

Abstract
Leishmania donovani is considered the causative organism of visceral leishmaniasis (VL) and post-kala-azar dermal leishmaniasis (PKDL). Testing of 4/29 DNA samples from VL and PKDL patients as well as 2/7 field isolates showed an aberrant internal transcribed spacer 1 (ITS1) restriction fragment length polymorphism (RFLP) pattern, which upon sequencing strongly matched Leptomonas seymouri, thus confirming its presence in Indian leishmaniasis.
TEXT
Visceral leishmaniasis (VL) is a vector-borne disease caused by replication of parasites of the Leishmania donovani complex (L. donovani and L. infantum) within the macrophage-phagocytic system. In the Indian subcontinent and parts of Africa, its transmission is anthroponotic (2), with post-kala-azar dermal leishmaniasis (PKDL) being a sequel of VL, and is characterized by a macular, maculo-papular, or nodular rash (11).
Generally, in the Indian subcontinent, patients presenting with clinical features suggestive of VL/PKDL have the diagnosis confirmed by the presence of parasites in Giemsa-stained smears and/or culture positivity, serological diagnosis (enzyme-linked immunosorbent assay [ELISA] or rK39 strip test), and, rarely, by molecular approaches. The causative parasites are assumed to be L. donovani, although in recent years, studies have shown L. donovani causing cutaneous leishmaniasis in Sri Lanka (18). Additionally, a lower trypanosomatid, Leptomonas seymouri, has been detected in isolates from patients with VL, but not in clinical specimens (19).
Molecular diagnosis of leishmaniasis is often by PCR that typically targets the internal transcribed spacer 1 (ITS1), separating the genes coding for small subunit (SSU) rRNA and 5.8S rRNA (7). Additionally, isolates have been characterized by restriction fragment length polymorphism (RFLP) analysis of the ITS1 region (9) or the gene fragment encoding the 70-kDa heat shock protein (hsp70) (13), the latter being among the first kinetoplastid genes to be cloned and characterized due to their conserved nature (10). Upon routine diagnosis of patients with suspected VL or PKDL by ITS1 PCR, a different band pattern was reported that did not match the classical L. donovani WHO reference strain DD8 (MHOM/IN/1980/DD8) (7). Accordingly, this study was undertaken to study the RFLP patterns of clinical specimens sourced from patients with VL or PKDL along with archived parasite isolates from a different patient population.
The study population included 29 patients from 1 January 2010 to 31 January 2012 who were admitted to the School of Tropical Medicine, Kolkata, with clinical features of VL (n = 23) or PKDL (n = 6). Clinical materials included peripheral blood from patients with VL or lesional skin biopsy specimens from patients with PKDL after obtaining informed consent. The diagnosis of VL/PKDL was confirmed by rK39 strip test (20), ELISA for antileishmanial antibodies, and PCR of the ITS1 region of Leishmania sp (7). The study received approval from the Institutional Ethical Committee of the School of Tropical Medicine, Kolkata, India, and Institute of Postgraduate Medical Education and Research, Kolkata, India.
In addition, our study included archived Leishmania isolates (n = 7; V1 to V5, P1, and P2), obtained from patients with VL (n = 5) or PKDL (n = 2); all except V5 presented at the School of Tropical Medicine between 2006 and 2011. In patients with VL, parasites were isolated from spleen/bone marrow aspirates (7), while for PKDL, a 3-mm punch biopsy specimen from a nodule was collected in medium 199 (M199) supplemented with 20% heat-inactivated fetal calf serum (FCS), penicillin G (50 IU/ml), and streptomycin (50 μg/ml). The material was passed through a 230-μm sterile iron mesh and finally resuspended in 1.5 ml of the same medium, and after incubation at 24°C, culture growth was evident after 5 to 10 days. After transformation from amastigotes to promastigotes, they were gradually adapted into M199 supplemented with 10% FCS, penicillin G (50 IU/ml), and streptomycin (50 μg/ml) and subcultured every 2 to 3 days, the inoculum being 1 × 106/ml. When parasites reached the range of 107, they were cryopreserved (approximately 1 × 107 parasites per cryo vial) in freezing medium (M199 containing 30% FCS and 7.5% dimethyl sulfoxide [DMSO]).
