

Abstract
Aim. To evaluate the utility of a seizure care pathway for seizure presentations to the emergency department (ED) in order to safely avoid unnecessary admission and to provide early diagnostic and therapeutic guidance and minimize length of stay in those admitted. Methods. 3 studies were conducted, 2 baseline audits and a 12-month intervention study and prospective data was collected over a 12-month period (Nov 2008-09). Results. Use of the Pathway resulted in a reduction in the number of epilepsy related admissions from 341 in 2004 to 276 in 2009 (P = 0.0006); a reduction in the median length of stay of those admittedfrom 4-5 days in the baseline audits to 2 days in the intervention study (P ≤ 0.001); an improvement in time to diagnostic investigations such as CT brain, MRI brain and Electroencephalography (P ≤ 0.001, P ≤ 0.048, P ≤ 0.001); a reduction in readmission rates from 45.1% to 8.9% (P ≤ 0.001); and an improvement in follow-up times from a median of 16 weeks to 5 weeks (P < 0.001). From a safety perspective there were no deaths in the early discharged group after 12 months follow-up. Conclusion. The burden of seizure related admissions through the ED can be improved in a safe and effective manner by the provision of a seizure care pathway.
1. Introduction
Epilepsy is the most common serious neurological disorder of young people affecting nearly 3.4 million individuals in Europe [1]. Societal costs are considerable as individuals with medically intractable seizures make up a third of the epilepsy population [1]. More than EU15 billion is spent annually on the treatment of epilepsy in Europe, a financial burden comparable to that of lung and breast cancer combined [2, 3]. A Recent Irish prevalence study estimated that up to 40,000 children and adults in Ireland have the disorder, which gives a point prevalence of about 0.9%; in line with other industrialized nations [4]. Studies in the last decade have shown that the majority of patients with epilepsy will be urgently admitted to secondary and tertiary care institutions (mostly through the ED) at some point in the history of their illness and a significant proportion will require multiple visits [2]. Furthermore, symptomatic seizures, secondary to acute medical or surgical illness, alcohol and drug intoxication, brain trauma and stroke, add to the burden of seizure pathology in the ED. Finally, a range of mimic disorders from psychogenic nonepileptic seizures (PNES) to blackouts caused by impaired vascular responsiveness contribute to the diagnostic and therapeutic challenges.
Despite the heavy burden of seizures in the ED, international studies suggest that the majority of patients are referred unnecessarily for admission and that the acute treatment of seizures is often ineffective indicating that seizure admissions are a cause of unnecessary medical intervention, delayed diagnosis, and prolonged length of stay [5, 6].
Beginning in 2006 we first sought to determine the impact of emergency seizure admissions on the resources of a large Irish teaching hospital. On the basis of two baseline audits we identified a number of areas where we could improve the quality of service to patients with seizures by the employment of an evidence-based seizure care pathway in the emergency department (ED) and acute medical admissions unit (AMAU). This is a report of preliminary quality and safety metrics accrued by this intervention over a 12-month period (November 2008-2009).
2. Methods
The study consisted of three parts:
Retrospective audit of admissions with seizures through the emergency department in 2004.
Prospective audit of admissions with seizures through the emergency department in August 2006.
Measurement of quality and safety metrics after the implementation of an evidence-based seizure care pathway from November 2008 to November 2009.
2.1. Part 1: Retrospective Audit 2004
The first study group was restricted to in-patients discharged in 2004 with a diagnosis of a seizure or convulsion. These patients were identified through the Hospital In-Patient Enquiry (HIPE) system (a national coding system for hospital discharges in Ireland), [7] which identified 341 patients with epilepsy or seizure as the primary reason for admission. We completed detailed retrospective evaluation of the medical records of 50 randomly chosen patients. Particular attention was paid to investigations, diagnosis, specialist referral, and follow-up. The charts were also examined for what we designated as “Necessity of Admission.” An admission was deemed medically necessary if there was a history of prolonged (>5 minutes) or clustered (>2) events, a history of status epilepticus (>30 minutes of seizure activity), or an abnormal neurological exam 90 minutes after arrival to the ED. HIPE system was used to determine if any of these patients was readmitted or died over a one-year period following admission.
