

Abstract
Context:
A database describing the range of normal rotator cuff strength values in uninjured high school pitchers has not been established. Chronologic factors that contribute to adaptations in strength also have not been established.
Objectives:
To establish a normative profile of rotator cuff strength in uninjured high school baseball pitchers and to determine whether bilateral differences in rotator cuff strength are normal findings in this age group.
Design:
Cohort study.
Setting:
Baseball playing field.
Patients or Other Participants:
A total of 165 uninjured male high school baseball pitchers (age = 16 ± 1 years, height = 1.8 ± 0.1 m, mass = 76.8 ± 10.1 kg, pitching experience = 7 ± 2 years).
Main Outcome Measure(s):
Isometric rotator cuff strength was measured bilaterally with a handheld dynamometer. We calculated side-to-side differences in strength (external rotation [ER], internal rotation [IR], and the ratio of ER:IR at 90° of abduction), differences in strength by age, and the influence of chronologic factors (participant age, years of pitching experience) on limb strength.
Results:
Side-to-side differences in strength were found for ER, IR, and ER:IR ratio at 90° of abduction. Age at the time of testing was a significant but weak predictor of both ER strength (R2 = 0.032, P = .02) and the ER:IR ratio (R2 = 0.051, P = .004) at 90° of abduction.
Conclusions:
We established a normative profile of rotator cuff strength for the uninjured high school baseball pitcher that might be used to assist clinicians and researchers in the interpretation of muscle strength performance in this population. These data further suggested that dominant-limb adaptations in rotator cuff strength are a normal finding in this age group and did not demonstrate that these adaptations were a consequence of the age at the time of testing or the number of years of pitching experience.
Keywords: shoulder, muscle physiology, throwing
Key Points.
A normative population profile for rotational shoulder strength in uninjured high school pitchers has been established.
Side-to-side differences existed for external rotation strength, internal rotation strength, and ratio of external rotation to internal rotation strength.
External rotation strength and ratio of external rotation to internal rotation strength increased as age increased in the dominant limb.
Age at the time of testing did not predict internal rotation strength.
The number of years of pitching experience did not predict strength measurements in the dominant limb.
Shoulder injuries are prevalent among baseball athletes at all levels of play.1–3 Pitchers are particularly vulnerable to injury, with overuse rather than trauma dominating as the primary injury mechanism.1–5 The cause of chronic injury in this population is cumulative microtrauma from the repetitive, dynamic overhand motion used to pitch a baseball.6–8 Muscle weakness, specifically of the rotator cuff musculature, has been proposed as a possible risk factor for developing shoulder injury.5,9–12 In a 5-year prospective study of 207 professional baseball pitchers, Byram et al9 reported that pitchers who exhibited external rotation (ER) muscle weakness during the preseason were more likely to experience a subsequent injury that necessitated surgery. The authors concluded that assessing preseason muscle strength might be an effective strategy for identifying athletes at risk for injury and might provide the opportunity to prescribe training programs for injury prevention.9
Rotator cuff strength in the uninjured baseball athlete has been described.10–20 Bilateral strength differences, including less ER strength10,17,20 and greater internal rotation (IR) strength11,14,16 of the throwing shoulder than of the nonthrowing shoulder, have been reported. In addition, lower ER:IR strength ratios have been reported in the asymptomatic throwing shoulder than in the nonthrowing shoulder of the baseball athlete.11,13,16,18,20 This difference in ER:IR strength ratios results predominantly from the presence of greater dominant-limb internal rotators without a similar dominance effect in the external rotators.11,15 Despite the plethora of studies in which shoulder strength in baseball athletes has been described, a descriptive profile of rotator cuff strength in the uninjured high school baseball pitcher has not been established. Investigations in which researchers have described rotator cuff strength in this population have been limited by small sample sizes (range, 22–39 participants).16,18 Such small sample sizes are inadequate for capturing the broad range of normative values that might exist in an uninjured population. Consequently, what constitutes “normal” strength values for the high school pitcher is unclear. It is also unclear whether strength adaptations identified in the throwing limbs of collegiate and professional pitchers are present in this younger group of athletes.
