

Abstract
Background: Adequate use of different learning strategies is one of the most important prerequisites of academic success. The actual use of learning strategies is the result of an interaction between individual and situational variables. Against this background we conducted a longitudinal study with first year medical students to investigate whether individuals show different patterns in their use of learning strategies and whether these patterns change during the first academic year.
Methods: Medical students (N=175, 58% female) were surveyed three times in their first academic year regarding their use of learning strategies. A hierarchical cluster analysis (Ward) was conducted in order to identify groups of students with different patterns of learning strategies.
Results: We identified four different patterns in approaches to learning among novice medical students (“easy-going”, “flexible”, “problematic” and “hardworking” learners). Compared to their peers, the problematic learners had the worst final school grades. In addition changes in the use of learning strategies were identified, most of them occurred during the first term.
Conclusion: Students start their academic studies with different patterns of learning strategies; the characteristics of these patterns change during the first academic year. Further research is necessary to better understand how individual and situational variables determine students’ learning.
Keywords: medical education, undergraduate, learning, learning strategies, Germany
Abstract
Hintergrund: Verschiedene Lernstrategien zweckmäßig zu nutzen, ist eine der wichtigsten Voraussetzungen für Lernerfolg. Welche Lernstrategien tatsächlich genutzt werden, ist abhängig von der Interaktion individueller und situativer Variablen. Vor diesem Hintergrund haben wir eine längsschnittlich angelegte Studie durchgeführt, um herauszufinden, ob individuelle Muster der Lernstrategienutzung identifiziert werden können und wie sich diese Muster im Verlauf des ersten Studienjahres verändern.
Methoden: Studierende der Medizin (N=175; 58% weiblich) wurden innerhalb des ersten Studienjahrs dreimal zu ihren Lernstrategien befragt. Um Gruppen von Studierenden mit unterschiedlichen Lernstrategiemustern zu identifizieren, wurden hierarchische Clusteranalysen (Ward) durchgeführt.
Ergebnisse: Es konnten vier verschiedene Lernstrategiemuster bei den Studierenden des ersten Semesters der Humanmedizin identifiziert werden (die „unbekümmerten“, die „flexiblen“, die „problematischen“ und die „fleißigen“ Lerner). Im Vergleich zu ihren Mitstudierenden hatten die problematischen Lerner die schlechtesten Abiturnoten. Weiterhin konnten vor allem im ersten Semester Veränderungen in der Anwendung von Lernstrategien festgestellt werden.
Schlussfolgerung: Zu Beginn ihres Studiums setzten Studierende unterschiedliche Muster von Lernstrategien ein; die Ausprägung dieser Muster verändern sich während des ersten Studienjahres. Weitere Studien sind notwendig, um besser zu verstehen, wie individuelle und situative Faktoren, studentisches Lernen beeinflussen.
Introduction
Inquiries into medical students’ learning are important for a number of reasons. First of all, the competence and willingness to learn in an efficient and effective way is increasingly regarded not just as a prerequisite for medical education, but also as an important outcome given the rapid change and growth of knowledge that is relevant for medical practice [1]. Secondly, medical education is and has always been an endeavour where a huge body of knowledge has to be mastered and the question, how this is done best, is probably as old as medical education itself [2]. With regard to medical practice it is especially important that students avoid to accumulate “inert knowledge”, knowledge that is readily available for reproduction during an exam, but cannot be used for solving problems [3], [4]. A deeper understanding of this conflict between learning for school and learning for life emerged with the research tradition of students’ approaches to learning (SAL). By observing how students approached a given learning task two fundamentally different orientations could be distinguished: Deep learning, i.e. aiming at understanding the significance and meaning of the learning material, and superficial learning, i.e. aiming at just memorizing the facts. Building on initial qualitative studies several inventories have been developed to measure students’ learning approaches adding further validity evidence in favour of these constructs and elaborating them. The most important extension of the twofold model has certainly been the description of a strategic or achievement orientation in student learning, characterized by aiming at academic achievement (i.e. high grades) in the first place [5]. The deep/surface classification is also supported by studies from another research tradition investigating students learning strategies. Based on evidence from cognitive psychology this conception understands learning as a complex process requiring a number of intentional activities embracing cognitive processes (dealing with the learning material), managing and regulating internal and external resources (e.g. time management, creating a conducive learning environment), emotional and motivational processes (e.g. dealing with potential distraction or frustration) and meta-cognition (i.e. supervising the learning process as a whole) [6].