2.2. Part 2: Prospective Audit August 2006
The second study group represented all patients who attended the ED with an event that was deemed likely to have been a seizure or its aftermath over one calendar month in 2006. A total of 102 patients were considered eligible for inclusion. Patients who presented with a complaint of seizure, weakness, confusion, head injury, dizziness, and collapse of unknown cause were examined for possible inclusion in the study. In a similar vein to part 1 of the study, attention was paid to investigations, diagnosis, referral, and follow-up in all patients.
2.3. Part 3: Intervention Study November 2008-2009
After the baseline audits, a seizure care pathway was designed and implemented by the neurology service with the cooperation of the ED staff. The pathway required early rapid access ambulatory follow-up for patients fit for discharge from the ED. A rapid access clinic (RAC) was established and run by an existing epilepsy nurse specialist (ENS). In addition to patients discharged from wards and the ED, this clinic also reviewed new referrals from GPs and patients with an established diagnosis of epilepsy who had exacerbations of their illness, all of which were designed to avoid ED referrals. Education sessions were provided by the ENS who also provided a phone help-line and e-mail service to facilitate follow-up care. The clinic was overseen by a neurologist. Patients presenting to the ED or admitted to the AMAU overnight with seizures were seen by the seizure service fellow. Referrals were made through an Electronic Patient Record (EPR) consultation system.
Patients were managed according to a locally designed, evidence-based, Seizure Care Pathway (Figure 1). The pathway clearly laid out the criteria for:
Figure 1.
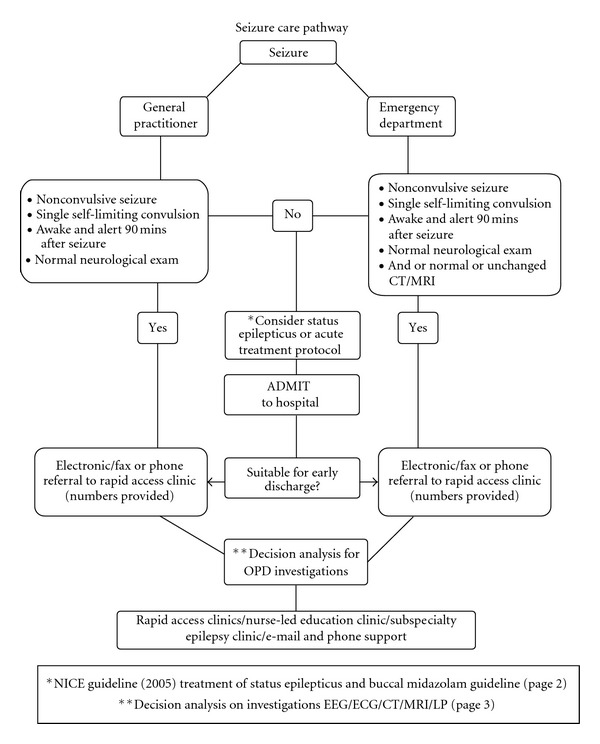
The Seizure Care Pathway used in the Intervention Study from November 2008.
Admission, discharge and follow-up.
Emergency treatment in the ED or AMAU.
A decision analysis for diagnostic tests.
Referral process for Nurse specialist education and self-management strategies.
The pathway was designed with reference to published international guidelines of care (Scottish Intercollegiate Guideline Network (SIGN) 2003 (8) and National Institute of Clinical Excellence (NICE) 2005 (9)). All patients seen by the seizure service were provided with printed cards with full details for phone and e-mail contact.
2.4. Statistical Analysis
Statistical analysis was carried out on SPSS Version 18 (SPSS Inc., Chicago, IL). Length of stay and time to CT, MRI and EEG were analysed using Kruskal Wallis test for nonparametric data. The rate of representation was analysed using Pearson Chi-square test. Times to follow-up were analysed using the Mann-Whitney U test. The reduction in admission rates was analysed using Chi-square test with Yates correction.