Because of the critical functional role of the rotator cuff muscles, objective evaluation of shoulder IR and ER strength is important during rehabilitation of the injured thrower and in preparticipation evaluations.11 In baseball, prevention and treatment of injuries in the youth athlete provide unique opportunities to potentially minimize the likelihood of incurring degenerative injuries later in the playing career.6 Therefore, the primary purpose of our study was to establish a normative profile of rotator cuff strength in the uninjured high school baseball pitcher and to determine whether bilateral differences in rotator cuff strength are normal findings in this age group. We hypothesized that the high school pitcher would present with asymmetric rotator cuff strength. The secondary purpose of our study was to determine the influence of age at the time of testing and years of pitching experience on rotator cuff strength in this population. Specifically, we hypothesized that greater IR and less ER strength would be associated with advancing age and years of pitching experience because strength adaptations would become more pronounced with extended baseball participation.
METHODS
Participants
Volunteers for this study (n = 165) were uninjured male high school baseball pitchers recruited from a larger study sample (n = 210) described in part I of this 2-part study.21 Of these 165 participants (age = 16 ± 1 years, height = 1.8 ± 0.08 m, mass = 76.8 ± 10.1 kg, pitching experience = 7 ± 2 years), 37 were left-hand dominant and 128 were right-hand dominant. We defined the dominant arm as the arm with which the athlete threw a ball. The participants' height, mass, and years of pitching experience progressively increased as their ages increased (Table 1). To be eligible for participation in the study, the athletes were required to have competed the 3 consecutive years before the study primarily as a pitcher in organized baseball in any capacity, to be uninjured and unrestricted in baseball activities at the time of testing, and to be aged 14 to 18 years. Athletes who had a history of upper extremity injury were eligible if they had made a full return to baseball participation at the time of testing. Uncompromised sports participation was validated with a Disabilities of the Arm, Shoulder and Hand Outcome Measure (Institute for Work & Health, Toronto, ON) sports score of 10% or less, with lower scores equating to higher levels of function. A musculoskeletal examination of both upper extremities was performed by an orthopaedic surgeon (K.M.K.) or board-certified sports physical therapist (W.J.H.) to confirm the absence of injury. Participants and parents provided written informed consent, and the research protocol was approved by the Mayo Clinic Institutional Review Board.
Table 1.
Participant Demographics
| Age Group, y | Limb Dominance, No. |
Height, m |
Mass, kg |
Pitching Experience, y |
||||
| Right | Left | Mean ± SD | Range | Mean ± SD | Range | Mean ± SD | Range | |
| 14 (n=19) | 16 | 3 | 1.75±0.09 | 1.60–1.96 | 68.20±12.10 | 54.00–92.25 | 4±1 | 3–6 |
| 15 (n=33) | 26 | 7 | 1.80±0.08 | 1.68–1.96 | 73.39± 11.16 | 56.25–94.50 | 6±2 | 3–9 |
| 16 (n=59) | 47 | 12 | 1.83±0.07 | 1.65–1.98 | 79.39±11.21 | 54.00–100.35 | 7±2 | 3–12 |
| 17 (n=45) | 33 | 12 | 1.85±0.07 | 1.70–2.01 | 81.46±9.53 | 54.55–105.75 | 7±2 | 3–12 |
| 18(n=9) | 6 | 3 | 1.85±0.08 | 1.70–1.93 | 81.62±6.46 | 72.27–92.27 | 9±2 | 7–13 |
Procedures
Before testing was initiated, all participants performed a 5- to 10-minute warmup consisting of stretching, jogging, and short-toss activities. Isometric muscle force was assessed with a handheld dynamometer (Commander PowerTrack II; JTECH Medical, Salt Lake City, UT) using a break test. The measurement range of the unit was 1 to 125 lb (0.45–56.25 kg), with a manufacturer-reported mechanical precision of 99%. Two examiners performed all strength testing, and an assistant recorded the results. The participant and examiner were blinded to the results. Trial-to-trial variability within and between examiners was less than 5 lb (2.25 kg). The validity and reliability of upper extremity strength assessment with handheld dynamometers have been established.22–24
The testing order was standardized and consisted of IR and ER strength of the right and left upper extremities. During testing, participants were seated on a bench or table without trunk support and with the hips and knees flexed to 90°. The seated position was chosen because it was considered more functional than the supine or prone position. During all tests, the limb was in 90° of abduction and modified neutral for shoulder rotation, with the elbow flexed to 90° (Figure 1). We chose the 90° abduction position because we considered it to be functional for the baseball athlete. Internal rotation positioning of the humerus during isometric strength testing was selected because this rotational position has been shown to promote high activity of the infraspinatus and subscapularis muscles while minimizing force contributions from other muscle groups.25 Participants could stabilize themselves by grasping the table with the nontesting limb.26 An assistant stabilized the distal aspect of the upper limb that was being tested26 and the contralateral shoulder to maintain consistent participant positioning throughout testing and to minimize any attempts at substitution. The point of resistance during testing was just proximal to the radial styloid process. The dynamometer was positioned on the dorsal surface of the limb during ER strength testing and on the volar surface during IR testing. Participants were taught the testing procedures and then performed 2 maximal-effort practice trials for each muscle group before testing began. Next, participants completed 2 trials that were each approximately 5 seconds in duration at each limb position, and they rested for a minimum of 30 seconds between trials.
