

Abstract
Objective
To assess the impact of the Patient Protection and Affordable Care Act's (ACA) changes in Medicare Advantage (MA) payment rates on the availability of and enrollment in MA plans.
Data Sources
Secondary data on MA plan offerings, contract offerings, and enrollment by state and county, in 2010–2011.
Study Design
We estimated regression models of the change in the number of plans, the number of contracts, and enrollment as a function of quartiles of FFS spending and pre-ACA MA payment generosity. Counties in the lowest quartile of spending are treated most generously by the ACA.
Principal Findings
Relative to counties in the highest quartile of spending, the number of plans in counties in the first, second, and third quartiles rose by 12 percent, 7.6 percent, and 5.4 percent, respectively. Counties with more generous MA payment rates before the ACA lost significantly more plans. We did not find a similar impact on the change in contracts or enrollment.
Conclusions
The ACA-induced MA payment changes reduced the number of plan choices available for Medicare beneficiaries, but they have yet affected enrollment patterns.
Keywords: Medicare, managed care, payment policy
The ACA and Medicare Advantage Plan Availability
The Patient Protection and Affordable Care Act (ACA) relied on reductions in Medicare Advantage (MA) payment rates to finance a significant portion of the subsidies associated with coverage expansion. These payment reductions were controversial because they have the potential to alter benefit generosity and the set of plan choices that Medicare beneficiaries will face in the future. Specifically, the MA program offers Medicare beneficiaries the option of receiving extra benefits if they enroll in a private health insurance plan (most commonly an HMO). In recent years, these plans have been paid at rates higher than the estimated spending for comparable individuals in the traditional fee-for-service (FFS) Medicare program. Because of several legislative changes dating back to 2004, in some counties MA payment rates and average FFS diverge significantly (Biles et al. 2009). MedPAC reports that, on average, MA payment rates were about 13 percent higher than FFS spending on comparable beneficiaries (Medicare Payment Advisory Commission 2010).
These generous payments promote a wide array of plan choices for Medicare beneficiaries (an important objective of the program, which prior to 2003 had been called Medicare + Choice). In fact, a commonly used diagnostic for the MA program is the availability of plans for beneficiaries (Medicare Payment Advisory Commission 2011). When plans exited in 1997 following the introduction of payment changes in the Balanced Budget Act (BBA), Congress responded by increasing payment rates to preserve plan choice. Thus, understanding the impact of payment reform on plan choice has important ramifications for maintaining the proposed payment rates.
The ACA has the potential to significantly alter this MA plan landscape. Under the new law, MA payment rates will be based on spending by FFS Medicare beneficiaries in each county. However, the generosity of MA payment will depend on the level of FFS spending. Specifically, counties in the lowest quartile of FFS spending will have their MA payment rates set at 115 percent of their average FFS spending level, those in the second quartile will have their rates set at 107.5 percent, those in the third quartile will have their rates set at 100 percent, and those in the highest quartile will have their rates set at 95 percent. While these changes will be implemented gradually (starting in 2012, and transitioning over a period of 2–6 years depending on the market), insurers likely have already anticipated the impact of these changes on their future stream of cash flows from the Medicare Advantage products they offered before the ACA was enacted in 2010. For 97 percent of all counties, these payment changes will result in reduced payment generosity. Therefore, insurers may have already removed some products from certain markets.
We investigate these issues by analyzing county-level changes between 2010 and 2011 in the number of MA plans and contracts offered in each county. “Contracts” measure the number of insurers offering a given type of plan, and “plans” measure the number of plans (and thus unique benefit packages) among which beneficiaries can choose. From the beneficiary perspective, the diversity of choice is largely captured by the number of plans they can choose (although plans offered by insurers under the same contract likely share the same provider network, so diversity of networks is better captured by the number of contracts). Moreover, in addition to measuring diversity of offerings, the number of contracts influences competition within the MA market. We hypothesize that counties that are scheduled to undergo a larger reduction in their payment rate due to the ACA rules should also experience a larger number of plan and contract exits.