3. Results
3.1. Results of Part 1
During 2004, HIPE data identified 341 admissions with a specific diagnosis of epilepsy or seizure out of a total of 11,721 admissions from all causes through the ED. The median length of stay was 4 days.
In the 50 charts randomly selected out of this group, 34% of patients had a previously documented diagnosis of epilepsy at presentation. Investigations performed included CT brain (84%), MRI brain (28%), and EEG (56%). Median delay to CT, MRI, and EEG were 2 days, 5 days, and 5 days, respectively. Ambulatory follow-up was evenly divided between Neurology (28%), General Medicine (28%), and General Practitioner (20%), with a further 24% having no follow-up whatsoever. 23/50 patients (46%) represented to the emergency department with further seizures over the next 12 months.
Using our criteria for “Necessity of Admission,” we concluded that 36% could have been discharged earlier or from the ED, had appropriate investigations and neurological opinion been available in a timely manner. Of the 341 patients with a diagnosis of epilepsy, 10 died over the subsequent year but only one of those who presented with status epilepticus died as a direct result of their epilepsy.
3.2. Results of Part 2
20 (19%) of the 102 patients included in the study had a previously established diagnosis of epilepsy. 34 (33%) patients were admitted though the ED. Median length of stay of those admitted was 5 days. Of the special investigations required for epilepsy, CT Brain was the only one conducted on the day of admission and in only 5.8% of cases. Neither MRI nor EEG's were performed on any patient on the day of presentation. Ultimately of the 34 admitted, 14 (41%) had an EEG, 21 (61%) patients had a CT brain, and 4 (12%) had an MRI Brain. Median delay for EEG was 2 days; CT brain was 1 day, and MRI was 2.5 days. No data was collected on mortality or follow-up as it was designed primarily to gather data on patients presenting to the ED.
3.3. Results of Part 3
During 2009, there were 276 admissions with a primary diagnosis of epilepsy out of 12, 607 admissions from all causes through the ED. 350 patients who presented to ED between November 2008 and November 2009 with seizures and other forms of collapse were referred to the seizure team for assessment and had the seizure care pathway applied. 97 patients had an established history of either generalised or focal epilepsy and 72 patients had epilepsy associated with significant medical and surgical comorbidities. 34 patients were referred with undefined collapse, 12 patients were referred with confusion, and 4 patients with myoclonic jerks. Collapses, nonepileptic seizures and confusion accounted for 57 referrals (16.2%). Table 1 shows the complete list of admitting diagnoses.
Table 1.
List of admitting diagnosis.
| Underlying diagnosis of study cohort | Numbers |
|---|---|
| Preexisting diagnosis of primary generalised epilepsy | 37 |
| Preexisting diagnosis of localisation related epilepsy | 60 |
| Generalised status epilepticus | 7 |
| Nonepileptic seizures | 11 |
| Collapses | 34 |
| Antiepileptic medication-related toxicity | 3 |
| Significant past medical history of head injury | 6 |
| Known primary CNS tumours | 8 |
| Known CNS metastasis | 6 |
| History of stroke/TIA | 8 |
| Stroke presenting as seizures | 2 |
| Known history of learning disability | 5 |
| Dementia | 5 |
| HIV positive | 2 |
| Hepatitis B/C positive | 10 |
| Schizophrenia | 1 |
| Hyponatraemia | 11 |
| Sepsis with symptomatic seizure | 1 |
| Sepsis with rigors misidentified and referred as seizure | 3 |
| Post-operative seizures | 3 |
| Seizure after significant physical trauma | 1 |
111 (31%) patients were discharged directly from the ED. 30 (8.5%) patients stayed more than 30 days. The median length of stay was 2 days.
