

Abstract
A number of variations in the pulmonary arteries and veins have been documented, and the information is very important for performing a safe lung resection. This report describes a case of an anomalous segmental vein of the left upper lobe of the lung. The patient was a 75-year old male who was suspected to have lung cancer in the left upper lobe. A contrast-enhanced computed tomography showed a vessel behind the left lower bronchus. A three-dimensional computed tomography angiography demonstrated that it was an anomalous vein for the apicoposterior segment of the left upper lobe of the lung, draining into the left inferior pulmonary vein. The aberrant vein was readily identified during surgery and was divided without injury, and a left upper lobectomy was successfully performed. Aberrant pulmonary veins for the superior segment of the right upper lobe of the lung are rarely observed, and the same kind of anomaly on the left side has not been reported.
Keywords: Three-dimensional computed tomography, Angiography, Anomalous pulmonary vein, Left lung
INTRODUCTION
A number of variations in the pulmonary arteries and veins have been documented, and the preoperative recognition of the delineation is very useful in performing a safe lung resection. A three-dimensional computed tomography has the advantage of a clear identification of the pulmonary vessel branches, even at the subsegmental and more peripheral levels. This report describes a case of an anomalous segmental vein of the left upper lobe of the lung, draining into the left inferior pulmonary vein, which was clearly demonstrated with the three-dimensional computed tomography angiography.
CASE REPORT
A 75-year old male was admitted for treatment due to a suspected diagnosis of lung cancer. He had no symptoms or illness. A chest roentgenogram and computed tomography revealed a consolidated lesion in the left upper lung field. The tumour mass measuring 1.7 × 1.5 × 1.5 cm was located in the left upper lobe. A positron emission tomography with fluorine-18-fluorodeoxyglucose was positive for the mass, and the clinical stage of the tumour was diagnosed as T1aN0M0. A preoperative contrast-enhanced computed tomography showed a vessel behind the left lower bronchus (Fig. 1a, white arrow). The three-dimensional computed tomography angiography demonstrated that it was an anomalous vein from the apicoposterior segment of the left upper lobe of the lung, draining into the left inferior pulmonary vein (Fig. 1b, black arrow).
Figure 1:
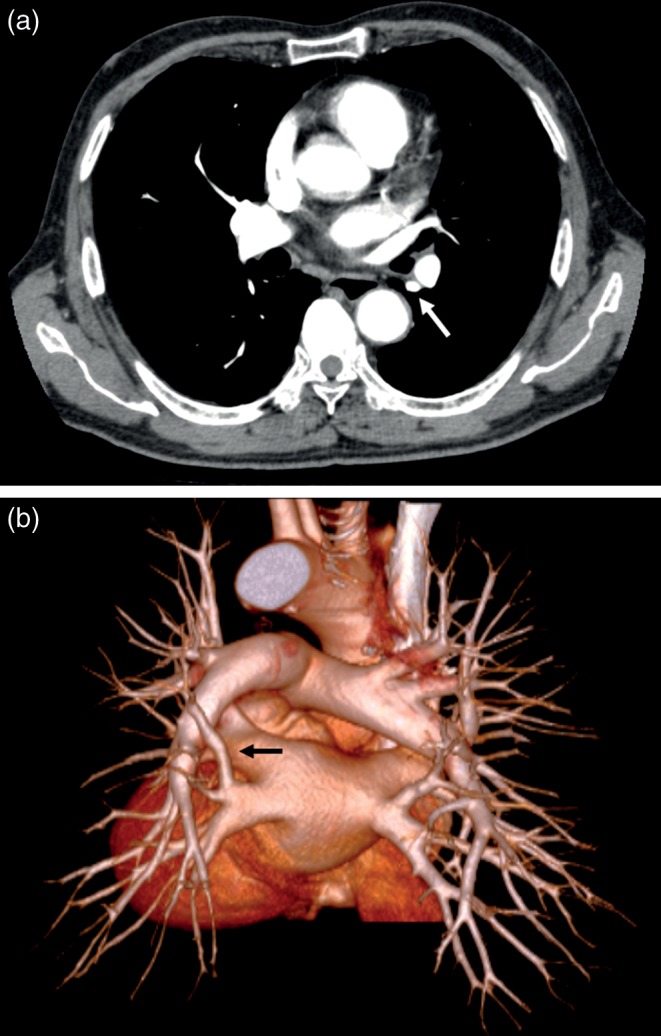
(a) A contrast-enhanced computed tomography showed a vessel behind the left lower bronchus (white arrow). (b) A three-dimensional computed tomography angiography demonstrated that it was an anomalous vein from the apicoposterior segment of the left upper lobe of the lung, draining into the left inferior pulmonary vein (black arrow).