Figure 1.
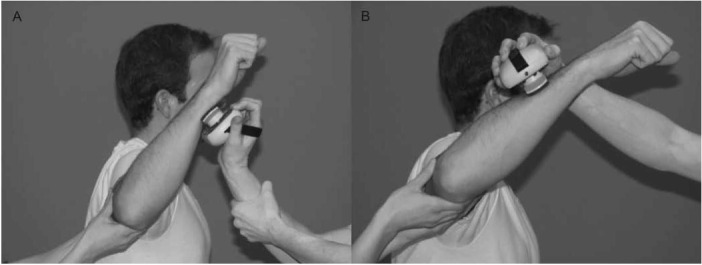
Participant positioning. A, Internal rotation strength testing. B, External rotation strength testing.
Data Analyses
Strength data were normalized to each person's mass to permit comparisons among participants. The peak values of the 2 trials for each motion were averaged and used for analysis. Paired t tests were performed to identify side-to-side differences in strength for the group. Differences in strength across age groups were evaluated with a univariate analysis of variance. When differences were identified, pairwise comparisons were performed using a post hoc Tukey test. Linear regressions were performed to determine the influence of participant age and years of pitching experience on dominant-limb strength. The α level was set a priori at .05. We used SPSS (version 19; SPSS Inc, Chicago, IL) for statistical analysis.
RESULTS
When evaluating side-to-side differences for the group, we found differences for all measures of interest (Table 2). External rotation strength was lower in the dominant than the non-dominant limb (t164 = 2.014, P = .046). Internal rotation strength was higher in the dominant than in the nondominant limb (t164 = −3.832, P < .001). Finally, the ratio of ER:IR strength was higher in the nondominant than the dominant limb (t164 = −5.125, P < .001).
Table 2.
Group Strength Results a
| Motion at 90° of Abduction | Dominant Limb |
Nondominant Limb |
P Value | t164 Value | ||
| Mean ± SD | 90% Confidence Interval | Mean ± SD | 90% Confidence Interval | |||
| External rotation | 17.5±4 | 12.2, 23.5 | 17.9±4 | 11.8, 23.9 | .046b | 2.014 |
| Internal rotation | 18.7±5 | 11.5, 27.1 | 17.7±4 | 10.7,26.8 | <.001b | −3.832 |
| External rotation to internal rotation ratio | 96±22 | 68.9, 132.6 | 105±23 | 74.3, 135.3 | <.001b | −5.125 |
a All strength values are reported as percentages of body mass.
b Indicates difference.
Across age groups, we found no differences in strength for the dominant limb (Table 3; Figure 2). For the nondominant limb, we found differences in the ratio of ER:IR strength (F4,160 = 3.958, P = .004), with the 14-year-old group demonstrating a lower ratio of ER:IR strength than the 16- and 17-year-old groups. We found no other differences in strength across age groups for the nondominant limb (Table 3; Figure 2).
Table 3.
Analysis of Variance for Comparison of Strength Across Age Groups
| Motion at 90° of Abduction | Limb | F4,160 Value | P Value |
| External rotation | Dominant | 2.139 | .08 |
| Nondominant | 2.364 | .06 | |
| Internal rotation | Dominant | 0.708 | .59 |
| Nondominant | 0.480 | .75 | |
| External rotation to internal rotation ratio | Dominant | 2.203 | .07 |
| Nondominant | 3.958 | .004a |
aIndicates difference.
Figure 2.