Of the 181 EEGs requested during the intervention study period, 99 (55%) were done on the same day. 66 (36%) were done within 1 to 3 days, and 16 (9%) were done as outpatients within 4 weeks. The median delay for EEG in the intervention study was zero days. 150 patients had CT Brain requested and 140 (93%) were performed on the same day and median delay for CT brain was again zero days. In 2008-2009, 68 (19%) of the total cohort of 350, had MR imaging of the brain requested. Same day MR brain acquisition however went up from 0% in 2004 to 7.2% in 2008-2009 and another 8.8% cases were done within 1 to 3 days. The median delay for MRI brain was 8 days in 2008-2009. Of the 57 patients with nonepileptic collapse, 12 had an EEG, 18 patients had CT brain and only one patient had an MRI brain performed.
216/350 patients (61.7%) were seen in follow-up clinics. 110 patients (31.4%) were seen in the Rapid Access Clinic (RAC). The median follow-up time to review in the RAC was 4 weeks. 64 patients (18%) were seen in the subspecialty epilepsy clinic and median follow-up time for this more stable group was 8 weeks. 18 patients (5.1%) were followed up by other services. 6 patients (1.71%) were followed up in other hospitals 31 (8.9%) of the total study group were readmitted in the 12-month follow-up period.
Of the patients seen during the study period, 19 (5.4%) patients died during the subsequent 12-month follow-up. Only 5 of those died from neurological causes. The remainder died of a combination of respiratory, cardiac, and oncological causes. The neurological causes of death were herpes encephalitis, obstructive hydrocephalus, nonconvulsive status epilepticus and subdural haematoma. Three patients died of direct seizure-related causes, two with nonconvulsive status epilepticus, and one with convulsive status epilepticus. During the intervention study period no patient who was discharged from the ED or within 2 days of admission died.
4. Comparisons of Outcomes Across All 3 Studies
4.1. Admission Rates
The number of admissions with epilepsy or seizure dropped significantly from 341 out of 11,721 (2.9%) in 2004 to 276 out of 12, 607 (2.2%) in 2009 (P = 0.0006).
4.2. Median Length of Stay
There was a significant reduction in median length of stay between the first 2 audits and the intervention study (P < 0.001). Figure 2 summarises the median length of stay over the 3 studies
Figure 2.
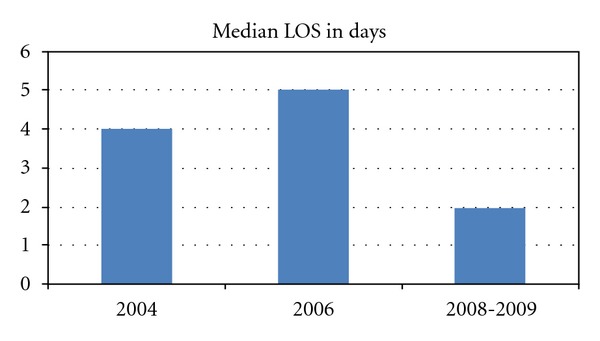
Median length of stay is shown in days for each of the study periods in Figure 2.
4.3. Time to Investigations
There was a significant improvement in time to diagnostic investigations such as CT brain, MRI brain, and electroencephalography between the first two audits and the intervention study (P ≤ 0.001, P ≤ 0.048, P ≤ 0.001). Figure 3 summarizes the median delay to investigations on admitted patients across the three studies.
Figure 3.
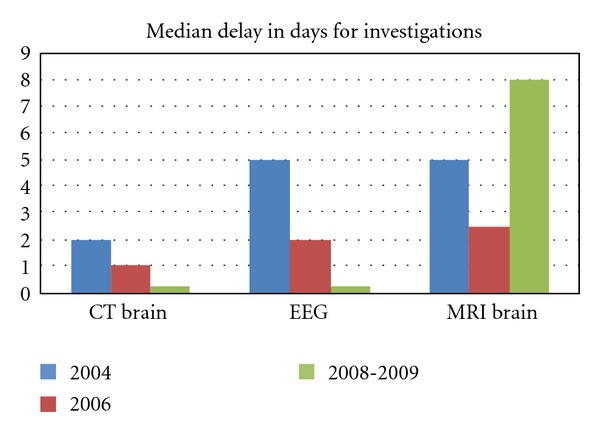
The median length of time to CT brain, EEG and MRI brain for each of the study periods.