He underwent a left upper lobectomy through a posterolateral thoracotomy. The anomalous vein was easily identified between the left upper and lower lobes behind the hilum (Fig. 2, black arrow) and was confirmed to drain into the inferior pulmonary vein. The superior pulmonary veins and arteries of the left upper lobe from the anterior hilum were divided and dissected. The aberrant vessel was ligated and cut, and then a left upper lobectomy was safely performed. The postoperative course was uneventful.
Figure 2:
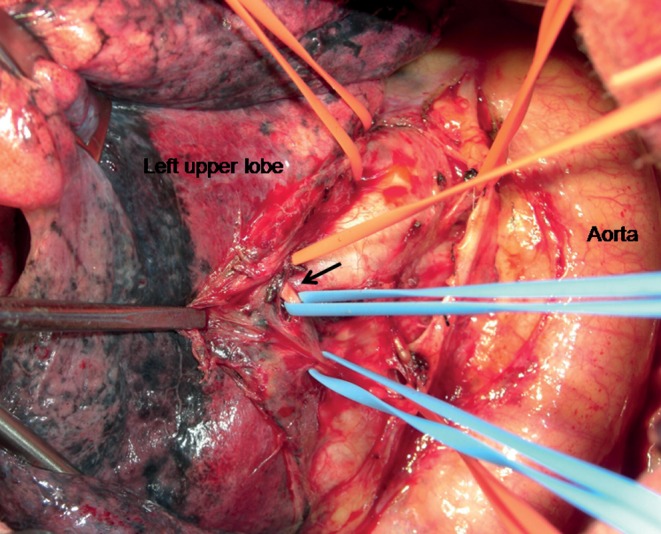
A intraoperative view showing an anomalous segmental vein (black arrow).
DISCUSSION
Anatomical variations of the pulmonary arteries and veins are associated with a potential risk of bleeding during pulmonary resections. The preoperative identification of individual vessel configurations is very important for safe and proper procedures in lung surgery.
Kim et al. [1] first reported the contrast-enhanced CT findings of aberrant pulmonary veins, which were observed as a focal nodularity attached to the posterior wall of the bronchus intermedius. Those vessels were the right superior segmental pulmonary veins of the upper lobe draining into the inferior pulmonary vein or left atrium and were observed in 5% of the right side in normal subjects. These abnormal drainage veins of the right upper lobe occur in 5.7% of patients who undergo surgical resection of the right lung [2]. On the other hand, the same kind of anomaly has not yet been reported on the left side, and therefore, the present case is the first such case ever to be reported.
Watanabe et al. [3] and Usami et al. [4] reported that three-dimensional computed tomography angiography is a far less invasive and an easier method for delineation of the pulmonary vessels for lung resection than conventional pulmonary angiography.
The three-dimensional computed tomography is now widely available, and it has the advantages of the clear identification of pulmonary vessel branches, even at the subsegmental and more peripheral levels. Such preoperative information is very helpful for pulmonary resection. A preoperative three-dimensional computed tomography angiography provided a great advantage in the current case. The aberrant vein was readily identified during surgery and divided without injury.
Video-assisted thoracic surgery (VATS) has recently become a common surgical modality worldwide. The three-dimensional computed tomography angiography could provide a very useful visual information of variations of pulmonary vessels, which is crucial for VATS. Consequently, surgeons can easily to simulate the surgical process either before or even during a thoracotomy.
The three-dimensional computed tomography angiography was very useful for the detection of individual vessel configurations and the aberrant vein. The imaging modality will become essential for the preoperative evaluation of pulmonary vessels including abnormal vessels during lung surgery.
Conflict of interest: none declared.
REFERENCES
- 1.Kim J, Choi D, Lee K. CT of the bronchus intermedius: frequency and cause of a nodule in the posterior wall on normal scans. Am J Roentgenol. 1995;165:1349–52. doi: 10.2214/ajr.165.6.7484561. [DOI] [PubMed] [Google Scholar]
- 2.Asai K, Urabe N, Yajima K, Suzuki K, Kazui T. Right upper lobe venous drainage posterior to the bronchus intermedius: preoperative identification by computed tomography. Ann Thorac Surg. 2005;79:1866–71. doi: 10.1016/j.athoracsur.2004.12.014. [DOI] [PubMed] [Google Scholar]
- 3.Watanabe S, Arai K, Watanabe T, Koda W, Urayama H. Use of three-dimensional computed tomographic angiography of pulmonary vessels for lung resections. Ann Thorac Surg. 2003;75:388–92. doi: 10.1016/s0003-4975(02)04375-8. [DOI] [PubMed] [Google Scholar]
- 4.Usami N, Iwao S, Mizuno T, Taniguchi T, Yokoi K. Three-dimensional angiography of aberrant segmental vein of right upper lobe. Asian Cardiovasc Thorac Ann. 2010;18:398. doi: 10.1177/0218492310375005. [DOI] [PubMed] [Google Scholar]