We also investigate the impact of the ACA payment changes on beneficiary enrollment in MA plans. We are more agnostic about any effects on enrollment; while it is possible that any reductions in plan or contract availability may have altered MA enrollment patterns, it is also possible that many MA enrollees shifted to the contracts and plans that remain in place in 2011.
Background
Although a significant amount of research has been done on the MA program (McGuire, Newhouse, and Sinaiko 2011), there has been less work on the effects of payment rate changes on plan or contract availability. Cawley, Chernew, and McLaughlin (2005) investigated this question, identifying the impact of payment on plan availability by using MA payment changes in the BBA (which divorced MA payments from underlying FFS costs in each county). They found that during that time period, MA payment rates were below the level necessary to support even one MA plan in half of all U.S. counties. Pizer, Frakt, and Feldman (2003) utilized a similar natural experiment (payment rate changes in the Benefits Improvement and Protection Act) to evaluate how enrollees value the benefits offered by MA plans. Gold (2007) and Gold and colleagues (2009, 2010) have written a series of reports describing changes in the MA plan and contract availability in the period after the Medicare Modernization Act of 2003.
This body of work has demonstrated that the relationship between payment rates and plan availability has continued, and that changes in payment rates can also affect plan generosity (as measured by premiums and the out-of-pocket costs MA enrollees face). Other recent work has simulated the impact of payment rate changes similar to those in the ACA on the availability of private fee-for-service (PFFS) plans in the MA program (Frakt, Pizer, and Feldman 2009). The authors find that such changes would lead to a dramatic reduction in the participation of these plans. We are not aware of any research that has evaluated the impact of the recent reforms in the ACA on MA plan availability.
Methods
Data Sources
We used data from the Centers for Medicare and Medicaid Services (CMS). Specifically, we obtained data on MA offerings and enrollment by county in 2010 and 2011, benchmark payment rates by county in 2010 (Center for Medicare and Medicaid Services 2011c), and the most recent CMS data available on FFS costs by county, from 2008 (Center for Medicare and Medicaid Services 2011a). We also obtained data on MA plan quality ratings at the state level (Jacobson, Neuman, and Huang 2009).
We restricted attention to counties or county equivalents in the 50 states and the District of Columbia. We dropped Loving County, Texas, from the analysis, which had only 12 Medicare beneficiaries in 2010. Our final analysis file contained data on 3,139 counties.
Dependent Variables
We calculated the number of MA “contracts” and plans offered by insurers in each county in 2010 and 2011. (Using the terminology employed by CMS, insurers enter into a contract to sell a particular type of MA product in a given county or set of counties. Under each of these contracts, insurers may offer multiple plans, such as those with more or less generous benefit structures.) Each of these dependent variables captures a different potential response by insurers to the new payment rates. A reduction in the number of contracts would suggest that insurers are exiting counties altogether (since most insurers offer only a single contract for each plan type in a given county), while a reduction in the number of plans would indicate a reduction the diversity of each insurer's product offering in a county.
We restricted attention to three plan types: local HMO plans, local PPO plans, and regional PPO plans. Each of these plan types requires insurers to set up and maintain a network of providers. PFFS plans are also an important part of the MA landscape, and insurer offerings of these plans were also likely affected by the ACA payment rules. However, PFFS plan availability has also been influenced by the Medicare Improvements for Patients and Providers Act of 2008 (MIPPA). The MIPPA rules require that PFFS plans must use networks of contracted providers by 2011. Developing such a network is especially difficult in many of the markets where these plans have thrived in recent years, such as rural counties. CMS statistics indicate that the number of PFFS plans and enrollees declined between 2008 and 2010 as a result of these changes; there were 1.9 million Medicare beneficiaries enrolled in 77 PFFS contracts in January 2008, compared with 560,000 beneficiaries enrolled in 28 contracts in January 2011 (Center for Medicare and Medicaid Services 2008, 2011b). Because the MIPPA rules may complicate our ability to assess the impact of the PPACA on PFFS plans, our primary analysis does not assess changes in PFFS plan availability. (We do consider PFFS plans in our sensitivity analyses, and we control for PFFS enrollment in our main analysis of the availability of HMO and PPO plans.)