All of the archived strains were typed by ELISA using species-specific L. donovani monoclonal antibody (5) and PCR-RFLP (9). For PCR, DNA following isolation from peripheral blood, skin biopsy specimens, and isolates (QIAamp DNA minikit; Qiagen, Hilden, Germany) was eluted in 200 μl elution buffer. Different parts of Leishmania were amplified, namely (i) ribosomal ITS1 (9) and (ii) hsp70 (13). Amplification reactions were performed in 25 μl of mixture (JumpStart REDTaq ReadyMix reaction mix; Sigma-Aldrich Chemicals, St. Louis, MO) in a Master cycler (Eppendorf, Hamburg, Germany). The amplified ITS1 and hsp70 regions were digested using HaeIII (Fermentas, Glen Burnie, MD); briefly, reactions were carried out using 1 U of HaeIII, 1× buffer, and 5 μl of the amplicon (approximately 100 μg of DNA) and incubated at 37°C for 3 h (for ITS1) or overnight (for hsp70). The digested product was analyzed by electrophoresis (3% agarose, 5 V/cm for 1.5 h) along with a 100-bp DNA ladder or GeneRuler low-range DNA ladder (Fermentas, Glen Burnie, MD) and visualized in a G-BOX Gel Doc system (Syngene, Cambridge, United Kingdom) using Gene Tools software (version 4.01.04).
For sequencing of archived Leishmania isolates, PCR products of the ITS1 region were purified (QIAquick gel extraction kit; Qiagen, Hilden, Germany) and then cloned into the pJET1.2 vector by blunt end ligation (CloneJET PCR cloning kit; Fermentas, Glen Burnie, MD). Recombinant plasmid DNA was used to transform Escherichia coli DH5α; eight colonies with an ITS1 insert were selected for each sample. Plasmid DNA was purified from colonies using a Qiagen plasmid minikit (Qiagen, Hilden, Germany) and sequenced (BigDye Terminator v3.1 cycle sequencing kit; Applied Biosystems, Foster City, CA) on an automated DNA sequencer (ABI Prism 3130, Foster City, CA). DNA sequence editing and analysis were performed using Seqscape V2.5 software (Applied Biosystems, Foster City, CA).
The reference sequences of the ITS1 gene from several trypanosomatid species were retrieved from GenBank and aligned with the sequence determined in this study (http://www.ncbi.nlm.nih.gov/GenBank/index.html) using ClustalW software and a phylogenetic tree constructed by the neighbor-joining method using MEGA version 5.0 (21).
Blood was sourced from patients with VL (n = 23) and lesional skin biopsy specimens from patients with PKDL (n = 6) (Table 1); 58.62% of patients hailed from Bihar, India (17/29), and among them, 11 (64.70%) were from zones with antimonial resistance (17). Of the remaining 12 patients, 11 were from West Bengal, India, and one was from Chhattisgarh, India, whose areas of antimonial resistance, if any, have not been defined.
Table 1.
Clinical features of the study population
| Feature | Result for patients with: |
|
|---|---|---|
| VL (n = 23) | PKDL (n = 6) | |
| Age (yr) | ||
| Mean ± SD | 30.7 ± 19.2 | 31.6 ± 16.6 |
| Median (range) | 25.5 (1–70) | 25 (13–57) |
| Male/female ratio | 16/7 | 5/1 |
| History of VL (%) | NAa | 83.3 |
| Interval between cure of VL and onset (yr) | ||
| Mean ± SD | NA | 7.2 ± 2.1 |
| Median (range) | NA | 6 (5.5–10) |
| Spleen size (cm) | ||
| Mean ± SD | 10.1 ± 7.9 | NA |
| Range | 3–29 | NA |
| Liver size (cm) | ||
| Mean ± SD | 4.4 ± 2.9 | NA |
| Range | 2–10 | NA |
NA, not applicable.
