

Abstract
Background:
Here, we present to practicing spine surgeons and an even broader professional audience a case in which one spine surgeon, operating in his own outpatient surgery facility, performed a staggering number of procedures or “multiple operations on the same patient” (MOSP). In the vacuum of information regarding the multiply operated patient, the authors are without any guidance or even knowledge as to whether or not MOSP is a complete aberration or occurs with some documentable frequency within the medical/surgical profession.
Case Report:
The authors report a very extraordinary case of a woman, who, between April 4, 2000, and April 17, 2002, underwent 27 operative procedures on various parts of her spine. Within this same time frame, she additionally had one operation on each shoulder and an arthroscopy of the left knee. Each operation was performed at the same outpatient spine surgery center by the same surgeon and each was accompanied by a full operative report.
Conclusions:
As there is little information regarding MOSP, future documentation and reports are required so that the extent and degree of MOSP can be better evaluated. Furthermore, it is critical to examine multiple quality concerns, including indications for surgery, examination of patients’ personality traits in order to understand why one individual would subject herself to such a multitude of operations in such a short period of time, and some examination of the surgeon's motivations and practice patterns.
Keywords: Minimally invasive surgery, multiple operations, one patient
INTRODUCTION
Here, we present to practicing spine surgeons and an even broader audience how one patient was subjected to a staggering number of operations (27 on the spine and 3 on various other joints) within the space of only 2 years. The term “multiple operations on the same patient” (MOSP) was coined to describe this entity.
CASE REPORT
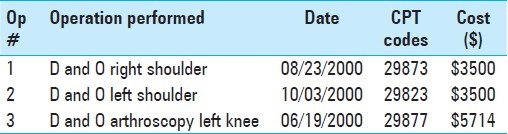
A 38-year-old female presented elsewhere in 1994 with cervical spine complaints, attributed to an earlier rear-impact motor-vehicle accident. Initial treatment included acupuncture, physical therapy, and a 1999 C5-6 posterior cervical laminectomy (7 cm posterior cervical scar). Postoperatively, she claimed she was “worse,” with occipital-parietal headaches, constant neck and bilateral arm pain accompanied by intermittent numbness, tingling, and weakness of both arms and hands. When she initially presented to the second surgeon (focus of this study), he established the following diagnoses: (1) neck pain with C4, C6, and C7 radiculopathy, bilaterally; (2) bulging discs C3-4, C4-5, C5-6, and C6-7; (3) stenosis, C5-6 and C6-7; (4) headaches; and (5) failed neck syndrome, status – post open cervical posterior laminectomy. Subsequent to the initial evaluation, examination date, and some appropriate cervical imaging studies, she underwent 27 spine operations, along with 3 other orthopedic operations. These were all performed over the course of a 2-year time period (April 2000 to April 2002). The surgical fees for the 27 spinal operations alone, based upon financial records and charges, totaled $231,006. The individual spine operations (in chronological order as outlined in the operative notes for each date) and surgical charges are listed in Table 1, along with the CPT codes.[1] Table 2 lists similar information for the non-spine related operations.
Table 1.