We also excluded plan types that are not paid on a capitated basis. Because employer-specific plans and “special needs” plans are not available to all Medicare beneficiaries, we excluded them from the analysis. The final file contained 23,207 and 23,039 plan-county records for 2010 and 2011, respectively, from which we calculated our yearly plan counts for each county. The analogous figures for the number of contracts were 10,313 and 10,765 in 2010 and 2011, respectively.
We also investigated the impact of the ACA payment changes on beneficiary enrollment in MA plans using the fraction of all Medicare beneficiaries enrolled in the set of plans described above.
Independent Variables
Our primary independent variables describe the expected generosity of payments after implementation of the ACA. We estimated the payment rates that will prevail under the new MA payment regime using county FFS costs in 2008. Although the FFS-based payment rates in future years will depend upon differential changes in FFS costs across counties during the next several years, we are limited to these 2008 figures for the current analysis. Because MA payment rates under the ACA are based on dividing counties into quartiles of FFS spending, our analysis relies heavily on these quartile categories for each county. While over time counties may change quartiles, the current quartile is likely predictive of future payment rates.
We also examine the impact of past generosity on changes in plan offerings. We estimated past generosity as the difference between each county's MA benchmark payment rate from 2010 and their FFS costs in 2008. For example, if a county's benchmark rate were $800 per enrollee per month (leaving aside any risk adjustment for the enrollee's health status), and if the average FFS cost level were $700, the generosity of payment in that county would be $100.
In all analyses we control for county population (in deciles). Because changes in PFFS offerings and enrollment may impact HMO and PPO offerings and especially enrollment, we also control for percent of Medicare beneficiaries in a county enrolled in a PFFS plans in 2010. Finally, because the ACA also made MA payment changes related to plan quality scores, we include a state-level summary of the percentage of all contracts operating in the state with a quality rating of four or five stars. By controlling for all of these factors, our regression analyses provide a more precise estimate of the new ACA rules than simple tabulations would.
Statistical Analysis
To estimate the impact of the ACA payment rate changes on MA contract and plan offerings, we ran two versions of the following fixed effects Poisson regression:
| (1) |
In this model, we regressed the count of plans or contracts (Yct) in county c and year t (2010 and 2011) on a set of county dummies (αc), a year dummy (γt), and a set of variables that vary by time and county (xct, all of which are interacted with the year dummy): four quartile indicator variables (one omitted), the 2010 MA monthly payment generosity level in dollars, the county's overall population (in ten decile indicator variables, one omitted), county PFFS enrollment in 2010, and state-level plan quality ratings. The fixed effects formulation of the Poisson regression model controls for time-invariant county-level variables and estimates the impact of past and future payment generosity on within-county changes in offerings.
To estimate the impact of the ACA payment rate changes on MA enrollment, we ran the following fixed effects linear regression:
| (2) |
where MAct is the fraction of total Medicare beneficiaries in county c enrolled in an HMO or PPO plan in year t. As was the case with the contract and plan count models, we include county fixed effects and the same set of time-varying covariates from the models described above. In a linear model with two time points this is equivalent to modeling the change in enrollment in a county as a function of expected future generosity (in quartiles), past generosity level, county population, PFFS enrollment in 2010, and fraction of plans with high quality ratings. In contrast to the plan and contract count models, we ran this regression using the county number of Medicare beneficiaries as weights.
Results
In Table 1, we present the distribution of the number of plans and contracts and MA enrollment across counties. The median county had three contracts and six plans in both 2010 and 2011, with approximately 8 percent of all Medicare beneficiaries enrolled in an MA plan. A majority of counties experienced little or no change in the number of plans, contracts, or MA enrollment. It should be noted that these un-weighted figures might understate the differences in plan availability across quartiles. Recent work by Gold and colleagues indicates that counties in the lowest FFS spending quartile contain only 16 percent of the Medicare population (Gold et al. 2011).1 The results presented in Table 1 also indicate significant variation in generosity across counties. 2
Table 1.
