

Abstract
Spontaneous coronary artery dissection is a rare cause of acute coronary syndrome, particularly seen in women during pregnancy or in the puerperium. It has a high acute phase mortality. The etiology is uncertain. Hormonal changes during pregnancy, hemodynamic stress and changes in the autoimmune status have been considered as possible etiological factors. A timely diagnosis and institution of appropriate treatment is important for a successful outcome. There is no consensus of opinion for optimal treatment. Conservative management, coronary artery bypass graft surgery, and percutaneous coronary intervention, all have been described in the literature as possible therapeutic options. Spontaneous coronary artery dissection should be considered as a differential in any young woman presenting with chest pain associated with pregnancy. We report two cases of pregnancy-associated spontaneous coronary artery dissection, both successfully managed, along with a comprehensive review of the previously published literature.
Keywords: Acute coronary syndrome, pregnancy-associated coronary artery dissection, pregnancy-related myocardial infarction, spontaneous coronary artery dissection
INTRODUCTION
Spontaneous coronary artery dissection (SCAD) is an infrequent cause of acute coronary syndrome (ACS),[1,2] mainly affecting fairly young[3,4] otherwise healthy women. About 26 – 38% of cases occur in late pregnancy, peripartum or postpartum.[1,3–7] The condition mainly involves left main stem or left anterior descending artery or both.[1,7–10] It was first reported by Pretty,[11] in 1931, in a young Caucasian woman who had a sudden death after developing chest pain. Since then only 116 cases have been reported in the literature. The incidence has been reported to range from 0.1 – 1.1%.[12–15] The etiology of primary SCAD remains uncertain.
Urgent coronary angiography and intravascular ultrasound (IVUS) are indicated in the acute phase in order to establish the diagnosis and determine the best therapeutic approach.[7,8,16] Medical therapy, percutaneous coronary intervention (PCI) and coronary artery-bypass grafting (CABG) have been applied in the acute phase[17] but optimal therapy is yet to be determined.[8] Sudden death is the most common presentation, reported in 60 – 80% of the cases[3] whilst patients may also present with chest pain with or without ECG changes.
We present two cases of pregnancy-related SCAD, both successfully managed, one with conservative treatment and the other with intracoronary stent implantation. A comprehensive review of the published literature since it was first reported in 1931 is presented.
CASE 1
A 41-year-old woman, G3P3, previously fit and well, presented with a history of intermittent chest pains, which started 5 days after an uneventful delivery of her third child. Her chest pain became progressively worse and intolerable, which forced her to call the emergency medical services. The ECG manifested ST elevation across the antero-lateral leads with reciprocal ST depression in the inferior leads [ECG 1].
ECG 1.
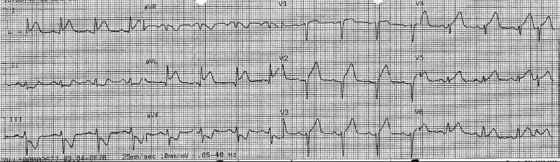
ECG of case 1 showing ST elevation across the antero-lateral leads with reciprocal ST depression in the inferior leads
She was a smoker and was known to have hypercholesterolemia. The patient denied any illicit drug use. There was no history of any connective tissue disease and no significant family history of ischemic heart disease. Her antiphospholipid antibodies were negative.
She underwent emergency coronary angiography, which demonstrated an occlusion of the LAD at its ostium, with appearances suggestive of dissection and no flow-limiting disease elsewhere [Figure 1a]. The patient underwent primary percutaneous coronary intervention after pre-dilatation and a Vision 3.5 × 28 mm bare metal stent (BMS) was implanted in the LAD [Figure 1b]. The procedure was well tolerated. This led to the restoration of Thrombolysis in Myocardial Infarction (TIMI) III flow, resolution of her pain and ECGs.
Figure 1.