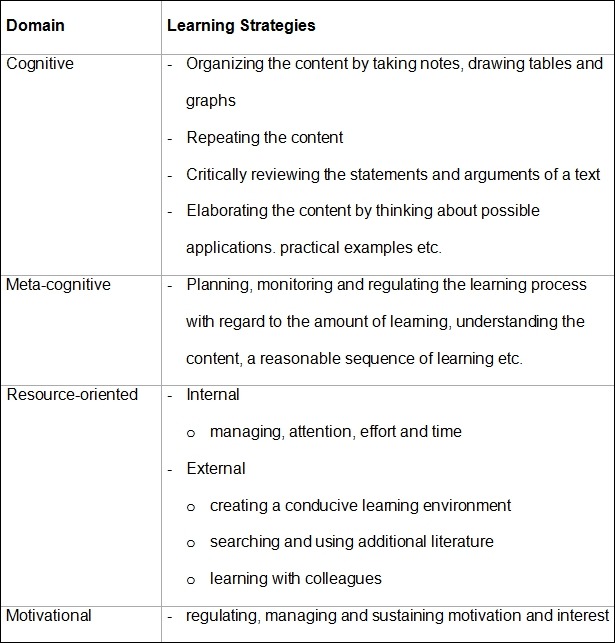
A number of instruments have been developed to measure learning strategies [7], [8], [9], and despite some conceptual differences they all embrace comparable domains (see Table 1 (Tab. 1)). Data obtained with these inventories are usually analysed by means of multivariate statistical methods like factor analysis resulting in factors that basically resemble the deep/surface (or meaning/reproduction) classification found in the SAL tradition [10]. In contrast, studies analyzing which learning strategies students really use by means of cluster analyses are conducted less frequently. Such approaches might reveal “dissonant” patterns in the “orchestration” of learning strategies that are much less intuitive than the deep/surface/achieving approaches [11], [12], [13].
Table 1. Domains of Learning Strategies [8].
Against this background, one of the most pressing questions is why and when students exhibit a deep, a surface, or a strategic approach respectively or – more generally – what influences how students learn. Evidence from a number of studies points to the impact of the learning environment (e.g. instructional methodology, assessment formats, educational philosophy, teacher behaviour) as one of the most important determinants of students’ learning [5], [14], [15]. With regard to medical education the comparison of traditional and problem-based learning (PBL) curricula indicated for instance that students did learn differently within the respective programs and that PBL-students exhibited more self-regulated learning than their peers in the traditional curriculum [16], [17], [18]. Differences were also found when medical students were compared to psychology students, indicating that the latter were more oriented towards understanding, while the medical students were more oriented towards reproduction [19].
With regard to the context sensitivity of learning approaches and the notion that learning is more and more regarded as a lifelong process [20], [21], it is necessary to understand the dynamics and development of learning in the course of time. Thus, longitudinal studies investigating students’ use of learning strategies are necessary, but are relatively rare and yielded ambiguous results hitherto [22]. Some studies confirmed what one might expect or at least hope for, i.e. that students make more use of deep learning strategies and consolidate a meaning orientation in their learning as they progress through their studies [23], [24]. In a longitudinal study comparing a traditional with a PBL-curriculum in medical education, students in the PBL track adopted more deep learning strategies than their colleagues. In addition, students who changed to the PBL track after one year improved their deep learning strategies [25]. However, there is also evidence that the reverse might be true, namely that the longer they study the more students develop a superficial, reproduction oriented learning approach [5]. This is also true with regard to medical education, even within a PBL curriculum [26].
Overall, understanding better how students learn and how the learning environment influences the way students approach learning will allow medical teachers to optimise the learning environment i.e. the curriculum, instructional methods, assessments, etc. [27], [28], [29].
Research questions
Against this background we conducted a longitudinal study to investigate the use of learning strategies of medical students in their first academic year. We thought that the transition from school into medical education is especially important with regard to the use of learning strategies as students have to adapt to a new learning environment and establish effective study habits in a relatively short time. Thus, we came up with the following research questions:
Can we identify different patterns in the use of learning strategies in novice medical students? If so, are these different learning patterns associated with different learning outcomes?
Can we identify an impact of the new learning environment on the use of learning strategies in following students through the course of their first academic year?
Method
Learning environment
This study was carried out at Freiburg University Medical School. Although the term “learning environment” is often used quite comprehensively to denote social, physical, psychological, and pedagogical variables of a specific situation or institution we focus here on the curricular aspects (although the other variables might influence student learning as well). The curriculum of this institution is rather “traditional” with regard to structure and content. Two preclinical years (mainly basic science teaching) are followed by a first national exam and four years of clinical training with the concluding second national exam. The curriculum is largely discipline-based and, with regard to methods, rather teacher-centred.
Participants
Medical students from Freiburg, Germany, were surveyed on three occasions during their first academic year in 2007 and 2008. We asked them to fill out a questionnaire in the first week of their study (T1), at the end of the first half year (T2) and at the end of the first year (T3).