Descriptive Statistics
| Minimum | 25th Percentile | Median | 75th Percentile | Maximum | |
|---|---|---|---|---|---|
| Number of plans, 2010 | 0 | 3 | 6 | 9 | 55 |
| Number of plans, 2011 | 0 | 3 | 6 | 9 | 50 |
| Change in plans | −9 | −1 | 0 | 0 | 7 |
| Number of contracts, 2010 | 0 | 2 | 3 | 4 | 27 |
| Number of contracts, 2011 | 0 | 2 | 3 | 4 | 27 |
| Change in contracts | −3 | 0 | 0 | 0 | −3 |
| MA enrollment, 2010 | 0 | 3.6% | 7.7% | 14.2% | 50.7% |
| MA enrollment, 2011 | 0 | 3.8% | 7.9% | 14.2% | 55.5% |
| Change in MA enrollment | −15.9% | −0.2% | 0.4% | 1.2% | 16.0% |
| MA payment generosity, 2010 | −489 | 79 | 137 | 188 | 752 |
Note. all figures are based on data from HMO and PPO MA plans only.
Source: CMS's “Medicare Options Compare” files for 2010–2011, contract-plan-state-county enrollment data for 2010–2011, and Ratebook data for 2010–2011.
Tables 2a–c describe the change in the average number of plan, contracts, and MA enrollment, respectively, by quartile and year. Table 2a suggests that, despite little change in the overall number of plans, the new MA payment rules in ACA have influenced plan availability. Specifically, the ACA rules encouraged plan entry in some counties and hastened plan exit in others. Counties in the lowest quartile of spending, where MA plans will be paid relatively generously relative to FFS costs, saw the number of plans offered increase by 0.3 plans on average. The average number of plans in 2010 in these counties was 5.9. Quartile 2 counties experienced a smaller increase of 0.1 plans, and quartile 3 counties saw a small reduction of 0.1 plans. Counties in the highest quartile of spending, where plans will be paid less generously relative to FFS costs, saw the largest reduction, 0.6 plans. The average number of plans in 2010 in these counties was 9.0.
Table 2.
(a) Number of Plans by FFS Spending Quartile, 2010–2011. (b) Number of Contracts by FFS Spending Quartile, 2010–2011. (c) MA Enrollment by FFS Spending Quartile, 2010–2011
| Number of Plans, 2010 | Number of Plans, 2011 | Change, 2010–2011 | |
|---|---|---|---|
| (a) | |||
| Quartile 1 (lowest spending) | 5.9 | 6.2 | 0.3 |
| Quartile 2 | 7.0 | 7.1 | 0.1 |
| Quartile 3 | 7.7 | 7.6 | −0.1 |
| Quartile 4 (highest spending) | 9.0 | 8.4 | −0.6 |
| Total | 7.4 | 7.3 | −0.1 |
| Number of Contracts, 2010 | Number of Contracts, 2011 | Change, 2010–2011 | |
|---|---|---|---|
| (b) | |||
| Quartile 1 (lowest spending) | 2.7 | 2.9 | 0.2 |
| Quartile 2 | 3.2 | 3.4 | 0.2 |
| Quartile 3 | 3.4 | 3.5 | 0.1 |
| Quartile 4 (highest spending) | 3.8 | 3.9 | 0.1 |
| Total | 3.3 | 3.4 | 0.1 |
| MA Enrollment, 2010 | MA Enrollment, 2011 | Change, 2010–2011 | |
|---|---|---|---|
| (c) | |||
| Quartile 1 (lowest spending) | 17.3% | 17.9% | 0.6% |
| Quartile 2 | 15.0% | 15.7% | 0.7% |
| Quartile 3 | 15.2% | 15.8% | 0.6% |
| Quartile 4 (highest spending) | 17.7% | 18.4% | 0.7% |
| Total | 16.5% | 17.2% | 0.7% |
Note. all figures are based on data from HMO and PPO MA plans only. Plan and contract counts are unweighted; enrollment amounts are weighted by Medicare population.
Source: CMS's “Medicare Options Compare” files for 2010–2011, contract-plan-state-county enrollment data for 2010–2011, and Ratebook data for 2010–2011.