Spinal operations
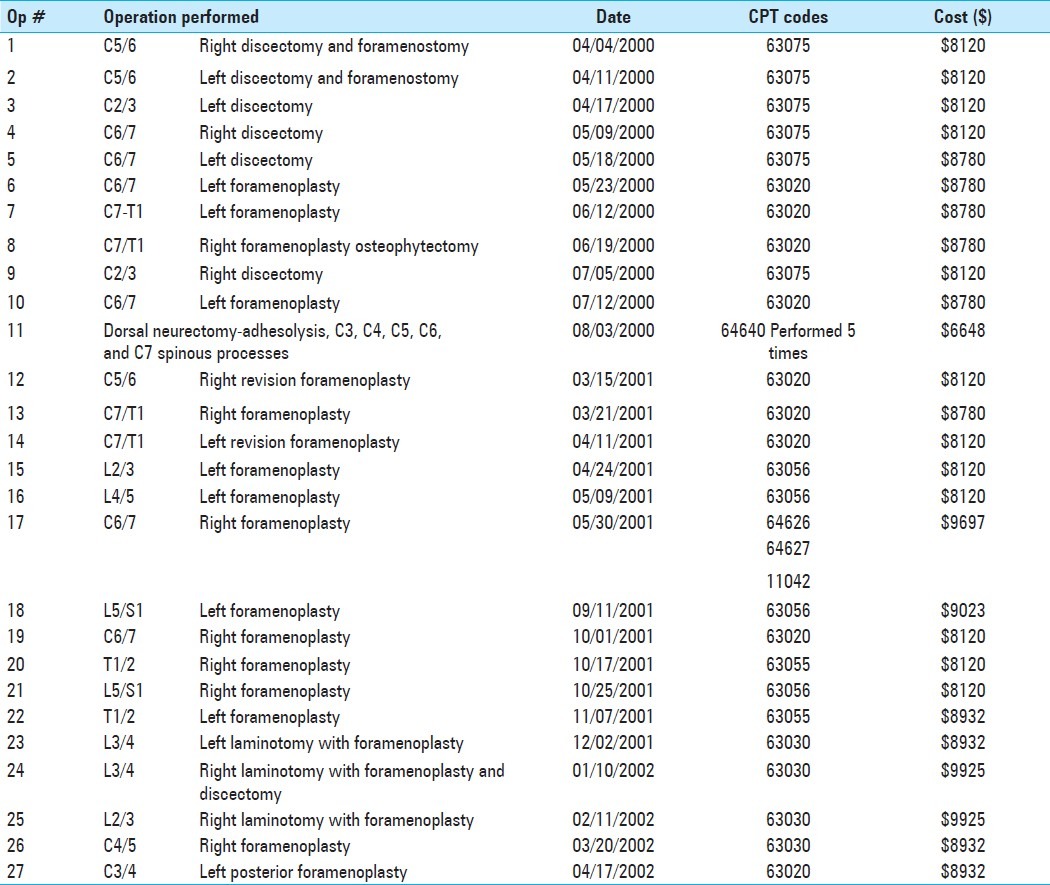
Table 2.
Joint operations
Surgical details
All of the operations performed were characterized as minimally-invasive. None of the CPT codes, however, in any way reflected the “minimally invasive” nature of any of the procedures. All were carried out in an ambulatory care setting/outpatient surgery center in a formal operating room, utilized Monitored Anesthesia Care (MAC; local anesthesia with intravenous sedation), and were documented as having an anesthesiologist, circulating nurse, and scrub nurse present. Each had a separate formal “Operative Report.”
Financial data
The “Patient Financial History” that documented the date of each and every service provided was 32 pages in length. It includes numerous charges for physical therapy, laboratory tests, diagnostic imaging services/studies, as well as the operations. Even after adjustments and “global write-offs,” the cost for 27 spine operations was $231,066. The patient subsequently estimated her total expenses at approximately $800,000, all of which were paid in cash. Since the surgeon “owned” all of the treatment facilities that provided the services (broken into different legal entities and names, but all directly or indirectly under his direction and control), this entire amount ultimately found its way into his hands.
Legal considerations
This patient came to the attention of the authors when she sought legal advice as to whether or not she had any legal causes of action against the surgeon. Neither author, one a neurological surgeon with 40 years of experience, the other a certified trial lawyer with 40 years of medical malpractice litigation experience (and some additional familiarity with this particular surgeon), had ever encountered a patient who had undergone so many operations. In fact, no laws or administrative regulations were violated by anything that occurred here. Unfortunately, the statute of limitations to bring a medical malpractice action and the statute of repose had both expired several years earlier.[3] Most importantly, if she had not requested legal advice, albeit far too late, this case would never have come to light.