Instruments
Learning Strategies
To measure the use of learning strategies, we used the LIST-questionnaire (Inventar zur Erfassung von Lernstrategien im Studium) [30], because this instrument is a slightly modified German translation of the Motivated Strategies for Learning Questionnaire (MSLQ) by Garcia and Pintrich [8]. The LIST has been used in a number of studies with university students; its factor structure was reliably reproduced [30]. It consists of 77 items that are to be rated on a 5-point-Likert-type scale ranging from 1 (very rarely) to 5 (very frequently). These items were classified into eleven scales with four to eleven items each.
Learning outcomes
In order to find out whether students with different learning strategy patterns differed in their achievements, we obtained their final school grades and their results in the regular end of term test in medical psychology. This test included six open-ended questions and 39 questions with right-wrong-don’t-know-format. We rotated these questions in a randomly determined order to prevent students copying the answers from their fellow students.
Data Analysis
We conducted a hierarchical cluster analysis (Ward) with the ratings of the T1-learning strategies in order to identify groups of students with different patterns of learning strategies. Analyses of variance (ANOVA) were computed and the results of the Scheffé post hoc tests were used in order to capture the defining characteristics of the clusters. Furthermore we conducted a MANOVA and paired t-tests in order to determine whether the use of learning strategies changes over time. All analyses were performed using SPSS for Windows version 17.0.
Results
A total of 175 students answered the questionnaire on all three occasions, 58% were females. The average age was 20.8 years (SD 2.5).
Cronbach’s Alpha for the LIST-scales and this sample ranged from 0.59~0.91. The scales are grouped into the following four categories: cognitive learning strategies: organization (CR-α=.83), repetition (CR-α=.75), elaboration (CR-α=.80), critical review (CR-α=.86). Meta-cognitive learning strategies: (CR-α=.59). Resource-oriented strategies (internal): effort (CR-α=.77), distractibility1 (CR-α=.91), time management (CR-α=.82). Resource-oriented strategies (external): learning with colleagues (CR-α=.85), learning environment (CR-α=.75), literature (CR-α=.72).
Cronbach’s Alpha for the open-ended questions was CR-α=.84). The right-wrong-don’t-know-format-questions versions were reliable (CR-α1=.61, CR-α2=.64, CR-α3=.66, CR-α4=.78).
Research Question 1:
Can we identify different patterns in the use of learning strategies in novice medical students?
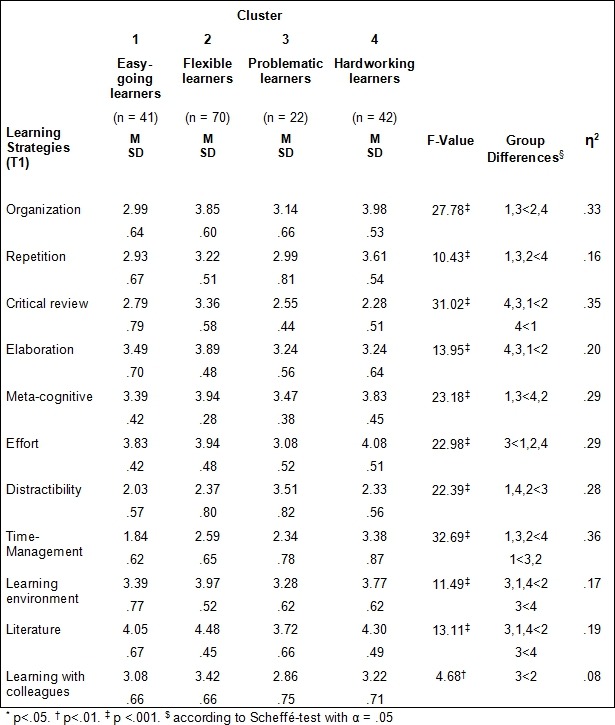
Based on the results of the cluster analyses (the decision was aided by dendrogram) the four cluster solution was most appropriate. Profiles of these clusters are shown in Table 2 (Tab. 2). The clusters may be described as follows:
Table 2. Analyses of variance for learning strategies at T1 by cluster membership.
Cluster 1 (easy-going learners)
We named the students (n=41) in this cluster easy-going-learners, because their score in distractibility is low. Compared to their peers in all other clusters they also had the lowest scores in time management strategies (i.e. they make less use of these strategies). Furthermore they made less use of the cognitive learning strategy organization compared to their peers in cluster 2 and cluster 4, and compared to students in cluster 4 they had lower scores in repetition.
Cluster 2 (flexible learners)
We characterized the students (n=70) in the second cluster as flexible learners because they made frequent use of various learning strategies, indicating a high degree of flexibility with regard to learning (see Table 2 (Tab. 2)). Compared to their peers they had the highest scores on critical review and elaboration which are important deep level learning strategies. They also had the highest scores on external resource-oriented learning strategies.
Cluster 3 (problematic learners)
The students (n=22) in the third cluster were characterized as problematic learners. Interestingly, these students showed a similar pattern as the easy-going learners with regard to the use of cognitive and meta-cognitive learning strategies (see Table 2 (Tab. 2)). However, they had the highest scores on distractibility (i.e. they are easily distracted while learning) and the lowest scores on effort. With regard to external resource-oriented strategies they had a less organized learning environment, they made less use of additional literature and learned less with their colleagues.