Table 2b describes a similar story for MA contracts, although in contrast to the results for MA plans, in all quartile categories the average number of contracts increased. In quartile 1 counties the average number of contracts increased by 0.2 (off of a 2010 base of 2.7), while in quartile 4 counties the number of contracts increased by only 0.1 contracts (off of a 2010 base of 3.8). Table 2c illustrates that MA enrollment increased slightly during the study period, in the range of 0.6 percent to 0.7 percent across all quartile groups.
Table 3 presents results from our regression models. The results from the Poisson plan count model indicate that there is a monotonic and positive relationship between the change in a county's number of plans offered in 2011 versus 2010 and the generosity of MA payments relative to FFS costs under the ACA rules. When converted from the log scale, the parameter estimates imply that compared with the highest spending quartile counties in the lowest, second lowest, and second highest spending quartiles experienced increases in the number of plans of 12.0 percent (p = .003), 7.6 percent (p = .018), and 5.4 percent (p = .049), respectively.
Table 3.
Regression Results
| Change in the Number of Plans (log scale) | Change in the Number of Contracts (log scale) | Change in Enrollment | |
|---|---|---|---|
| Quartile 1 (lowest spending) | 0.114** (0.038) | 0.050 (0.055) | 0.27 (0.27) |
| Quartile 2 | 0.073* (0.031) | 0.020 (0.045) | 0.30%* (0.15) |
| Quartile 3 | 0.053* (0.027) | 0.010 (0.040) | 0.02% (0.12) |
| Generosity pre-PPACA ($100) | −0.030* (0.013) | −0.001 (0.019) | 0.17%*(0.07) |
p < .05.
p < .01.
Note. Regression model also includes county population dummies, PFFS penetration, and percent of plans with high quality ratings. All figures are based on data from HMO and PPO MA plans only. Plan and contract regressions are unweighted, enrollment regressions are weighted by Medicare population.
Source: CMS's “Medicare Options Compare” files for 2010–2011 and contract-plan-state-county enrollment data for 2010–2011.
The results also indicate that the level of MA payment generosity before the introduction of the ACA rules affected the change in the number of plans. For every 100 dollar increase in the generosity of payment pre-ACA, the number of plans exiting rose by 2.9 percent (p = .026). We interpret this as evidence that generous payment pre-ACA led to more plans in the pre period, which led to a higher exit rate in the post period at any given ACA payment level.
The analogous analysis of contracts reveals a similar pattern of results, but the effects are smaller and are not statistically significant. The coefficient estimates indicate that relative to the highest spending quartile, counties in spending quartiles 1, 2, and 3 experienced increases in the number of contracts of 5.2 percent, 2.0 percent, and 1.0 percent, respectively. Pre-ACA generosity was not associated with changes in contracts between 2011 and 2010.
The results from our analysis of changes in MA enrollment show that compared with counties in the highest spending quartile, enrollment increased by 0.27, 0.30, and 0.02 percentage points in quartiles 1, 2, and 3, respectively. However, only the result for quartile 2 is statistically significant. There is a positive and statistically significant result for the generosity variable, implying that more generous payment pre-ACA led to greater enrollment despite the reduction in the number of plans.
We performed a number of sensitivity analyses to assess the robustness of our main result on the change in the number of plans by FFS quartile. First, we assessed whether MIPPA induced reductions between 2010 and 2011 in PFFS plan offerings by quartile of FFS spending, which could have offset the pattern of non-PFFS plan changes we observed. We first analyzed the change in the number of PFFS plans as the dependent variable. If PFFS plans were dropped in the same counties where non-PFFS plans were added, then we should have seen a differential change in the plan count that was exactly the opposite as the pattern of our main result. We instead found that counties in quartiles 1 and 2 saw relatively fewer plans exit than counties in quartile 4, a pattern similar to our result for HMO and PPO plans. Second, we analyzed the change in the number of all plans—HMO, PPO, and PFFS—as the dependent variable. If new non-PFFS plans replaced PFFS plans that insurers retired, then there should be no differences in plan changes across quartiles. Running the regression on this new dependent variable did not fundamentally change the magnitude or statistical significance of our main result; only the coefficient for quartile 3 was reduced in magnitude and statistical significance. Essentially, while it is true that PFFS plans were exiting the market, the pattern does not indicate that the changes offset any of the non-PFFS plan changes we have documented.
