc 1974;165:82–86. [PubMed]
- 28.O'Driscoll SW. The triceps-reflecting anconeus pedicle (TRAP) approach for distal humeral fractures and nonunions. Orthop Clin North Am 2000;31:91–101. [DOI] [PubMed]
- 29.Turner TM, Hohn RB. Craniolateral approach for repair of condylar fractures or joint exploration. J Am Vet Med Assoc 1980;176: 1264. [PubMed]
- 30.Montgomery RD, Milton JL, Mann FA. Medial approach to the humeral diaphysis. J Am Anim Hosp Assoc 1988;24:433–438.
- 31.Wallace MK, Berg J. Craniolateral approach to the humerus with transection of the brachialis muscle. Vet Surg 1991;20:97–99. [DOI] [PubMed]
- 32.Piermattei DL. Approach to the supracondylar region of the humerus and the caudal humeroulnar part of the elbow joint. In: Piermattei DL, ed. An Atlas of Surgical Approaches to the Bones and Joints of the Dog and Cat. 3rd ed. Philadelphia: WB Saunders, 1993:154–157.
- 33.Sturgeon C, Wilson AM, McGuigan P, Lawes TJ, Muir P. Triceps tenotomy and double plate stabilization of “Y–T” fracture of the humeral condyle in three dogs. Vet Comp Orthop Traumatol 2000;13:34–40.
- 34.Aktuglu K, Ozsoy H. Ilizarov circular external fixator for open olecranon fractures: a report of 3 cases. Acta Orthop Scand 1999;70: 93–96. [DOI] [PubMed]
- 35.Kinik H, Us AK, Mergen E. Self-locking tension band technique. A new perspective in tension band wiring. Arch Orthop Trauma Surg 1999;119:432–434. [DOI] [PubMed]