DISCUSSION
Rarely have the frequency, extent, rationale, indications/quality indicators, and outcomes been reviewed for MOSP. In fact, no specific statistics or databases separately track information related to MOSP, either during a specific interval or throughout an individual's lifetime. In the literature reviewed, few spine surgery articles focused on re-operation rates; rather, most of the available information came from media reports. This lack of available information regarding MOSP makes the publication of this case report and the dissemination of this information even more compelling.
Two of the earliest accounts of MOSP were found in the British Medical Journal in 1899. In the first publication, one surgeon performed four operations within 7 weeks (for ruptured tubal pregnancy, suspected appendicitis, a stone in the ureter, and an exploration of the right kidney).[18] The patient died 4 h after the last operation. In the second paper, another surgeon performed eight operations in over 3 years (anterior colporrhaphy with perineoplasty, Alexander's operation, excision of the portio vaginalis and extirpation of the vaginal mucus membrane, cautery for prolapse of the anus, breast extirpation with axillary node removal, hysteropexy, laparotomy with bilateral oophrectomy for left ovarian cancer, and laparotomy for an intra-abdominal tumor of the left sacro-iliac region with the creation of an artificial anus).[28] This patient ultimately died from cancer.
In another case, an otolaryngologist operated on his own nurse 18 times for symptoms related to trauma (dizziness, hearing problems). These were repeated perilymph fistula repairs.[11] Each operative procedure cost about $10,000 (in 1989). The surgeon had an 8% financial interest in the “pioneering tilting hydraulic platform” manufactured by NeuroCom, alleged to have been useful in diagnosing and evaluating the condition of trauma-related dizziness.[12]
There are two recognized conditions that deal with the phenomenon of repeated plastic surgery. These are: Plastic/Cosmetic Surgery Addiction and Body Dysmorphic Disorder (BDD).[19,20,23] Although not always easily distinguishable, both of these compel afflicted patients to seek multiple cosmetic operations. BDD is recognized and incorporated into the DSM-IV, in section 300.7, where it is in the same category as hypochondriasis.[2] Media reports describe one patient who had undergone 14 “full-scale operations” and 52 cosmetic procedures (reportedly a world record for the most procedures ever undergone by one person). She had spent $100,000 on cosmetic surgery, including five facelifts.[27] Another media report describes a patient having 10 plastic surgery “treatments” in 1 day (mini-brow lift, Botox in the forehead and frown area, rhinoplasty revision, fat injections in cheeks, naso-labial folds, and lips, chin reduction, neck liposuction, ears pinned back, breast augmentation revision, liposuction on waist, hips, outer and inner thighs, and buttock augmentation).[7] Although there is little actual documentation available, Michael Jackson had allegedly undergone approximately 10 procedures by 1990, at which time he was 32 years old.[17,24] Although the patient presented in this report carried neither of these psychiatric diagnoses, she likely had either some type of a somatoform (DSM-IV 300.81 et al.) or factitious disorder (DSM-IV 300.19 et al.) which would explain her own behavior and response. This does not even begin to account for the surgeon's actions in doing 27 spinal operations in 2 years. When Newall wrote about informed consent for plastic surgery, she questioned whether a surgeon in a case of BDD has or should at some point have an ethical or moral obligation to either refuse to do more operations or, at a minimum, make a psychiatric referral on behalf of the patient, who would in these circumstances appear to be defenseless.[19]
“Multiple operations on the same patient” in the spine
Several literature reports have dealt with revision surgery following an “index” spine operation. Most have focused on the lumbar spine. In the majority of the spine articles reviewed, multiple re-operations typically meant 2-3 operations in a single individual. Deyo et al. reviewed 31,543 patients who underwent lumbar spine surgery between 2004 (the index operation year) and 2008. The 4-year re-operation rate was 17.2% for those with prior surgery versus 10.6% for those without prior operation.[8] Similarly, Malter reported a 15% incidence of re-operation 5 years after different types of lumbar surgical procedures were performed on 6376 patients in 1998.[14] Hu reported a 9.5% re-operation rate at 4 years following 4722 back operations performed in 1997.[13] When Walid analyzed 1153 patients undergoing spinal operations over 2-5 postoperative years, the overall re-operation rate was 10.4%. Although he made no specific mention of the number of re-operations, some patients in the series had undergone three or more procedures in the same spine region, but none had any operations at any other spinal level.[26] In the case presented in this study, the patient had 18 cervical operations, 2 thoracic operations, and 7 lumbar operations.