Analysis of the ITS1 PCR products of these 29 patients showed two distinct trends, namely (i) a single 320-bp amplicon in 86.2% (19 VL and 6 PKDL) of samples that matched the reference strain DD8 and (ii) dual bands of 320 and 418 bp in 13.8% (4 patients with VL). Examination of the RFLP pattern of the 320-bp product revealed a pattern similar to that of DD8, having 3 fragments with sizes of 191, 75, and 54 bp, defined as “pattern A.” With regard to the 4 samples having a dual band pattern, each band was gel extracted, purified, and digested separately with HaeIII; the 320-bp product had an RFLP profile similar to that of DD8 (i.e., pattern A), while the larger PCR product of 418 bp remained undigested by HaeIII and was defined as “pattern B.”
Among the seven archived isolates studied, five were obtained from bone marrow/splenic aspirates of patients with VL (V1 to V5), while two were from dermal tissue of patients with PKDL (P1 and P2). The majority of these patients (5/7, except V1 and V3) hailed from Bihar, the main zone of endemicity for VL in India; among them, two (V2 and P1) were from areas of antimonial resistance and three (V4, V5, and P2) were from an area having no antimonial resistance (17). The remaining two archived isolates (V1 and V3) were isolated from a patient each from West Bengal and Assam, respectively, whose patterns of antimonial resistance, if any, are yet to be defined.
All archived strains showed strong binding with D2, an L. donovani species-specific monoclonal antibody (12), and the absorbances obtained were comparable with that obtained with DD8 (MHOM/IN/1980/DD8), the L. donovani reference strain; accordingly, they were typed as L. donovani. To further characterize these archived isolates, we performed ITS1 RFLP and found two variations in the PCR products (Fig. 1, inset) that were verified by HaeIII digestion. RFLP data showed that pattern A was dominant, being present in 5/7 isolates (71.4%), and pattern B was present in 2 isolates (28.6%) (Fig. 1), akin to the profile obtained in clinical specimens. This lack of digestion by HaeIII has not been reported previously in leishmaniasis and suggests unusual variations in the sequence of the ITS1 region among Leishmania strains. Although some sequence variations in the ITS1 region between strains of L. donovani have been reported, (9, 16), a difference of 100 bp in the PCR product has not been reported to date.
Fig 1.
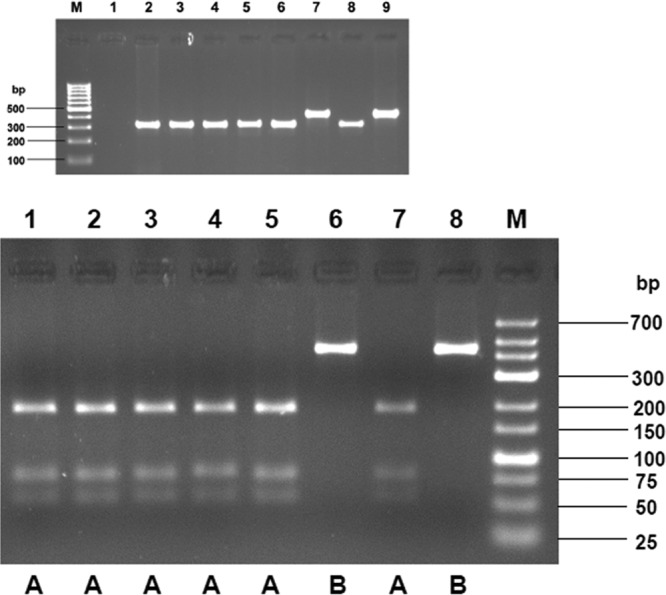
RFLP analysis of the ITS1 region amplified from Leishmania donovani isolates. Lanes: 1, DD8; 2, V1; 3, V2; 4, V3; 5, V4; 6, V5; 7, P1; 8, P2; M, low-range DNA ladder. (Inset) PCR assay of the ITS1 region from Leishmania donovani isolates. Lanes: M, 100-bp ladder; 1, PCR control (water); 2, DD8; 3, V1; 4, V2; 5, V3; 6, V4; 7, V5; 8, P1; 9, P2.
To substantiate our findings, we performed hsp70 PCR-RFLP with our archived isolates. Once again, two patterns emerged: i.e., 5 isolates matched the L. donovani reference strain, whereas 2 isolates (V5 and P2 which showed pattern B for ITS1 RFLP) showed another pattern (data not shown). The latter pattern was not comparable with any other Leishmania species (13), but it was similar to that reported in 9 Indian isolates (19). In the clinical specimens, the hsp70 PCR did not yield any product (data not shown).