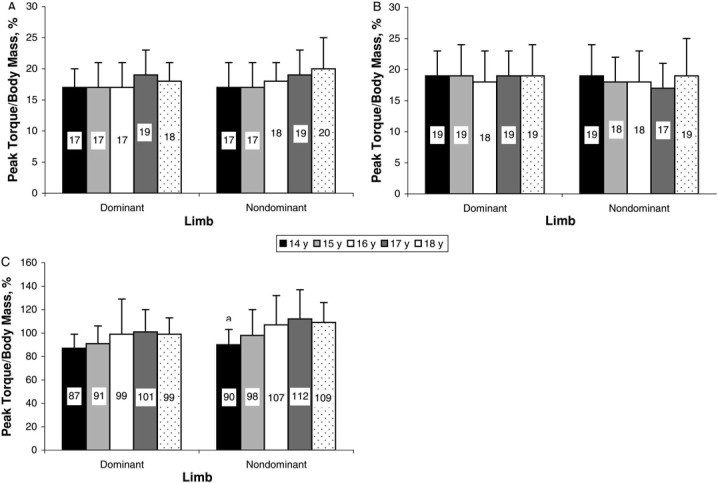
Strength of the dominant and nondominant limbs by age group. A, External rotation at 90° of abduction. B, Internal rotation at 90° of abduction. C, Ratio of external to internal rotation at 90° of abduction.a Indicates difference in strength across ages (F4,160 = 0.004, P<.05).
Participant age at the time of testing was a significant predictor of ER strength (R2 = 0.032, P = .02) and the strength ratio of ER:IR (R2 = 0.051, P = .004) at 90° for the dominant shoulder (Table 4). Strength increased with advancing age; however, the amount of variability in strength accounted for by the participant's age was small. Age at the time of testing did not predict IR strength, and years of pitching experience did not predict strength measurements in the throwing limb (Table 4).
Table 4.
Influence of Age at Testing and Years of Pitching Experience on Dominant-Limb Strength at 90° of Abduction
| R2 | P Value | |
| Age at testing | ||
| External rotation | 0.032 | .02a |
| Internal rotation | 0.001 | .74 |
| External rotation to internal rotation ratio | 0.051 | .004a |
| Years of pitching experience | ||
| External rotation | 0.009 | .22 |
| Internal rotation | 0.001 | .75 |
| External rotation to internal rotation ratio | 0.002 | .55 |
a Indicates difference.
DISCUSSION
Descriptive studies are necessary to enable effective and accurate data interpretation.27 By evaluating a large sample of athletes who were homogeneous in terms of age and position played, we provided a normative profile of rotator cuff strength in the uninjured high school baseball pitcher. Advantages of the data we reported include the ability to replicate the testing procedures in almost any setting with equipment that is widely available. Furthermore, these data add to the literature by providing an additional means for medical staff to assess rotator cuff strength beyond a side-to-side comparison. In the general population, a side-to-side comparison is often performed to identify deficits in muscle strength. Because of the demands placed on the dominant limb of an overhead athlete, strength in the dominant limb is not expected to be equivalent to that in the nondominant limb. Thus, population-specific strength data have been recommended for use in rehabilitation and prevention of shoulder injuries.11,28
Consistent with previous investigations10,11,14–18,20 and in agreement with our hypotheses, we identified side-to-side rotator cuff strength asymmetries in the uninjured baseball pitcher. External rotation strength was lower for the dominant than the nondominant limb. The opposite pattern was observed for IR strength because these muscles were stronger in the dominant limb. The 2 muscle groups function differently during the pitching motion. The internal rotators act concentrically during the acceleration phase of the pitching motion. Hinton16 described the muscle activity of the internal rotators during pitching as resembling a plyometric type of training, in which an explosive concentric muscle contraction (acceleration) follows a maximal stretch (limb cocking). Similar types of plyometric muscle training have been found to greatly enhance muscle power.29 In contrast, the external rotators act eccentrically during the deceleration phase of the pitching motion.30,31 Eccentric loading has been shown to cause intramuscular connective tissue tearing, which can lead to a cycle of chronic inflammation and muscular weakness.16,32,33 Thus, differences in the type of muscle contraction being performed during the pitching motion are potentially the source of limb-specific adaptations in muscle strength in this population.
Although we identified side-to-side differences in muscle strength, these differences were less than 1% for both IR and ER peak torque relative to body mass. The magnitude of these side-to-side differences falls within the range of our measurement error. Within-examiner and between-examiners variability for strength measures was less than 5 lb (2.25 kg), which translates to less than 3% peak torque/body mass measurement variability for the sample. Both examiners were trained by the primary investigator (W.J.H.), who has 16 years of experience as a physical therapist and is a board-certified sports physical therapist. Furthermore, all testing was performed under the visual supervision of the primary investigator to ensure that the same methods were used at all times.
When visually inspecting the distribution of strength values, we noted that the data set exhibited a normal bell-shaped curve with no skewness or kurtosis. Thus, we believe these values represent the range of what constitutes normal strength. Given that our primary purpose was to identify the range of strength values for the population, we believe the variability inherent to our strength measures is more than acceptable. Thus, these data suggest that in the high school pitcher, the strength of the dominant limb is similar to that of the nondominant limb.