A related concern is that the change in plans we have documented is due to efforts on the parts of both insurers and CMS to reduce redundant plan offerings or plans with low enrollment. To address this issue, we performed two related sensitivity analyses. For the first analysis, we constructed a measure of the average number of plans per contract in each county at baseline, and added it as an independent variable to our regression model of the change in the number of plans. For the second analysis, we calculated the percentage of plans that were part of a contract with four or more plans, and added it as an independent variable. Each of these variables should capture the relative prevalence of low enrollment or duplicate plans across the four payment quartiles. In both of these analyses, our main result was unchanged.
One final concern with our results regarding the number of plans is that we simply may be picking up a trend in plan availability. Perhaps it is the case that the number of plans was already in decline, and the rate of reduction was higher in counties with higher levels of FFS spending. To investigate this possibility, we replicated our plan count analysis using data from 2009 and 2010. The results do not support the idea that there was a trend in the decline in plans. Compared with the highest spending quartile, the number of plans in the lowest spending quartile actually declined by 8.9 percent (p = .03).3
Discussion
An important objective of the Medicare Managed Care program, in all its incarnations, has been to promote choice. The payment methodology prior to ACA supported this goal by setting generous payment rates. By revising the payment system ACA ameliorated the overpayment problem. Our results demonstrate that this led to a reduction in plan options for beneficiaries and the analysis suggests that this may have reduced the number of insurers offering different plan types in less generous counties (measured by contracts). Those beneficiaries residing in counties that offered generous MA payment pre-ACA faced larger reductions in MA plan availability. However, we observed few changes in the number of contracts or in MA enrollment associated with these changes in generosity and offerings. It is likely that changes in the number of contracts respond more slowly, as changing contracts is likely more costly for firms. The lack of changes in enrollment suggests that despite reduction in plan availability, enrollee demand for MA remains. It may be the case that when payment rates actually fall, premiums and benefits will change and enrollment changes may follow. The reduction in plans could foreshadow future changes because plan changes reflect anticipated future cuts as insurers prepare for the post-ACA environment.
The normative conclusion from this finding depends on the value one places on plan diversity. Although beneficiary choice is good, overpaying to get that choice may not be. In addition, recent research indicates that a smaller number of plans may be more optimal, because the presence of too many plans causes “choice overload” and reduces enrollment in MA (McWilliams et al. 2011). Thus, policy makers must recognize the tradeoffs between payment generosity and other program objectives.
Our analysis has several limitations. Most notably, the change in MA payment generosity may have also affected the benefit generosity of the contracts and plans that remain in place. MA plan premiums and cost sharing amounts (e.g., the deductible level) may have increased. Investigating this topic is complicated by the multi-dimensional nature of plan generosity, the shifting availability of plans, and the fact that plan generosity reflects all of the counties served, as opposed to a single county. Thus, the investigation of the impact of payment on plan generosity remains a topic for future research. Second, we rely on plan anticipation of payment changes to identify effects and estimate future generosity based on 2008 FFS costs. Firms may have more recent and more relevant information. The actual effects on plan and contract availability may grow as we approach the end of the transition to the new payment system.
Despite these limitations, our analysis highlights the connection between payment and plan diversity. Given the nation's fiscal constraints, we cannot afford to pay more for MA beneficiaries than we would if they enrolled in the FFS Medicare program. Yet as this analysis demonstrates, payment reform will have ramifications beyond simply reducing spending. Plan choices will be affected. Ultimately, this will require policy makers to weigh fiscal needs with plan diversity.
Acknowledgments
Joint Acknowledgment/Disclosure Statement: This research was supported by a grant from the National Institute on Aging (grant no. P01 AG032952), and by the Marshall J. Seidman Program in Health Economics in the Department of Health Care Policy at Harvard Medical School. We thank James Livingston for valuable programming and data assistance. A previous version of this article was presented at the International Health Economics Association, 8th World Congress, Toronto, Canada, 12, July 2011.