In order to identify the organism from which this aberrant ITS1 gene was being amplified, the nucleotide sequence of the 418-bp fragment was determined, wherein we selected DD8 and P2 as representatives of patterns A and B, respectively; P2 was selected as it had undergone very few passages following transformation. We aligned two sequences denoting one sequence, “LdA,” for L. donovani DD8, representative of pattern A and denoting the other, “LdB,” for P2, representative of pattern B; the ClustalW alignment of the two sequences showed several mismatches and deletions (score, 73), indicating there were significant differences between them (Fig. 2A). To determine whether these sequence variants were due to Taq polymerase errors, two colonies of the variant were selected for a second round PCR using the same primers and resequenced; they were all identical to the original sequence, confirming that the observed sequence variant was not a technical error. Furthermore, two sequences were BLAST searched independently, where LdB showed a strong match with Leptomonas seymouri (accession no. EU623433.1). Based on the sequence of the ITS1 region of P2 and DD8, a neighbor-joining tree was constructed that included 33 L. donovani Indian isolates, available at National Centre for Biological Information (http://www.ncbi.nlm.nih.gov), and an extended set of organisms (Fig. 2B). The tree showed that P2 was most closely related to Leptomonas seymouri (score, 99.0) (Fig. 2B) along with 21 L. donovani Indian isolates. The remaining 12 L. donovani Indian isolates were phylogenetically closely related to DD8 (Fig. 2B) (http://www.ncbi.nlm.nih.gov/nuccore/EU364830). Additionally, sequence analysis of these 33 isolates showed that the size of the ITS1 PCR product of the 21 isolates that matched Leptomonas seymouri was 418 bp, while the size of the 12 Indian archived isolates that matched with DD8 was 320 bp. Importantly, no HaeIII restriction site was present in the 418-bp sequence, corroborating our observations (Fig. 1).
Fig 2.


Determination of the presence of Leptomonas sp. (A) Alignment of ITS1 sequences amplified from Leishmania donovani isolates representing RFLP patterns A and B. LdA, Leishmania donovani showing RFLP pattern A; LdB, isolate showing RFLP pattern B. *, matching of nucleotide; -, absence of nucleotide. (B) Neighbor-joining tree based on p-distances of the ITS1 sequences of Leishmania donovani and P2. Outgroup, Leptomonas sp. The analysis is based on an alignment of 1,234 nucleotides. Distances are measured along the horizontal branches, according to the scale shown. Bootstrap values above 70% are indicated at the internodes. *, sequence of L. donovani isolates of India collected from GenBank; •, sequence of P2.
To confirm the presence of Leptomonas seymouri in the clinical specimens, we designed a reverse primer from a 30-bp portion (nucleotide positions 197 to 227) unique to this organism. It was selected based on it being the inserted sequence present in the ITS1 region of P2 following alignment of P2 and DD8 (Fig. 2A). The forward primer (5′ CTGGATCATTTTCCGATGATACTAT 3′) was designed from the common sequence (bp 1 to 25) between P2 and DD8, while the reverse primer was 5′ TGCCCTCTCTCACACAGCA 3′; a partial ITS1 region was amplified at an annealing temperature of 60°C for 30 s. Among the archived isolates, P2 and V5, which showed pattern B gave a 210-bp product, confirming these strains were Leptomonas seymouri. We propose that after parasite transformation, Leptomonas seymouri outgrew L. donovani as Leptomonas species have been reported to grow faster than L. donovani (19). In patient DNA, 4 samples appeared coinfected with L. donovani and Leptomonas seymouri as they gave the 210-bp Leptomonas ITS1 PCR product; additionally, 2 more samples from patients with VL showed a 210-bp product (data not shown); none of the patients with PKDL showed a 210-bp band.