4.4. Follow-up
There was a significant reduction in follow-up times from a median of 16 weeks to 5 weeks (P < 0.001). Figure 4 shows median times to follow-up in the baseline audit in 2004 and in the intervention study in 2008-2009.
Figure 4.
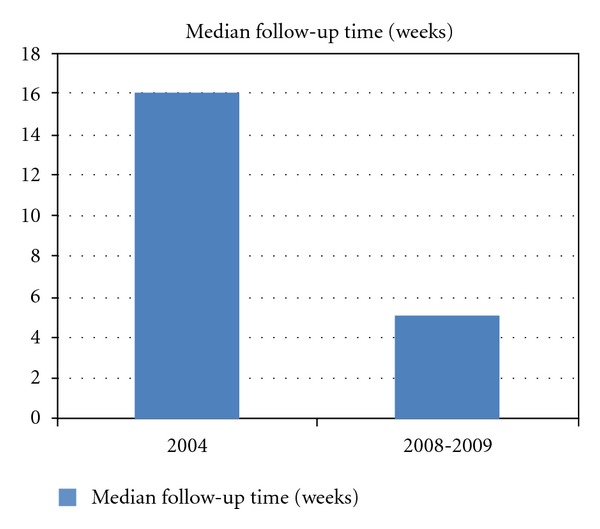
The median time to follow-up in weeks for the baseline audit in 2004 and the intervention study in 2008-2009.
4.5. Readmission
There was a significant reduction in readmission rates from 45.1% to 8.9% (P ≤ 0.001). Figure 5 shows the change in readmission rates between 2004 and the intervention study in 2008-2009
Figure 5.
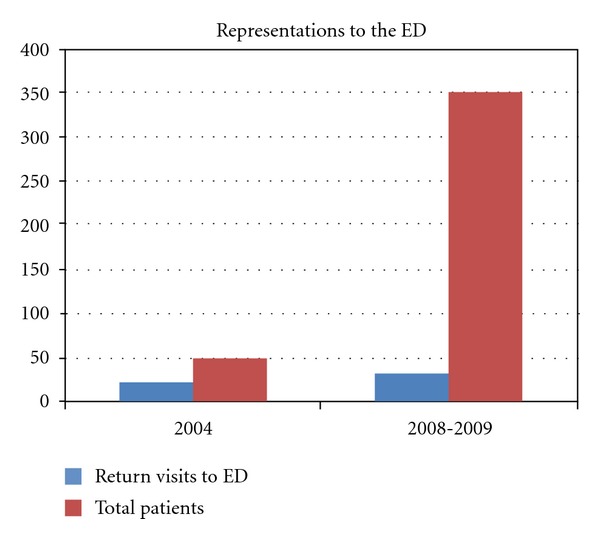
The rate of representations of patients with seizures to the Emergency Department in 2004 and during the intervention study in 2008-2009.
5. Discussion
The use of care pathways in modern healthcare delivery has been somewhat controversial since the expected gains are not always forthcoming. For instance a Cochrane review of the implementation of a care pathway in stroke rehabilitation did not endorse any benefit to patient care [8]. Nevertheless, given the highly variable care delivered in the ED in relation to seizure care, we felt that a care pathway could provide much needed improvement.
The aim of this study was to demonstrate improvements in for patients presenting to the ED with seizures and related disorders, without compromising safety by the use of an evidence-based seizure care pathway. The main quality indicators measured were requirement for admission, median length of stay, time to diagnostic tests, specialist follow-up, readmission rates, and mortality.