Disclosures: None.
Notes
We thank a reviewer for making this point.
At baseline, generosity was $201 in quartile one, $132 in quartile two, $83 in quartile three, and $28 in quartile four.
The results from these sensitivity analyses are available from the authors upon request.
SUPPORTING INFORMATION
Additional supporting information may be found in the online version of this article:
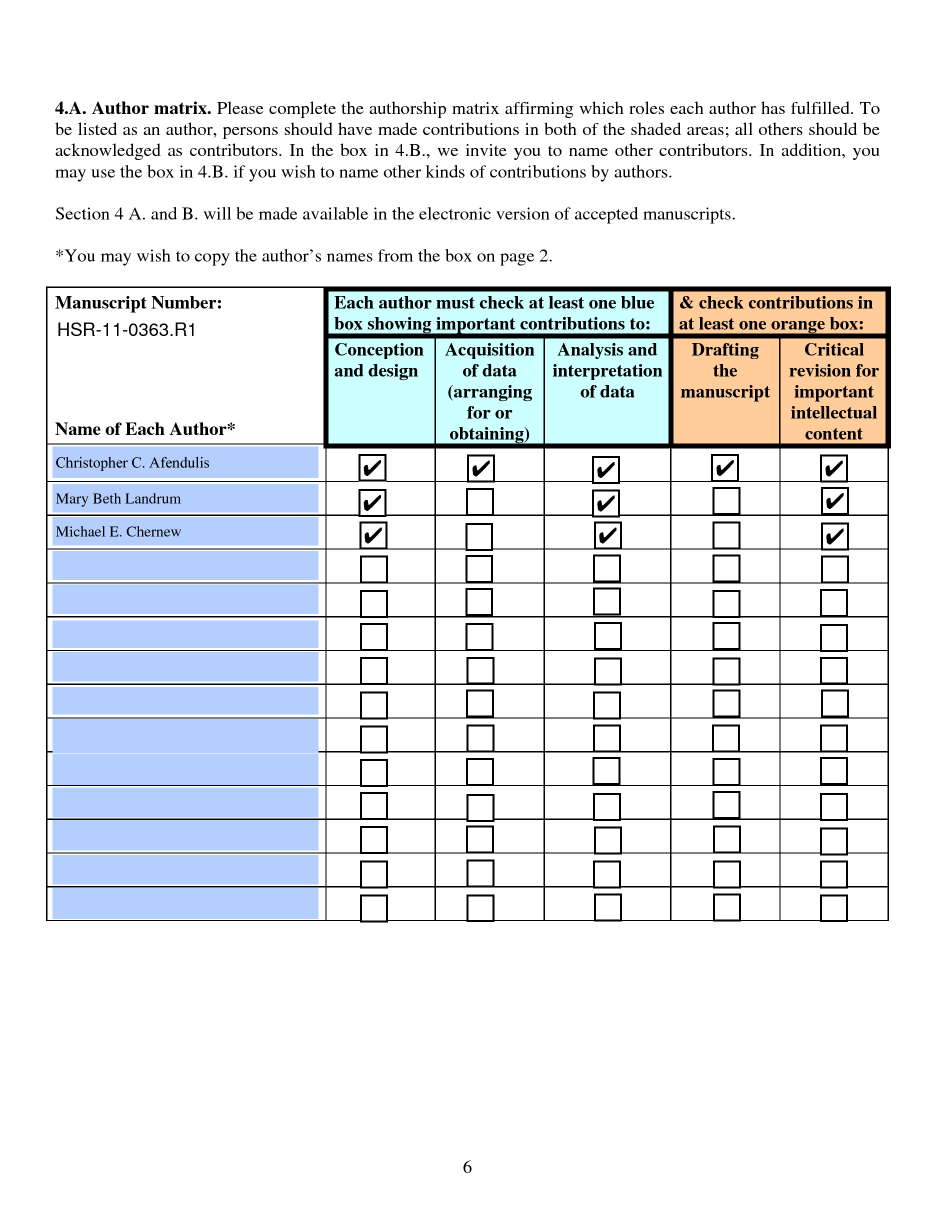
Appendix S1. Author Matrix.