It is unclear whether bilateral symmetry in strength is adequate for long-term effective and injury-free sports performance in this group of overhead athletes. Therefore, we advocate interpreting shoulder strength in the dominant limb of a baseball athlete using both a bilateral comparison and a comparison relative to normative population data to identify any limitations in muscle performance. Future studies that incorporate a prospective design will be necessary to determine whether a point exists at which inadequate muscle strength is a risk factor for injury or negatively affects pitching effectiveness.
The ratio of ER:IR strength was lower in the dominant limb (9%) than the nondominant limb. These results are consistent with those of previous investigators,11,13,16,18,20 who found the ratio of ER:IR strength to be lower in the dominant than the nondominant limb (range, 4%–11%) secondary to gains in IR strength of the dominant limb in the absence of corresponding gains in ER strength. A proper balance between agonist and antagonist muscle groups is thought to provide dynamic stabilization to the inherently unstable shoulder joint.28 The range of optimal ER:IR muscle strength in the overhead athlete has been defined as 66% to 75%.28,34 However, the strength ratios we reported are markedly higher than these previously reported values. In the thrower's position, we measured ER:IR strength ratios of 96% and 105% in the dominant and nondominant limbs, respectively (Table 2). However, most researchers who have evaluated shoulder strength in baseball pitchers have used isokinetic testing modes to assess concentric muscle strength at speeds ranging from 90°/s to 300°/s.13–16,20,35 In contrast, Donatelli et al,10 Magnusson et al,17 and Byram et al9 used handheld dynamometers to assess isometric rotator cuff strength in professional baseball pitchers. Using similar methods, these authors described ratios of ER:IR strength (range, 72%–142%) that were comparable to the results we reported. The discrepancy in strength performance during isokinetic compared with isometric muscle contractions might be explained, at least in part, by the force-velocity relationship. The greatest force production occurs during eccentric muscle contractions followed by isometric contractions, and high-speed contractions typically elicit the lowest muscle force.36 Strength assessed during an eccentric contraction is greatest secondary to internal muscle force production as the muscle is forcibly lengthened, which stresses the elastic components of the contractile structure.36 Isometric testing conditions result in greater force production than isokinetic testing because more time exists for cross-bridge formation, which is one of the primary contributors to force production, to be completed. Positioning the limb in midrange during isometric testing also takes advantage of the force-length principle, which stipulates that maximal force production is possible when optimal actin and myosin overlap is present.37 When the muscle is shortened or lengthened beyond the full resting length, the probability of actin and myosin interaction is less, and muscle tension decreases.37
Previous work supports this physiologic rationale as the basis for differences in the ER:IR strength ratios we identified. In isokinetic studies, researchers assessing eccentric muscle performance have reported higher eccentric ER to concentric IR strength ratios than researchers evaluating concentric performance of both muscle groups.19 Furthermore, Knapik et al38 reported that muscle torque production during strength testing was greater during isometric conditions than isotonic or isokinetic testing modes. It is possible that ER strength deficiencies elicited during isokinetic testing of the baseball athlete are a consequence of the testing mode and do not precisely capture the strength production capabilities of this muscle group. These results emphasize that differences exist in the type of information garnered based on the methods used for strength assessment. Thus, isometric assessment techniques might be more useful for identifying discrete strength deficits. Isokinetic strength assessment using high speeds and eccentric contractions might provide greater insight into functional performance in throwers, including muscle fatigability and speed of contraction. Information from both testing modes might be valuable in designing injury prevention and rehabilitation exercise programs.
The secondary purpose of our study was to identify chronologic factors that might affect dominant-limb strength in the uninjured high school baseball pitcher. Adaptations in shoulder strength associated with baseball participation have been described for athletes from high school to professional levels of play.14,16,19 Expecting more pronounced adaptations in muscle strength to be associated with physical maturation and longevity of sport participation would be reasonable. However, none of the chronologic variables we evaluated had a meaningful effect on shoulder rotational strength. We did not identify differences in strength for the dominant limb by age, and although age at the time of testing predicted ER strength and the ER:IR strength ratio, the amount of variability accounted for by the athlete's age was quite small. The ranges of ages and pitching experiences of our participants possibly were not large enough to capture the influence of chronologic characteristics on rotator cuff strength in the baseball pitcher. Alternatively, other factors, including the volume of throwing activities, might have an effect on muscle strength adaptations. We were unable to assess the influence of the number of innings pitched or pitches thrown on strength because we did not believe that a retrospective collection of this information could be captured with a high level of accuracy. We advocate that future investigators assess strength across a spectrum of ages and prospectively capture the volume of throwing activities to identify factors that contribute to muscle strength adaptations in the baseball pitcher.