Cluster 4 (hardworking learners)
We named the students (n=42) in the fourth cluster the hardworking learners, because these students had the highest scores on time management (an internal resource-oriented strategy). They also had very high scores on organization and repetition. On the other hand, their low scores on critical review might indicate, that they did not go very much into depth with what they learn.
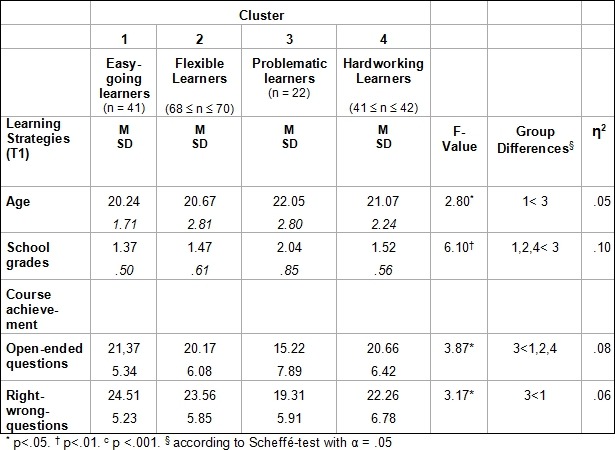
The clusters did not differ in regard to gender (χ2=6.43, df=3, n.s.), but we found a significant effect for age (F(3,170)=2.80, p<.05): Post hoc tests showed that students in the easy-going group were significantly younger than students in the problematic group (see Table 3 (Tab. 3)).
Table 3. Analyses of variance for age, final school grades and course achievement by cluster membership.
Are these different learning patterns associated with different learning outcomes?
Compared to their peers, the problematic learners had the worst final school grades and their course achievement was not as good as the achievement of their peers (see Table 3 (Tab. 3)).
Research Question 2:
Does medical education have an impact on how students learn?
To answer our second research question we looked for changes in the use of learning strategies over the course of time. In a first step we analysed the data of the whole cohort (see Table 4 (Tab. 4)), in a second step we further analysed the data of each cluster individually. Eight significant time effects for learning strategies were identified (see Table 4 (Tab. 4)). Additional analyses (paired t-tests) showed that the majority of changes took place between T1 and T2 (i.e. students’ first term tOrg(167)=3.85, p<.001, tCritR(170)=3.32, p<.01, tMetaC(169)=4.94, p<.001, tEffort(172)=5.26, p<.001, tDistract=-2.40, p<.05, tTimeM(173)=-4.53, p<.001, tLit (173)=9.34, p<.001, tLCol(172)=2.38, p<.05). The largest effect for time was found for the use of additional literature (η2part=.37). The means for distractibility (having difficulties with keeping track of the learning task at hand) and for using of time management strategies increased, while the use of the other strategies which are subject to change decreased. Further decreases occured between T2 and T3 namely with regard to critical review (tCritR(164)=4.83, p<.001), use of additional literature (tLit(172)=2.01, p<.001) and learning with colleagues (tLCol(171)=2.47, p<.05).
Table 4. Repeated measures analyses of variance for learning strategies by cluster membership (CL) and time of assessment (T, T1=first week of study, T2=end of the first half year, T3=end of the first year).
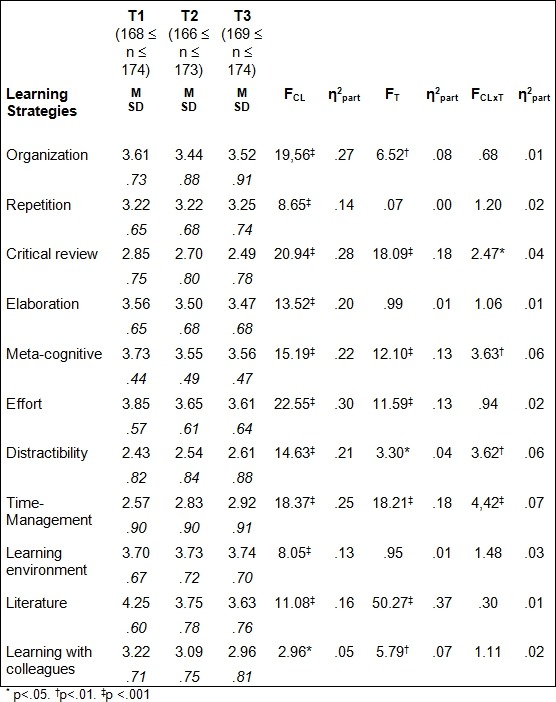
Four significant effects for the interaction between time and cluster membership were detected (see Table 4 (Tab. 4)). Further analyses showed that there was a decrease in the use of critical thinking in the clusters flexible learners (MT1=3.35, MT2=3.01, MT3=2.78), problematic learners (MT1=2.54, MT2=2.52, MT3=2.32), and hardworking learners (MT1=2.26, MT2=2.11, MT3=1.97) and a decrease of meta-cognitive learning strategies in the clusters flexible learners (MT1=3.95, MT2=3.74, MT3=3.69) and hardworking learners (MT1=3.83, MT2=3.63, MT3=3.55). Increases in distractability were found for easy-going learners (MT1=2.03, MT2=2.40, MT3=2.37), flexible learners (MT1=2.37, MT2=2.39, MT3=2.56) and hardworking learners (MT1=2.33, MT2=2.40, MT3=2.59). Finally increases in time management strategies were found for easy-going learners (MT1=1.82, MT2=2.45, MT3=2.62), flexible learners (MT1=2.59, MT2=2.74, MT3=2.85) and problematic learners (MT1=2.34, MT2=2.60, MT3=2.89).