There are several other spine surgery series that focus on 2–3 re-operations performed on the same patient, but rarely more.[4,16,22,25] In the Spine Tango Database, there were 1330 (3.3%) secondary revisions/re-operations performed out of a total of 40,000 spinal procedures. Additionally, 74 patients (0.1%) underwent third operations. The average time from index operation to the first revision was 165 days, and to re-revision was 340 days.[22] In another relevant study, Martin et al. evaluated the incidence of repeat lumbar spine surgery at 90 days, 1 year, and 4 years following spinal operations performed in 29,529 patients (average age 47.5 years). The mean re-operation rate was 1.9% at 90 days (range 1.1-3.4%), 6.4% at 1 year (range 2.8–12.5%), and 13.8% at 4 years (range 8.1–24.5%). Notably, significant differences were noted for the adjusted mean re-operation rates of surgeons: 1.9% at 90 days (range 1.2–4.6%), 6.1% at 1 year (range 4.3–10.5%), and 13.2% at 4 years (range 10.0–19.3%). The authors observed, “…a large variation in re-operation rates across hospitals and surgeons after lumbar discectomies, a relatively simple spinal procedure. These findings suggest uncertainty about indications for repeat surgery, variations in perioperative care, or variations in quality of care.”[15]
The media contain several reports on MOSP. A Medicare database analyzed by the Wall Street Journal disclosed that one surgeon had an “unusual propensity” for performing multiple operations on the spine of individual patients.[5,6] One of his patients had six operations in less than 2 years, and he had even recommended a 7th operation. Between 2008 and 2009, this same surgeon performed spinal fusions on 61 Medicare patients. In 16 of these, he did 24 additional fusions. In one case, he admitted that after seven spine operations and $175,000, none of this had improved his patient's condition. One woman who sued for malpractice alleged that she had been operated on by him five times in less than 13 months. Another patient alleged that three operations had been performed in less than 5 months. The surgeon's overall rate for that time period was 39 additional fusions per 100 initial fusions, the highest rate in the nation among surgeons who performed spinal fusions on 20 or more Medicare patients. A spine surgeon, who was also at that time the president of the Association for Medical Ethics, commented on this surgical record, observing that “When you get a number like six or seven surgeries on someone's spine in a short period of time, that starts to be suspicious.”[5] More recently, Epstein and Schwall reported on re-operation rates (in 2010 at one institution) for 177 patients undergoing instrumented spinal fusions (all levels) utilizing INFUSE (off-label 96% of the time). Most critically, the re-operation rate was 20% for all age groups, but was 40% for patients over 65 years of age.[10]
The patient reported here had multiple “decompressions” but no spinal fusions, no use of INFUSE, and no instrumentation or other “predisposing factors” that might otherwise account for any of these 27 spinal operations.