Our study had limitations. It is important for clinicians to replicate the methods in this investigation when using the normative population data. Alternative testing positions or methods might affect muscle force production and thereby influence the interpretation of the athlete's strength. Multiple testing positions, including supine, prone, seated with support, and seated without support, have been described for assessment of rotator cuff strength. We performed strength testing in an unsupported, seated position to approximate a position of function for the baseball athlete and to facilitate reproduction of the study's methods in almost any environment. However, this position introduces the potential for compensatory motions and the inability to control scapular position. Substitutions were limited with instruction, practice, and use of a second examiner, and the participant was allowed to stabilize (ie, grasp the table) with the nontesting limb. The methods we used have been described. Tyler et al26 reported having a second examiner manually stabilize the limb of participants who were in a seated position. In addition, the seated position is often the position used during isokinetic testing.13,16,20 Bak and Magnusson39 described participants grasping the sitting surface with the nontesting limb during the strength assessment to increase stability. We acknowledge that the most functional assessment of muscle activity would be with the athlete standing and the muscles of interest working as a component of the whole-body kinetic chain. However, we believe the standing position would have introduced too much variability in the participant's ability to stabilize the trunk and upper extremity. Under these circumstances, the ability to accurately capture the force-producing capabilities of the rotator cuff musculature would be unacceptably compromised. Finally, our evaluation of the influence of age on strength adaptations included groups of unequal sizes. The 18-year-old age group included only 9 participants. Thus, associations between age and rotator cuff strength might have been masked in this investigation secondary to a small sample within this subgroup.
CONCLUSIONS
Isometric shoulder IR and ER strength was tested in 165 uninjured high school baseball pitchers. Strength data for these muscle groups and the ratio of ER:IR strength established a normative profile of rotational shoulder strength for the high school baseball pitcher. These data are important for clinicians to use when interpreting strength performance in athletes who are attempting to return to play after an injury and when individualizing training enhancement programs. These data also suggested that unilateral adaptations in dominant-limb strength are a normal finding in these young athletes.
REFERENCES
- 1.Collins CL, Comstock RD. Epidemiological features of high school baseball injuries in the United States, 2005– 2007. Pediatrics. 2008;121(6):1181–1187. doi: 10.1542/peds.2007-2572. [DOI] [PubMed] [Google Scholar]
- 2.Conte S, Requa RK, Garrick JG. Disability days in major league baseball. Am J Sports Med. 2001;29(4):431–436. doi: 10.1177/03635465010290040801. [DOI] [PubMed] [Google Scholar]
- 3.Dick R, Sauers EL, Agel J. Descriptive epidemiology of collegiate men' s baseball injuries: National Collegiate Athletic Association Injury Surveillance System, 1988–1989 through 2003–2004. J Athl Train. 2007;42(2):183–193. et al. [PMC free article] [PubMed] [Google Scholar]
- 4.Lyman S, Fleisig GS, Waterbor JW. Longitudinal study of elbow and shoulder pain in youth baseball pitchers. Med Sci Sports Exerc. 2001;33(11):1803–1810. doi: 10.1097/00005768-200111000-00002. et al. [DOI] [PubMed] [Google Scholar]
- 5.Wilk KB, Obma P, Simpson CD, Cain EL, Dugas JR, Andrews JR. Shoulder injuries in the overhead athlete. J Orthop Sports Phys Ther. 2009;39(2):38–54. doi: 10.2519/jospt.2009.2929. [DOI] [PubMed] [Google Scholar]