Discussion
With regard to our first research question we identified four different patterns in the approaches to learning among novice medical students. As these patterns were identified at the very beginning of students’ first academic year, they most likely reflect individual preferences in learning that have been established during the individual learning history hitherto. The largest group of students, the flexible learners, seem to be very well prepared for the demands of medical education: They use a variety of learning strategies, they are deep level learners and they are rewarded by good results. These are certainly the students we all think of when we imagine an ideal student.
With regard to achievement the easy-going learners also seem to get along quite well. However, their approach to learning is not as favourable as their course achievement suggests. Although they seem to win hands down they might run into difficulties as more challenging and demanding learning tasks come up. Then they might need just those learning strategies they use less and that would qualify them to master huge amounts of content (i.e. time management), to understand complex material (i.e. organization) and to build up a knowledge base (i.e. repetition).
In contrast, the hardworking learners approach their learning in a very organized fashion not only with regard to time management, but also with regard to learning material. However, these students seem to regard learning very much as a means to an end (i.e. becoming a physician) and not as an end in itself, as may be concluded from their low score on critical review (an important deep level learning strategy). These students might also get along quite well particularly with regard to the current demands of examinations, because written tests focussing on reproductive knowledge are still very common in German medical education. However, with regard to lifelong learning and the importance of critical thinking skills in physicians’ day-by-day practice one would wish that these students broaden their repertoire of learning strategies towards deeper and more thorough learning. An appropriate reward structure (i.e. exams that require deep level learning) would certainly help in this regard.
Finally, the problematic learners are certainly the group that needs the most attention of all the clusters identified. These students do not only show an unfavourable pattern of learning strategies, but they also bring up the rear in terms of course achievement. However, given the relatively poor school grades of theses students one might conclude that at least some of their learning problems existed prior to medical school.
With regard to our second research question we identified changes in the use of learning strategies. Some affected all students, some were specific for one or more of the clusters. Overall we were not surprised to see most of the changes happen during the first term. When students completed the survey for the first time they had no experience whatsoever with their new learning environment at medical school and could only base their answers on their prior learning experiences and their presumptions (or their ideal) about how they will learn in medical education. Given that, we consider the changes during the second term as more important, as they more specifically reflect students’ adaption to medical school: a decrease in critical review, use of additional literature and learning with colleagues. We witnessed the most prominent decline of all learning strategies in the use of additional literature as this is true for all participants in our study. Further changes refer to learning with colleagues. A decrease in the use of this learning strategy is clearly undesirable as learning with colleagues not only contributes to deep learning, but also to other important educational goals of medical education: Individual conceptual assumptions can be challenged and corrected more easily [31], [32], the individual ability to argue and explain can be trained as well as interpersonal skills that are important prerequisites with regard to team communication. Furthermore, learning with peers might also contribute to the socialisation process into the medical profession. However, as some effort in terms of organization and time is needed, learning with colleagues might also suffer from time constraints caused by a high study load.
Even more worrisome is the fact that the use of critical review, an important deep level learning strategy declines in three clusters (with exception of the easy-going learners). This decline is most prominent in the group of the flexible learners. As they have the relatively highest score at T1 one might suspect a regression to the mean here [33], but the decline continues to almost the same extent throughout the second term suggesting that it rather reflects students’ experiences with the learning environment. Obviously, they are not encouraged to cultivate their tendency to get to the bottom of things. With regard to the problematic and the hardworking learners this is just as unsettling as it further enhances the unfavourable tendencies that are already inherent in their pattern of learning strategies at the very beginning of their studies.
Further significant effects of interaction between time and cluster membership allocation refer to meta- cognitive strategies, distractability and time management. Although the decline in the use of meta-cognitive strategies identified in three clusters (with the exception of the easy going learners) could only be identified between T1 and T2 and must therefore be interpreted with great care, it is nevertheless important, as these strategies are considered as the core of self-regulated learning [34]. These strategies are used to plan, monitor and supervise one’s own learning and are thought to be directly related to the quality of the learning process in terms of effectiveness and sustainability [35]. Again, high workload and time constraints might discourage the use of these strategies even if their use is specifically encouraged [26].