{kind=link}
Please note: Wiley-Blackwell is not responsible for the content or functionality of any supporting materials supplied by the authors. Any queries (other than missing material) should be directed to the corresponding author for the article.
References
- Biles B, Pozen J, Guterman S. The Continuing Cost of Privatization: Extra Payments to Medicare Advantage Plans Jump to $11.4 Billion in 2009. New York: The Commonwealth Fund; 2009. [PubMed] [Google Scholar]
- Cawley J, Chernew M, McLaughlin C. “HMO Participation in Medicare + Choice”. Journal of Economics & Management Strategy. 2005;14(3):543–74. [Google Scholar]
- Center for Medicare and Medicaid Services. 2008. “Monthly Contract Summary Report–January 2008” [accessed on June 14, 2011]. Available at: http://www.cms.gov/MCRAdvPartDEnrolData/MCESR/list.asp.
- Center for Medicare and Medicaid Services. 2011a. “FFS Data Medicare Advantage–Rates & Statistics” [accessed on June 14, 2011]. Available at: http://www.cms.gov/MedicareAdvtgSpecRateStats/05_FFS_Data.asp.
- Center for Medicare and Medicaid Services. 2011b. “Monthly Contract Summary Report–January 2011” [accessed on June 14, 2011]. Available at: http://www.cms.gov/MCRAdvPartDEnrolData/MCESR/list.asp.
- Center for Medicare and Medicaid Services. 2011c. “Ratebooks & Supporting Data” [accessed on June 14, 2011]. Available at: http://www.cms.gov/MedicareAdvtgSpecRateStats/RSD/list.asp.
- Frakt AB, Pizer SD, Feldman R. “Payment Reduction and Medicare Private Fee-For-Service Plans”. Health Care Financing Review. 2009;30(3):15–24. [PMC free article] [PubMed] [Google Scholar]
- Gold M. “Private Plans in Medicare: A 2007 Update”. Washington, DC: The Henry J. Kaiser Family Foundation; 2007. [Google Scholar]
- Gold M, Phelps D, Neuman T, Jacobson G. “Medicare Advantage 2010 Data Spotlight: Plan Availability and Premiums”. Washington, DC: The Henry J. Kaiser Family Foundation; 2009. [Google Scholar]
- Gold M, Phelps D, Neuman T, Jacobson G. “Medicare Advantage 2011 Data Spotlight: Plan Availability and Premiums”. Washington, DC: The Henry J. Kaiser Family Foundation; 2010. [Google Scholar]
- Gold M, Jacobson G, Damico A, Neuman T. “Medicare Advantage Enrollment Market Update”. Washington, DC: The Henry J. Kaiser Family Foundation; 2011. [Google Scholar]
- Jacobson G, Neuman T, Huang J. What's in the Stars? Quality Ratings of Medicare Advantage Plans, 2010. Washington, DC: The Henry J. Kaiser Family Foundation; 2009. [Google Scholar]
- McGuire TG, Newhouse JP, Sinaiko AD. “An Economic History of Medicare Part C”. Milbank Quarterly. 2011;89(2):289–332. doi: 10.1111/j.1468-0009.2011.00629.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McWilliams JM, Afendulis CC, McGuire TG, Landon BE. “Complex Medicare Advantage Choices May Overwhelm Seniors–Especially Those with Impaired Decision Making”. Health Affairs. 2011;30(9):1786–94. doi: 10.1377/hlthaff.2011.0132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Medicare Payment Advisory Commission. Report to the Congress: Medicare Payment Policy. Washington, DC: MedPAC; 2010. [DOI] [PubMed] [Google Scholar]
- Medicare Payment Advisory Commission. Report to the Congress: Medicare Payment Policy. Washington, DC: MedPAC; 2011. [Google Scholar]
- Pizer SD, Frakt AB, Feldman R. “Payment Policy and Inefficient Benefits in the Medicare + Choice Program”. International Journal of Health Care Finance and Economics. 2003;3(2):79–93. doi: 10.1023/a:1023373630383. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.