- 6.Andrews JR, Fleisig GS. Preventing throwing injuries. J Orthop Sports Phys Ther. 1998;27(3):187–188. doi: 10.2519/jospt.1998.27.3.187. [DOI] [PubMed] [Google Scholar]
- 7.Fleisig GS, Andrews JR, Dillman CJ, Escamilla RF. Kinetics of baseball pitching with implications about injury mechanisms. Am J Sports Med. 1995;23(2):233–239. doi: 10.1177/036354659502300218. [DOI] [PubMed] [Google Scholar]
- 8.Lyman S, Fleisig GS, Andrews JR, Osinski ED. Effect of pitch type, pitch count, and pitching mechanics on risk of elbow and shoulder pain in youth baseball pitchers. Am J Sports Med. 2002;30(4):463–468. doi: 10.1177/03635465020300040201. [DOI] [PubMed] [Google Scholar]
- 9.Byram IR, Bushnell BD, Dugger K, Charron K, Harrell FE, Jr, Noonan TJ. Preseason Shoulder strength measurements in professional baseball pitchers: identifying players at risk for injury. Am J Sports Med. 2010;38(7):1375–1382. doi: 10.1177/0363546509360404. [DOI] [PubMed] [Google Scholar]
- 10.Donatelli R, Ellenbecker TS, Ekedahl SR, Wilkes JS, Kocher K, Adam J. Assessment of shoulder strength in professional baseball pitchers. J Orthop Sports Phys Ther. 2000;30(9):544–551. doi: 10.2519/jospt.2000.30.9.544. [DOI] [PubMed] [Google Scholar]
- 11.Ellenbecker TS, Mattalino AJ. Concentric isokinetic shoulder internal and external rotation strength in professional baseball pitchers. J Orthop Sports Phys Ther. 1997;25(5):323–328. doi: 10.2519/jospt.1997.25.5.323. [DOI] [PubMed] [Google Scholar]
- 12.Trakis JE, McHugh MP, Caracciolo PA, Busciacco L, Mullaney M, Nicholas SJ. Muscle Strength and range of motion in adolescent pitchers with throwing-related pain: implications for injury prevention. Am J Sports Med. 2008;36(11):2173–2178. doi: 10.1177/0363546508319049. [DOI] [PubMed] [Google Scholar]
- 13.Alderink GJ, Kuck DJ. Isokinetic shoulder strength of high school and college-aged pitchers. J Orthop Sports Phys Ther. 1986;7(4):163–172. doi: 10.2519/jospt.1986.7.4.163. [DOI] [PubMed] [Google Scholar]
- 14.Brown LP, Niehues SL, Harrah A, Yavorsky P, Hirshman HP. Upper extremity range of motion and isokinetic strength of the internal and external shoulder rotators in Major League Baseball players. Am J Sports Med. 1988;16(6):577–585. doi: 10.1177/036354658801600604. [DOI] [PubMed] [Google Scholar]
- 15.Cook EE, Gray VL, Savinar-Nogue E, Medeiros J. Shoulder antagonistic strength ratios: a comparison between college-level baseball pitchers and nonpitchers. J Orthop Sports Phys Ther. 1987;8(9):451–461. doi: 10.2519/jospt.1987.8.9.451. [DOI] [PubMed] [Google Scholar]
- 16.Hinton RY. Isokinetic evaluation of shoulder rotational strength in high school baseball pitchers. Am J Sports Med. 1988;16(3):274–279. doi: 10.1177/036354658801600314. [DOI] [PubMed] [Google Scholar]
- 17.Magnusson SP, Gleim GW, Nicholas JA. Shoulder weakness in professional baseball pitchers. Med Sci Sports Exerc. 1994;26(1):5–9. [PubMed] [Google Scholar]
- 18.Mulligan IJ, Biddingtou WB, Barnhart BD, Ellenbecker TS. Isokinetic profile of shoulder internal and external rotators of high school aged baseball pitchers. J Strength Cond Res. 2004;18(4):861–866. doi: 10.1519/14633.1. [DOI] [PubMed] [Google Scholar]
- 19.Noffal GJ. Isokinetic eccentric-to-concentric strength ratios of the shoulder rotator muscles in throwers and nonthrowers. Am J Sports Med. 2003;31(4):537–541. doi: 10.1177/03635465030310041001. [DOI] [PubMed] [Google Scholar]
- 20.Wilk KE, Andrews JR, Arrigo CA, Keirns MA, Elber DJ. The strength characteristics of internal and external rotator muscles in professional baseball pitchers. Am J Sports Med. 1993;21(1):61–66. doi: 10.1177/036354659302100111. [DOI] [PubMed] [Google Scholar]