The mean values for distractibility (having difficulties with keeping track of the learning tasks at hand) increase in three of the four clusters. The problematic learners already have the highest scores and remain on a relatively high level. The increase in distractibility might be caused by the high amount of new material to be learned by the students as this might lead to a cognitive overload resulting in more attentional difficulties [36].
Since the use of time management strategies increases in three of the four clusters (the hardworking learners already had the relatively highest score on that strategy in T1, thus, a ceiling effect might explain the absence of an increase here) one might conclude that both changes are due to the high study load in the first academic year. This might prompt students to restrict their learning to the bare necessities, i.e. what is indispensable to pass the exams. Thus, instead of looking for additional sources of knowledge, comparing, contrasting and critically evaluating what they have found, they might just learn with the handouts provided by their teachers or read just the one book which promises to provide the best preparation for the upcoming tests.
Limitations
Some limitations apply our study. The first limitation to be mentioned is the drop out rate over the observation period. Although we started with the complete cohort of roughly 300 students, we ended up with a sample of around 175 individuals. This is mainly due to organisational reasons as it became increasingly difficult during the course of our study to reach all students at the same time. As we used a longitudinal within subject design we had a coding system to warrant individual anonymity and we lost a few individuals due to coding inconsistencies. Furthermore our survey was quite comprehensive in terms of the sheer quantity of items therefore we had a number of missing data for some aspects and we decided to only include complete data sets in our analyses. Nevertheless, our sample is not biased with regard to age, gender, school grades, tests result and can be regarded as representative for our basic population.
This study was carried out at only one institution making it prone to local biases e.g. through the admission process and specifics of the curriculum. Admission at this institution is mainly based on final school grades the most typical admission criteria for medical education in Germany. With regard to the curriculum it would be interesting to repeat the study at an institution with a more learner-centred curriculum to compare the results.
A further limitation applies to the measurement of course achievement as that was based on only one test in medical psychology. The reason is that this is the only test within the first year using a grading system, all other tests resulted in just pass/fail decisions only.
Finally, we only followed students through their first academic year. Although we regard this as a critical period particularly with regard to the adaptation to the new learning environment, it is still a very short period given the duration of overall medical education (six years in Germany) and life long learning. Thus, further changes might occur in the approaches to learning especially with the transition into clinical training.
Conclusions
Despite these limitations we think that there is a number of lessons to be learned from our study. The results add up to a complex picture of students’ learning. Students are by no means a homogenous group, but approach their learning tasks with different strategies. Furthermore, how students learn does not solely depend on their individual preferences, aptitudes or skills, but is influenced by the learning environment (e.g. “assessment drives learning”). The results of our study help to better understand in which way learning is affected by external factors. Overall our results indicate that the learning environment in the first academic year of medical school yields unwanted results as students change their learning strategies to more superficial learning, with less awareness and more constraint than would be desirable (and imagined by themselves beforehand). Pre-existing unfavourable tendencies in learning are rather enhanced than diminished while beneficial approaches are rather discouraged than fostered. We think that the concept of learning strategies we used here is especially helpful in analysing very specifically how the different components of the learning environment (e.g. teaching formats, work load, test formats, student support) might contribute to that development, i.e. how they influence the use of learning strategies in our students. Furthermore, we think that the results of our study are helpful to anticipate and understand what kinds of challenges and difficulties students might face while they grow into medical education. Another important lesson of our study is the fact that not only those students whose difficulties are more obvious (i.e. the problematic learners) need attention, but also those who at a first sight seem to get along quite well in terms of course achievement, as the latter might mask insufficiencies in the learning approaches.
Taken together we think that our study contributes another puzzle piece to the bigger picture of medical students’ learning that enables us as medical teachers to better tailor our initiatives, interventions and support to students’ needs.
Notes
1 In the original version of the LIST this scale is named “attention.” However, since all its items refer to attentional problems high values rather indicate attentional deficits. Thus, we renamed the scale to “distraction“.
Competing interests
The authors declare that they have no competing interests.