Based on this analysis, we conclude that clinical specimens (4/29) isolated from patients with VL/PKDL were concomitantly infected with Leptomonas seymouri as also were two archived culture isolates among seven studied; importantly, they phylogenetically clustered more closely to the monoxenous parasite Leptomonas seymouri. The occurrence of insect trypanosomatids in humans is exceptional, but reports are available that HIV-positive patients are additionally infected with nonpathogenic insect trypanosomatids (6). In Brazil, Pacheco et al. (15) described a flagellate, apparently a monoxenous trypanosomatid, in a 35-year-old HIV-positive male who presented with symptoms of VL. Hybridization analyses, against a panel of many different trypanosomatids, revealed that the unknown flagellate had kinetoplastid DNA (kDNA) cross-homology only with Leptomonas pulexsimulantis, a parasite of a dog flea (18). However, the presence of lower trypanosomatids in immunocompetent individuals is a matter of greater concern (4). Our patients had no evidence of HIV infection (testing negative for HIV), yet four of them were coinfected with Leptomonas seymouri and L. donovani. Additionally, Leishmania coinfections, including with HIV (3), Plasmodium vivax (1), or Mycobacterium tuberculosis (8), have been reported. Therefore, it may be envisaged that as VL induces a strong immunosuppression, it possibly allows nonhuman trypanosomatids to be installed in mammalian hosts.
In this study, 13.8% (4/29) patients with VL/PKDL were coinfected with Leptomonas seymouri and L. donovani. Interestingly, on analysis of the isolates reported in GenBank as L. donovani, 21/33 (i.e., 63.63%) are actually Leptomonas seymouri; in this study, 28.57% (2/7) are Leptomonas seymouri. Nasereddin et al. (14) reported about 35.59% of Indian isolates obtained from patients with VL were unidentified by reverse line blot hybridization assay using L. donovani-specific probes, but had a ITS1 sequence similarity to Leptomonas seymouri. The appearance of this opportunistic infection by Leptomonas seymouri raises questions about the clinical relevance of this pathogen. However, to date, studies pertaining to the pathobiology of these opportunistic lower trypanosomatids infecting humans have been limited.
As this study had a substantial number of patients coming from zones of antimonial resistance, it raises the possibility that Leptomonas strains are possibly less sensitive to antimony. The in vitro susceptibility toward antimony of both monoxenous trypanosomatid field isolates P2 and V5 was lower than those of the other 5 strains (M. Chatterjee, personal communication), which raises the possibility of the potential contribution of Leptomonas to the growing incidence of unresponsiveness to antimonials reported from the Indian subcontinent; however, this must be substantiated in a larger study group to conclude whether Leptomonas infections influence the epidemiology, pathology, or case management of VL. Taking these findings together, this study emphasizes the importance of estimating the extent of opportunistic pathogens in leishmaniasis.
Nucleotide sequence accession number.
The sequence determined in this study has been submitted to GenBank and is available under accession no. JN848802.
ACKNOWLEDGMENTS
DD8 and V5 were kindly provided by Lionel F. Schnur, Department of Parasitology, Hadassah Medical School, Jerusalem, Israel, and Neeloo Singh, Central Drug Research Institute, Lucknow, India, respectively.
This work received financial assistance from the Indian Council of Medical Research (ICMR), Department of Biotechnology and Department of Science & Technology, Government of India.
Footnotes
Published ahead of print 23 May 2012
REFERENCES
- 1. Ab Rahman AK, Abdullah FH. 2011. Visceral leishmaniasis (kala-azar) and malaria coinfection in an immigrant in the state of Terengganu, Malaysia: a case report. J. Microbiol. Immunol. Infect. 44:72–76 [DOI] [PubMed] [Google Scholar]
- 2. Alvar J, Canavate C, Molina R, Moreno J, Nieto J. 2004. Canine leishmaniasis. Adv. Parasitol. 57:1–88 [DOI] [PubMed] [Google Scholar]