- 21.Hurd WJ, Kaplan KM, ElAttrache NS, Jobe FW, Morrey BF, Kaufman KR. A profile of glenohumeral internal and external rotation motion in the uninjured high school baseball pitcher, part I: motion. J Athl Train. 2011;47(3):282–288. doi: 10.4085/1062-6050-46.3.282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Byl NN, Richards S, Asturias J. Intrarater and interrater reliability of strength measurements of the biceps and deltoid using a hand held dynamometer. J Orthop Sports Phys Ther. 1988;9(12):395–398. doi: 10.2519/jospt.1988.9.12.395. [DOI] [PubMed] [Google Scholar]
- 23.Sullivan SJ, Chesley A, Hebert G, McFaull S, Scullion D. The validity and reliability of hand-held dynamometry in assessing isometric external rotator performance. J Orthop Sports Phys Ther. 1988;10(6):213–217. doi: 10.2519/jospt.1988.10.6.213. [DOI] [PubMed] [Google Scholar]
- 24.Magnusson SP, Gleim GW, Nicholas JA. Subject variability of shoulder abduction strength testing. Am J Sports Med. 1990;18(4):349–353. doi: 10.1177/036354659001800403. [DOI] [PubMed] [Google Scholar]
- 25.Kelly BT, Kadrmas WR, Speer KP. The manual muscle examination for rotator cuff strength: an electromyographic investigation. Am J Sports Med. 1996;24(5):581–588. doi: 10.1177/036354659602400504. [DOI] [PubMed] [Google Scholar]
- 26.Tylei TF, Nahow RC, Nicholas SJ, McHugh MP. Quantifying shoulder rotation weakness in patients with shoulder impingement. J Shoulder Elbow Surg. 2005;14(6):570–574. doi: 10.1016/j.jse.2005.03.003. [DOI] [PubMed] [Google Scholar]
- 27.Ellenbecker TS, Roetert EP, Sueyoshi T, Riewald S. A descriptive profile of age-specific knee extension flexion strength in elite junior tennis players. Br J Sports Med. 2007;41(11):728–732. doi: 10.1136/bjsm.2007.037085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. Am J Sports Med. 2002;30(1):136–151. doi: 10.1177/03635465020300011201. [DOI] [PubMed] [Google Scholar]
- 29.Radcliffe JC, Farentinos RC. Plyometrics: Explosive Power Training. Boulder, CO: Exer Technics Publishers; 1984. [Google Scholar]
- 30.Jobe FW, Moynes DR, Tibone JE, Perry J. An EMG analysis of the shoulder in pitching: a second report. Am J Sports Med. 1984;12(3):218–220. doi: 10.1177/036354658401200310. [DOI] [PubMed] [Google Scholar]
- 31.Jobe FW, Tibone JE, Perry J, Moynes D. An EMG analysis of the shoulder in throwing and pitching: a preliminary report. Am J Sports Med. 1983;11(1):3–5. doi: 10.1177/036354658301100102. [DOI] [PubMed] [Google Scholar]
- 32.Fox EL, Matthews DK. The Physiological Basis of Physical Education and Athletics. 3rd ed. Philadelphia, PA: Saunders College Publishers; 1981. pp. 152–155. [Google Scholar]
- 33.Nirschl R. Shoulder tendonitis. In: Pettrone FA, editor. American Academy of Orthopaedic Surgeons Symposium on Upper Extremity Injuries in Athletes: Washington, DC, June 1984. St Louis: CV Mosby; 1986. pp. 322–337. [Google Scholar]
- 34.Ellenbecker TS, Davies GJ. The application of isokinetics in testing and rehabilitation of the shoulder complex. J Athl Train. 2000;35(3):338–350. [PMC free article] [PubMed] [Google Scholar]
- 35.Wilk KE, Andrews JR, Arrigo CA. The abductor and adductor strength characteristics of professional baseball pitchers. Am J Sports Med. 1995;23(6):778. doi: 10.1177/036354659502300627. [DOI] [PubMed] [Google Scholar]
- 36.Lieber RL. Skeletal Muscle Structure, Function, & Plasticity: The Physiological Basis of Rehabilitation. 2nd ed. Baltimore, MD: Lippincott Williams & Wilkins; 2002. [Google Scholar]
- 37.Brooks GA, Fahey TD, Baldwin KM. Exercise Physiology: Human Bioenergetics and Its Applications. 3rd ed. New York, NY: McGraw-Hill Higher Education; 2000. [Google Scholar]
- 38.Knapik JJ, Wright JE, Mawdsley RH, Braun J. Isometric, isotonic, and isokinetic torque variations in four muscle groups through a range of joint motion. Phys Ther. 1983;63(6):938–947. doi: 10.1093/ptj/63.6.938. [DOI] [PubMed] [Google Scholar]
- 39.Bak K, Magnusson SP. Shoulder strength and range of motion in symptomatic and pain-free elite swimmers. Am J Sports Med. 1997;25(4):454–459. doi: 10.1177/036354659702500407. [DOI] [PubMed] [Google Scholar]