References
- 1.General Medical Council. Tomorrows Doctors: Recommendations on Undergraduate Medical Education. London: GMC; 2002. [Google Scholar]
- 2.Billroth T. Aphorismen zum "Lehren und Lernen der medicinischen Wissenschaften". Wien: C Gerold’s Sohn; 1886. [Google Scholar]
- 3.Whitehead AN. The Aims of Education and Other Essays. New York: Macmillan; 1929. [Google Scholar]
- 4.Renkl A, Mandl H, Gruber H. Inert knowledge: Analyses and remedies. Educ Psychol. 1996;31:115–121. doi: 10.1207/s15326985ep3102_3. Available from: http://dx.doi.org/10.1207/s15326985ep3102_3. [DOI] [Google Scholar]
- 5.Entwistle N, Ramsden P. Understanding student learning. London: Groom Helm; 1983. [Google Scholar]
- 6.Weinstein CE, Mayer RE. The teaching of learning strategies. In: Wittrock MC, editor. Handbook of Research on Teaching. New York: MacMillan; 1986. pp. 315–327. [Google Scholar]
- 7.Vermunt JD, Vermetten YJ. Patterns in student learning: Relationships between learning strategies, conceptions of learning and learning orientations. Educ Psychol Rev. 2004;16(4):359–384. [Google Scholar]
- 8.Garcia T, Pintrich P. Assessing students' motivation and learning strategies in the classroom context: The Motivated Strategies for Learning Questionnaire. In: Birenbaum M, Dochy FJ, editors. Alternatives in assessment of achievements, learning processes and prior knowledge. New York, NY: Kluwer Academic/Plenum Publishers; 1996. pp. 313–339. Available from: http://dx.doi.org/10.1007/978-94-011-0657-3_12. [DOI] [Google Scholar]
- 9.Weinstein C, Zimmermann S, Palmer D. Assessing learning strategies: The design and development of the LASSI. In: Weinstein CE, Goetz ET, Alexander PA, editors. Learning and study strategies: Issues in assessment, instruction, and evaluation. San Diego, CA: Academic Press; 1988. pp. 25–40. [Google Scholar]
- 10.Lonka K, Olkinuora E, Mäkinen J. Aspects and Prospects of Measuring Studying and Learning in Higher Education. Educ Psychol Rev. 2004;16:301–323. [Google Scholar]
- 11.Long WF. Dissonance detected by cluster analysis of responses tot he approaches and study skills inventory for students. Stud High Educ. 2003;28:21–35. doi: 10.1080/03075070309303. Available from: http://dx.doi.org/10.1080/03075070309303. [DOI] [Google Scholar]
- 12.Lindblom-Ylänne S, Lonka K. Dissonant study orchestrations of high achieving university students. Europ J Educ. 2000;15:19–32. [Google Scholar]
- 13.Meyer JH. Study Orchestration: The manifestation, interpretation and consequences of contextualized approaches to studying. High Educ. 1991;22:297–316. doi: 10.1007/BF00132293. Available from: http://dx.doi.org/10.1007/BF00132293. [DOI] [Google Scholar]
- 14.Wierstra R, Kanselaar G, Van Der Linden J, Lodewijks H, Vermunt JD. The impact of the university context on European students’ learning approaches and learning environment preferences. High Educ. 2003;45:503–523. doi: 10.1023/A:1023981025796. Available from: http://dx.doi.org/10.1023/A:1023981025796. [DOI] [Google Scholar]
- 15.Trigwell K, Prosser M. Relating approaches to study and quality of learning outcomes at the course level. Br J Educ Psychol. 1991;61:265–275. doi: 10.1111/j.2044-8279.1991.tb00984.x. Available from: http://dx.doi.org/10.1111/j.2044-8279.1991.tb00984.x. [DOI] [Google Scholar]
- 16.Hoofgaard Lycke K, Grottum P, Stromso HI. Student learning strategies, metal models and learning outcomes in problem-based and traditional curricula in medicine. Med Teach. 2006;28(8):717–722. doi: 10.1080/01421590601105645. Available from: http://dx.doi.org/10.1080/01421590601105645. [DOI] [PubMed] [Google Scholar]
- 17.Newble D, Hejka E. Approaches to learning of medical students and practising physicians: Some empirical evidence and its implications for medical education. Educ Psychol. 1991;11:333–342. doi: 10.1080/0144341910110309. Available from: http://dx.doi.org/10.1080/0144341910110309. [DOI] [Google Scholar]
- 18.Newble D, Clarke R. The approaches to learning of students in a traditional and in an innovative problem-based medical school. Med Educ. 1986;20(4):267–273. doi: 10.1111/j.1365-2923.1986.tb01365.x. Available from: http://dx.doi.org/10.1111/j.1365-2923.1986.tb01365.x. [DOI] [PubMed] [Google Scholar]
- 19.Lonka K, Lindblom-Ylänne S. Epistemologies, conceptions of learning, and study practices in medicine and psychology. High Educ. 1996;31:5–24. doi: 10.1007/BF00129105. Available from: http://dx.doi.org/10.1007/BF00129105. [DOI] [Google Scholar]