- 3. Andreani G, Lodge R, Richard D, Tremblay MJ. 2012. Mechanisms of interaction between protozoan parasites and HIV. Curr. Opin. HIV AIDS 7:276–282 [DOI] [PubMed] [Google Scholar]
- 4. Boisseau-Garsaud AM, et al. 2000. A new case of cutaneous infection by a presumed monoxenous trypanosomatid in the island of Martinique (French West Indies). Trans. R. Soc. Trop. Med. Hyg. 94:51–52 [DOI] [PubMed] [Google Scholar]
- 5. Chatterjee M, et al. 1998. Distribution of IgG subclasses in antimonial unresponsive Indian kala-azar patients. Clin. Exp. Immunol. 114:408–413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Chicharro C, Alvar J. 2003. Lower trypanosomatids in HIV/AIDS patients. Ann. Trop. Med. Parasitol. 97:75–78 [DOI] [PubMed] [Google Scholar]
- 7. Das NK, et al. 2011. Case series of misdiagnosis with rK39 strip test in Indian leishmaniasis. Am. J. Trop. Med. Hyg. 84:688–691 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. el-Safi SH, et al. 2004. Infection rates with Leishmania donovani and Mycobacterium tuberculosis in a village in eastern Sudan. Trop. Med. Int. Health 9:1305–1311 [DOI] [PubMed] [Google Scholar]
- 9. El Tai NO, Osman OF, el Fari M, Presber W, Schönian G. 2000. Genetic heterogeneity of ribosomal internal transcribed spacer in clinical samples of Leishmania donovani spotted on filter paper as revealed by single-strand conformation polymorphisms and sequencing. Trans. R. Soc. Trop. Med. Hyg. 94:575–579 [DOI] [PubMed] [Google Scholar]
- 10. Fraga J, Montalvo AM, De Doncker S, Dujardin JC, Van der Auwera G. 2010. Phylogeny of Leishmania species based on the heat-shock protein 70 gene. Infect. Genet. Evol. 10:238–245 [DOI] [PubMed] [Google Scholar]
- 11. Ganguly S, Das NK, Barbhuiya JN, Chatterjee M. 2010. Post-kala-azar dermal leishmaniasis-an overview. Int. J. Dermatol. 49:921–931 [DOI] [PubMed] [Google Scholar]
- 12. Jaffe CL, McMahon-Pratt D. 1983. Monoclonal antibodies specific for Leishmania tropica. I. Characterization of antigens associated with stage- and species-specific determinants. J. Immunol. 131:1987–1993 [PubMed] [Google Scholar]
- 13. Montalvo AM, et al. 2010. Heat-shock protein 70 PCR-RFLP: a universal simple tool for Leishmania species discrimination in the New and Old World. Parasitology. 137:1159–1168 [DOI] [PubMed] [Google Scholar]
- 14. Nasereddin A, Bensoussan-Hermano E, Schönian G, Baneth G, Jaffe CL. 2008. Molecular diagnosis of Old World cutaneous leishmaniasis and species identification by use of a reverse line blot hybridization assay. J. Clin. Microbiol. 46:2848–2855 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Pacheco RS, et al. 1998. Parasite genotypically related to a monoxenous trypanosomatid of dog's flea causing opportunistic infection in an HIV positive patient. Mem. Inst. Oswaldo Cruz 93:531–537 [DOI] [PubMed] [Google Scholar]
- 16. Pandey K, et al. 2007. Characterization of Leishmania isolates from Nepalese patients with visceral leishmaniasis. Parasitol. Res. 100:1361–1369 [DOI] [PubMed] [Google Scholar]
- 17. Perry MR, et al. 2011. Visceral leishmaniasis and arsenic: an ancient poison contributing to antimonial treatment failure in the Indian subcontinent? PLoS Negl. Trop. Dis. 5:e1227 doi:10.1371/journal.pntd.0001227 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Siriwardana HV, Thalagala N, Karunaweera ND. 2010. Clinical and epidemiological studies on the cutaneous leishmaniasis caused by Leishmania (Leishmania) donovani in Sri Lanka. Ann. Trop. Med. Parasitol. 104:213–223 [DOI] [PubMed] [Google Scholar]
- 19. Srivastava P, et al. 2010. Detection of Leptomonas sp. parasites in clinical isolates of Kala-azar patients from India. Infect. Genet. Evol. 10:1145–1150 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Sundar S, Reed SG, Singh VP, Kumar PC, Murray HW. 1998. Rapid accurate field diagnosis of Indian visceral leishmaniasis. Lancet 351:563–565 [DOI] [PubMed] [Google Scholar]
- 21. Tamura K, et al. 2011. MEGA5: molecular evolutionary genetics analysis using maximum likelihood, evolutionary distance, and maximum parsimony methods. Mol. Biol. Evol. 28:2731–2739 [DOI] [PMC free article] [PubMed] [Google Scholar]