In this case of MOSP, there must be some concern for the necessity or indications for each procedure. Porchet et al. developed criteria to determine the appropriate indications for lumbar laminectomy using the standard procedure developed at the RAND Corporation and UCLA as far back as 1999. Retrospectively applying these criteria to the medical records of 196 patients who had been operated on in Switzerland, they reported that 23% of these operations were inappropriate.[21] Recently, Epstein and Hood, using defined criteria, evaluated 274 consultations performed over 1 year in patients with either cervical or lumbar disc disease. They concluded that of 45 patients who were advised to have surgery by outside surgeons, none had either neurological deficits or significant pathological radiographic findings. Two who were advised to have lumbar surgery had cervical disease. Based upon the stated criteria, 47 or 17.2% of these 274 spinal consultations were scheduled for unnecessary spine surgery.[9] In the case presented here, we recognize the lack of necessity or indications for any of these procedures comprised just one of a host of quality concerns raised based solely upon the number of operations.
CONCLUSIONS
This case report focuses on a single individual who underwent 27 spinal operations involving the cervical (18), thoracic (2), and lumbar (7) regions, within just a 2-year period of time. It has existed below the radar of all health-care professionals, regulatory agencies, health-care organizations, insurance carriers, and state medical licensing boards. This vacuum of information regarding MOSP in the medical literature prevents anyone from ascertaining whether or not this is a completely isolated circumstance. A litigation inquiry uncovered this case, which would not have otherwise been exposed. Without exposure and reporting of this and any potential similar cases, there can be no scrutiny by the health profession, regulatory agencies, or the public, and therefore no means to oversee such incidents or impose any quality controls.
Footnotes
Disclaimer: The authors of this paper have received no outside funding and have nothing to disclose.
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2012/3/4/238/98578
Contributor Information
Fred L. Cohen, Email: vannefred@aol.com.
Gary W. Roberts, Email: gary@palmbeachtrialattorney.net.
REFERENCES
- 1.Abraham M, Beebe M, Dalton J, Evans D, Glenn R, Green G, et al. Current procedural terminology (CPT 2010) Standard ed. American Medical Association; 2009. [Google Scholar]
- 2.Diagnostic and statistical manual of mental disorders. 4th ed. Washington, DC: Corporate Author (TR#300.7 Body Dysmorphic Disorder.); 2000. American Psychiatric Association. text rev. [Google Scholar]
- 3.Black's Law Dictionary. 6th ed. St. Paul, Minnesota: West Minneapolis; 1990. p. 927. [Google Scholar]
- 4.Blue Distinction (Blue Distinction Centers for Spine Surgery Program, Program Selection Criteria for 2010 mid-point designations. Blue/DistinctionsSpine/Criteria/rev.12/08/10 [Google Scholar]
- 5.Carreyrou J, McGinty T. Medicare records reveal troubling trail of surgeries. Wall St J. 2011;257:72. [Google Scholar]
- 6.Carreyrou J, McGinty T. Hospital bars surgeon from operating room. [Last accessed on 2011 Apr 13]. Available from: http://online.wsj.com/article/SB10001424052748704336504576259142044058726.html .
- 7.Daily Mail Reporter. “I had 10 plastic surgery treatments in one day,” boasts new-look The Hills star Heidi Montag, 23. [Last accessed on 2012 Mar 7]. Available from: http://www.dailymail.co.uk/tvshowbiz/article-1244464/Heidi-Montag-Before-plastic-surg .
- 8.Deyo RA, Martin BI, Kreuter W, Jarvik JG, Angler H, Mirza SK. Revision surgery following operations for lumbar stenosis. J Bone Joint Surg Am. 2011;93:1979–86. doi: 10.2106/JBJS.J.01292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Epstein NE, Hood DC. “Unnecessary” spinal surgery: A prospective 1-year study of one surgeon's experience. Surg Neurol Int. 2011;2:83. doi: 10.4103/2152-7806.82249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Epstein NE, Schwall GS. Costs and frequency of “off-label” use of INFUSE for spinal fusions at one institution in 2010. Surg Neurol Int. 2011;2:115. doi: 10.4103/2152-7806.83929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Hain TC. Perilymph fistula. Personal Communication with F.C. Tuesday 4/19/11. [Last accessed on 2012 Mar 7]. Available from: http://www.dizziness-and-balance.com/disorders/unilat/fistula.html .