The main findings of the study are that through the utilization of the Seizure Care Pathway the ED and AMAU can reduce unnecessary admissions and safely discharge patients for early follow-up, which has a very significant impact on reducing representation rates. Timely decision support has the effect of significantly reducing time to diagnostic tests, particularly EEG, and thus reducing median length of stay by up to 3 days. All of these outcomes were significant statistically and support the use of care pathways for patients presenting to the ED with seizures without any increase in mortality. Below we examine each of these benefits.
5.1. Hospital Admission and Length of Stay
It has been suggested that admission of seizure patients is only warranted in patients who are at high risk of further events, remain drowsy or comatose following a period in the ED, or in whom the neurological exam reveals signs indicative of an underlying lesion or treatable infective cause. However, international studies suggest that the majority of patients are referred unnecessarily to the in-house medical or neurological services for admission [5, 6, 9, 10]. In our original retrospective audit (part 1), using a set of criteria based on the above indications for admission, we determined that 36% could have avoided admission. The intervention study showed the stability of this figure with 31% of patients actually being discharged from the ED and a further 8.5% within 24 hours of admission.
Comparison of HIPE data between 2004 with that of 2009 following implementation of the seizure care pathway shows a reduction in the number of admissions with a specific diagnosis of epilepsy from 2.9% (341) of total hospital admissions to 2.2% (276). This is despite an increase in overall admission rates from ED of 7.56% from 11,721 in 2004 to 12,607 in 2009. Had admissions continued at the rate of 2.9% with no seizure care pathway in place, it would have resulted in 365 epilepsy-related admissions in 2009, suggesting that 89 epilepsy specific admissions were avoided due to implementation of the seizure care pathway in 2008 to 2009. If we consider the median LOS to be 4 days (without the seizure care pathway being applied) this would have resulted in 356 bed days saved. Combining this figure with the 478 bed days saved by an overall median reduction in LOS of 2 days, a total of 834 is the projected bed days saved in one 12-month period as a direct result of the implementation of the seizure care pathway.
The reduction in median length of stay from 4 days in 2004 and 5 days in 2006 to 2 days during the intervention study in 2008-2009 was made possible by an emphasis upon early safe discharge in the pathway with an eye to reduce bed occupancy days. Establishment of a separate rapid access follow-up clinic made routine and even unscheduled early follow-up possible, which increased the safety and ease of early discharge. Reductions in length of stay secondary to implementation of care pathways have been reported in other areas of heath care, but not in the case of patients with seizures [11–13].
Of the discharged patients, 91.1% were not readmitted with epilepsy-related causes. The readmission rates show a significant drop from 47% to 8.9% between 2004 and 2008-2009. The reasons for such a drop are unclear. It is possible that some unobserved bias meant that patients more likely to return were seen in the 2004 audit. It may be due to a combination of more timely and effective inpatient management including the delivery of inpatient ENS education, the provision of phone and e-mail advice services, the use of rapid access to ambulatory clinics for exacerbations of existing epilepsy, and improved, timely communication with primary care teams. The reduction of median follow-up time from 16 weeks during 2004 to 5 weeks in 2008-09 may also have helped in reducing re-admissions to the ED.
5.2. Mortality
In relation to the overall safety of the seizure service with its emphasis on reducing admissions and length of stay, we found that only three of the 19 deaths in the study group were directly attributable to epilepsy. In 2004, only one death was attributable to epilepsy. While there is a slight increase in epilepsy-related deaths, there was no excess mortality in any patients discharged from the ED or within the 2-day median length of stay window.
5.3. Investigations
Accurate diagnosis and classification of seizure type are essential to the provision of quality patient care and good control. EEG is described as an important aid in the evaluation of seizure patients [14]. In relation to the baseline audit the median waiting time to EEG was 5 days, demonstrating that most patients were not being tested soon after the seizure period. Such waiting times observed in the baseline audits suggested that EEG contributed significantly to the length of stay of individual patients. During the intervention study the involvement of early specialist opinion allowed for the streamlining of those who required EEG which occurred on the day of admission in approximately 54% of the study group and in total over 90% had the test done in 3 days or less.