- 20.Albanese MA. Crafting the reflective lifelong learner: why, what and how. Med Educ. 2006;40(4):288–290. doi: 10.1111/j.1365-2929.2006.02470.x. Available from: http://dx.doi.org/10.1111/j.1365-2929.2006.02470.x. [DOI] [PubMed] [Google Scholar]
- 21.Mann KV. Educating medical students: Lessons from research in continuing education. Acad Med. 1994;69(1):41–47. doi: 10.1097/00001888-199401000-00013. Available from: http://dx.doi.org/10.1097/00001888-199401000-00013. [DOI] [PubMed] [Google Scholar]
- 22.Severiens S, ten Dam G, van Hout Wolters B. Stability of processing and regulation strategies: Two longitudinal studies on student learning. High Educ. 2001;42:437–453. doi: 10.1023/A:1012227619770. Available from: http://dx.doi.org/10.1023/A:1012227619770. [DOI] [Google Scholar]
- 23.Donche V, Coertjens L, Van Petegem P. Learning pattern development throughout higher education: A longitudinal study. Learn Individual Diff. 2010;20:256–259. doi: 10.1016/j.lindif.2010.02.002. Available from: http://dx.doi.org/10.1016/j.lindif.2010.02.002. [DOI] [Google Scholar]
- 24.Vermetten YJ, Vermunt JD, Lodewijks HG. A longitudinal perspective on learning strategies in higher education – different view points towards development. Br J Educ Psychol. 1999;69(2):221–242. doi: 10.1348/000709999157699. Available from: http://dx.doi.org/10.1348/000709999157699. [DOI] [Google Scholar]
- 25.Vu N, Van Der Vleuten C, Lacombe G. Medical students' learning processes: A comparative and longitudinal study. Acad Med. 1998;73(Suppl 10):S25–S27. doi: 10.1097/00001888-199810000-00035. Available from: http://dx.doi.org/10.1097/00001888-199810000-00035. [DOI] [PubMed] [Google Scholar]
- 26.Papinczak T, Young L, Groves M, Haynes M. Effects of a metacognitive intervention on students' approaches to learning and self-efficacy in a first year medical course. Adv Health Sci Educ. 2008;13(2):213–232. doi: 10.1007/s10459-006-9036-0. Available from: http://dx.doi.org/10.1007/s10459-006-9036-0. [DOI] [PubMed] [Google Scholar]
- 27.Vermunt J. The power of teaching-learning environments to influence student learning. In: Entwistle N, Tomlinson P, editors. Student learning and university teaching. Leicester: British Psychological Society; 2007. pp. 73–90. [Google Scholar]
- 28.Entwistle N. Understanding academic performance at university: A research retrospective. In: Shorrocks-Taylor D, editor. Directions in educational psychology. Philadelphia, PA: Whurr Publishers; 1998. pp. 106–127. [Google Scholar]
- 29.Newble D, Entwistle N. Learning styles and approaches: Implications for medical education. Med Educ. 1986;20(3):162–178. doi: 10.1111/j.1365-2923.1986.tb01163.x. Available from: http://dx.doi.org/10.1111/j.1365-2923.1986.tb01163.x. [DOI] [PubMed] [Google Scholar]
- 30.Wild KP, Schiefele U. Lernstrategien im Studium: Ergebnisse zur >Faktorenstruktur und Reliabilität eines neuen Fragebogens. Z Different Diagnost Psychol. 1994;15:185–200. [Google Scholar]
- 31.Roschelle J. Learning by collaborating: Convergent conceptual change. J Learn Sci. 1992;2:235–276. doi: 10.1207/s15327809jls0203_1. Available from: http://dx.doi.org/10.1207/s15327809jls0203_1. [DOI] [Google Scholar]
- 32.Webb NM. Peer interaction and learning in small groups. Int J Educ Res. 1989;13:21–39. doi: 10.1016/0883-0355(89)90014-1. Available from: http://dx.doi.org/10.1016/0883-0355(89)90014-1. [DOI] [Google Scholar]
- 33.Nesselroade J, Stigler S, Baltes P. Regression toward the mean and the study of change. Psychol Bull. 1980;88:622–637. doi: 10.1037/0033-2909.88.3.622. Available from: http://dx.doi.org/10.1037/0033-2909.88.3.622. [DOI] [Google Scholar]
- 34.Dinsmore D, Alexander P, Loughlin S. Focusing the conceptual lens on metacognition, self-regulation, and self-regulated learning. Educ Psychol Rev. 2008;20:391–409. doi: 10.1007/s10648-008-9083-6. Available from: http://dx.doi.org/10.1007/s10648-008-9083-6. [DOI] [Google Scholar]
- 35.Paris S, Winograd P. How metacognition can promote academic learning and instruction. In: Jones BF, Idol L, editors. Dimensions of thinking and cognitive instruction. Hillsdale, NJ: Lawrence Erlbaum Associates; 1990. pp. 15–51. [Google Scholar]
- 36.Sweller J, van Merrienboer JJ, Paas FG. Cognitive architecture and instructional design. Educ Psychol Rev. 1998;10:251–296. doi: 10.1023/A:1022193728205. Available from: http://dx.doi.org/10.1023/A:1022193728205. [DOI] [Google Scholar]