- 12.Harris M. Peer review's limits visible once again. (9-14).Am Med News. 1989;32:1. [Google Scholar]
- 13.Hu RW, Jaglal S, Axcell T, Andersoin G. A population-based study of reoperations after back surgery. Spine (Phila Pa 1976) 1997;22:2265–70. doi: 10.1097/00007632-199710010-00013. [DOI] [PubMed] [Google Scholar]
- 14.Malter AD, McNeney B, Loeser JD, Deyo RA. 5-year reoparation rate after different types of lumbar spine surgery. Spine (Phila Pa 1976) 1998;23:814–20. doi: 10.1097/00007632-199804010-00015. [DOI] [PubMed] [Google Scholar]
- 15.Martin BI, Mirza SK, Flum DR, Wickizer TM, Heagerty PJ, Lenkoski AF, et al. Repeat surgery after lumbar decompression for herniated disc: The quality implications of hospital and surgeon variation. Spine J. 2012;12:89–97. doi: 10.1016/j.spinee.2011.11.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Maven semantic: Spinal surgery research database. [Last accessed on 2012 Mar 7]. Available from: http://businesswire.com/news/home/20110201007164/en/Maven-Semantic-Spinal-S .
- 17.Michael Jackson's Health and Appearance. Wikipedia. [Last accessed on 2012 Mar 7]. Available from: http://en.wikipedia.org/wiki/Michael_Jackson's_health_and_appearance .
- 18.Munde P. Multiple surgery on one patient. BMJ. 1899:671. [Google Scholar]
- 19.Newell BL. Informed consent for plastic surgery, does it cut deeply enough? J Leg Med. 2011;32:315–35. doi: 10.1080/01947648.2011.600171. [DOI] [PubMed] [Google Scholar]
- 20.Plastic Surgery Addiction. [Last accessed on 2012 Mar 7]. Available from: http://ehe.osu.edu/cs/bitf/issues/plastic-surgery.php .
- 21.Porchet F, Vader JP, Larequi-Lauber T, Costanza MC, Burnand B, Dubois RW. The assessment of appropriate indications for lamiinectomy. J Bone Joint Surg Br. 1999;81-B:234–9. doi: 10.1302/0301-620x.81b2.8871. [DOI] [PubMed] [Google Scholar]
- 22. Spine Tango Database. Christoph Roder, M.D., PhD, MPH, Associate professor, director a.i. MEM Research Center, Institute for Evaluative Research in Medicine, University of Bern, E-mail: cristoph.roeder@memcenter.unibe.ch.
- 23.Suissa AJ. Addiction to cosmetic surgery: Representations and medicalization of the body. Int J Ment Health Addict. 2008;6:619–30. [Google Scholar]
- 24.Taraborreli JR. The magic and the madness. Terra Alta, WV: Headline. 2004 [Google Scholar]
- 25.Utku S, Baysal H, Zileli M. Spine surgery database: A Turkish registry for spinal disorders. Turk Neurosurg. 2010;20:223–30. doi: 10.5137/1019-5149.JTN.2538-09.1. [DOI] [PubMed] [Google Scholar]
- 26.Walid MS, Robinson JS, 3rd, Abbara M, Tolaymat A, Robinson JS., Jr De novo spine surgery as a predictor of additional spine surgery at the same or distant spine region. Ger Med Sci. 2011;9:10. doi: 10.3205/000133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Watt N, Clarke S. Cindy Jackson sets world record with 52 plastic surgeris, cosmetic procedures. 2011. Apr 5, [Last accessed on 2012 Mar 7]. Available from: http://abcnews.go.com/International/cindy-jackson-sets-world-record-52-plastic-surgery .
- 28.Williams WR. Multiple operations on a single patient. BMJ. 1999;319:757B. [PMC free article] [PubMed] [Google Scholar]