Neuroimaging is essential to identify structural lesions, which may result in the development of a seizure disorder. Jackson et al. [15] assert that MRI is the gold standard imaging investigation for suspected focal lesions. Despite strong consensus within the literature for performing MRI over CT especially in focal seizures [5, 15, 16] CT was the preferred modality for neuroimaging within all our study groups. This is largely to do with the ease of access to CT over MRI at our institution, which has not changed significantly since 2004. 84% of the retrospective sample had a CT performed, whilst only 28% had an MRI. In the intervention study only 42% of patients had a CT requested reflecting the fact that in a number of cases of either established epilepsy or indeed EEG proven Primary Generalized Epilepsy, the pathway was able to obviate the need for CT. An improvement in time to brain imaging was demonstrated in the intervention study with 93% of patients having their CT on the same day of request. Unusually, the mean wait time for MRI brain increased in 2009 compared to 2004. This, we believe, was due to the steadily increasing demand for MRI brain in acute presentations of seizure over those years coupled with limited availability of our MRI resource (one magnet open only during office hours). This has been ameliorated lately by the addition of a second scanner.
5.4. Review and Follow-up
As outlined by the SIGN [16] and NICE [17] guidelines, adults with epilepsy should have a specialist expert opinion in an ambulatory setting including regular structured annual review. In the retrospective 2004 audit, mean time to neurology clinic follow-up was 14 weeks and only 28% of patients were followed up by the specialty. The lack of decision support and or expert neurological opinion to two-thirds of the 2004 study group may have contributed to the longer length of stay in this group as there may have been a delay in diagnosis and pursuing appropriate investigations. Only 28% of that group were followed up by the neurology service in outpatient clinics, which we speculate may have contributed to return ED presentations and readmission rates. The intervention study suggests that the decision support embodied in the Seizure Care Pathway and early follow-up contributed significantly to a reduction in readmission rates.
6. Limitations
Retrospective chart reviews, which formed the basis of initial baseline data, are hazardous for deciding on service provision due to the unreliability and potential bias in the data. Furthermore, the initial analysis was on a relatively small number of charts. In this study we complimented the retrospective audit with a short prospective audit, which validated some of the retrospective audit and independently verified characteristics of patients admitted with epilepsy and their course in hospital. The intervention study was large enough to draw conclusions but its comparison to the two prior audits must be done with caution as the patient characteristics may have been biased in the smaller studies. This was exemplified by the significant differences in readmission rates between the two audits and the intervention study. While some of the difference were undoubtedly due to service improvements, the scale of difference suggested a possible bias in patient characteristics.
Finally, for system-wide change the decisions that contributed to the improved quality metrics would have ideally been made by ED and acute medical staff and specialist nurses applying the principles in the seizure care pathway. In this study the pathway was implemented by a specialist service and thus the generalizability of the results in unclear. However, the lack of widespread use of pathways for seizure presentations requited that a proof of principle study was required. Future study should now focus on the use of an integrated care pathway (ICP) without resource necessarily to a specialist at the ED/AMAU interface.
7. Summary and Recommendations
It appears that a large proportion of seizure-related presentations are referred to the in-house medical or neurological teams for admission, due in large part to the lack of access to appropriate algorithms for admission and decision support for early treatment and diagnostic investigation and the difficulty in obtaining outpatient investigations and specialist epilepsy follow-up in a reasonable length of time. This study conducted over a 12 month period using baseline data collected between 2004 and 2006 shows that using an evidence-based care pathway with early specialist advice and follow-up, along with directed patients education and a range of communication tools to aid in self-management such as telephone and e-mail advice, can contribute significantly to quality and value improvements in epilepsy care without compromising safety. We recommend further study of this programme and we have embedded a continuous improvement cycle into prospective audit.
References
- 1.Shorvon SD. The Treatment of Epilepsy. Oxford, UK: Blackwell; 2005. [Google Scholar]
- 2.Pugliatti M, Beghi E, Forsgren L, Ekman M, Sobocki P. Estimating the cost of epilepsy in Europe: a review with economic modeling. Epilepsia. 2007;48(12):2224–2233. doi: 10.1111/j.1528-1167.2007.01251.x. [DOI] [PubMed] [Google Scholar]
- 3.Andlin-Sobocki P, Jonsson B, Wittchen HU, Olesen J. Cost of disorders of the brain in Europe. European Journal of Neurology. 2005;12(supplement 1):1–27. doi: 10.1111/j.1468-1331.2005.01202.x. [DOI] [PubMed] [Google Scholar]
- 4.Linehan C, Kerr MP, Walsh PN, et al. Examining the prevalence of epilepsy and delivery of epilepsy care in Ireland. Epilepsia. 2010;51(5):845–852. doi: 10.1111/j.1528-1167.2009.02417.x. [DOI] [PubMed] [Google Scholar]
- 5.Dunn MJG, Breen DP, Davenport RJ, Gray AJ. Early management of adults with an uncomplicated first generalised seizure. Emergency Medicine Journal. 2005;22(4):237–242. doi: 10.1136/emj.2004.015651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Cascino GD, Hesdorffer D, Logroscino G, Allen Hauser W. Treatment of nonfebrile status epilepticus in Rochester, Minn, from 1965 through 1984. Mayo Clinic Proceedings. 2001;76(1):39–41. doi: 10.4065/76.1.39. [DOI] [PubMed] [Google Scholar]
- 7.Casemix Ireland. HIPE Coding Auditing Toolkit (HCAT) Information Leaflet. Casemix Ireland; 2007. [Google Scholar]
- 8.Kwan J, Sandercock P. In-hospital care pathways for stroke: an updated systematic review. Stroke. 2005;36(6):1348–1349. [Google Scholar]
- 9.Ryan J, Nash S, Lyndon J. Epilepsy in the accident and emergency department—developing a code of safe practice for adult patients. Emergency Medicine Journal. 1998;15(4):237–243. doi: 10.1136/emj.15.4.237. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Bhatt H, Matharu MS, Henderson K, Greenwood R. An audit of first seizures presenting to an accident and emergency department. Seizure. 2005;14(1):58–61. doi: 10.1016/j.seizure.2004.10.003. [DOI] [PubMed] [Google Scholar]
- 11.Pearson SD, Kleefield SF, Soukop JR, Cook EF, Lee TH. Critical pathways intervention to reduce length of hospital stay. American Journal of Medicine. 2001;110(3):175–180. doi: 10.1016/s0002-9343(00)00705-1. [DOI] [PubMed] [Google Scholar]
- 12.Co JP, Johnson KB, Duggan AK, Casella JF, Wilson M. Does a clinical pathway improve the quality of care for sickle cell anemia? The Joint Commission Journal on Quality and Patient Safety. 2003;29(4):181–190. doi: 10.1016/s1549-3741(03)29022-5. [DOI] [PubMed] [Google Scholar]
- 13.Dy SM, Garg P, Nyberg D, et al. Critical pathway effectiveness: assessing the impact of patient, hospital care, and pathway characteristics using qualitative comparative analysis. Health Services Research. 2005;40(2):499–516. doi: 10.1111/j.1475-6773.2005.00369.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kawkabani A, Rossetti AO, Despland PA. Survey of management of first-ever seizures in a hospital based community. Swiss Medical Weekly. 2004;134(39-40):586–592. doi: 10.4414/smw.2004.10738. [DOI] [PubMed] [Google Scholar]
- 15.Jackson N, Delanty N, Ridge CA. Imaging in patients with a first seizure. Irish Medical Journal. 2006;99(6) [PubMed] [Google Scholar]
- 16.Scottish Intercollegiate Guideline Network. Diagnosis and management of epilepsy in adults. 2003, http://www.sign.ac.uk/
- 17.National Institute for Clinical Excellence. The epilepsies: the diagnosis and management of the epilepsies in adults and children in primary and secondary care. 2005, http://www.nice.org.uk/