Angiography (right anterior oblique cranial projection) of the left anterior descending artery. (a) Initial angiogram demonstrating total occlusion of the proximal left anterior descending artery (arrow); (b) In the same projection as in A, after deployment of a stent in the proximal left anterior descending artery (arrow). Thrombolysis in myocardial infarction (TIMI) III flow was demonstrated. LAD – Left anterior descending artery; LCx - Left circumflex artery
The day after the procedure she became breathless and was found to be in pulmonary edema. She was treated with diuretics. Her subsequent echocardiogram revealed severe impairment of left ventricular systolic function with akinesis of the anterior septum, anterior wall, lateral wall, and apex.
She improved and was discharged home on aspirin, clopidogrel, beta-blocker, ACE-inhibitor, frusemide, and statin.
CASE 2
A 28-year-old woman, G3P3, 3 weeks postpartum, presented with sudden onset of pain in the left arm followed by severe central chest pain without any associated symptoms. She had a similar episode of left arm pain and chest pain a week prior to her presentation, which lasted for a few hours and settled spontaneously. An ECG showed an antero-lateral ST elevation myocardial infarction (STEMI) [ECG 2]. The pain was relieved with intravenous morphine.
ECG 2.
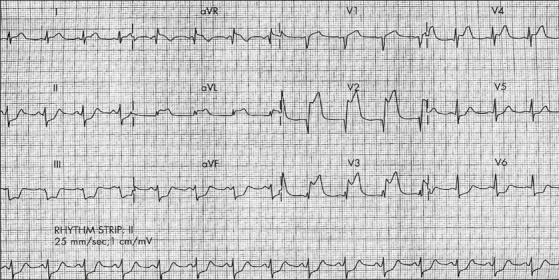
ECG of Case 2 showing ST elevation in the antero-lateral leads.
The only cardiovascular risk factor she had was smoking (she had a history of 13-pack years of smoking). There was no history of connective tissue disease and she denied any illicit drug use. The antiphospholipid antibodies were negative. Coronary angiography revealed a dissection of the LAD from the ostium to the first diagonal [Figure 2a]. Her chest pain settled with resolution of her ECGs and she was hemodynamically stable. A decision was therefore made to manage her conservatively. She was commenced on aspirin, clopidogrel, low-molecular weight (LMW) heparin, nitrates, beta-blocker, and ACE inhibitor. She was started on glycoprotein IIb/IIIa inhibitor (Tirofiban) for the next 72 hours. Her echocardiogram demonstrated preserved left ventricular function with normal dimensions and no regional wall motion abnormalities.
Figure 2.

Angiography of the left anterior descending artery; (a) Initial angiogram (left anterior oblique caudal projection) showing dissection of the anterior descending artery from the ostium to the first diagonal (arrow); (b) Repeat angiogram (left anterior oblique cranial projection) after one week (arrow); (c) After three months (left anterior oblique caudal projection) (arrow). LAD – Left anterior descending artery; LCx – Left circumflex artery
After one week, a repeat angiogram showed the persistence of the dissection flap but the thrombus had disappeared [Figure 2b]. After 5 days, the patient was discharged home on medical therapy. The patient remained asymptomatic when reviewed at 3 months and a repeat angiogram revealed a healed dissection flap [Figure 2c].
DISCUSSION
We undertook a comprehensive review of the literature since it was first reported in 1931. We searched ‘Medline’ and ‘PubMed’ using the MESH headings ‘pregnancy-related myocardial infarction’, ‘pregnancy-related coronary artery dissection,’ and ‘spontaneous coronary artery dissection’ and ‘acute coronary syndrome in pregnancy’. A manual search of the bibliographies of all selected reports was then performed. Koul et al.,[7] in 2001, reported 58 cases of pregnancy-associated SCAD (p-SCAD) between 1952 and 1999. Appleby et al.,[18] in 2009, reported additional 25 cases of p-SCAD between 1999 and 2008. A total of 118 case reports have been published since 1952, including our two cases [Table 1].
Table 1.
Pregnancy – related spontaneous coronary artery dissection
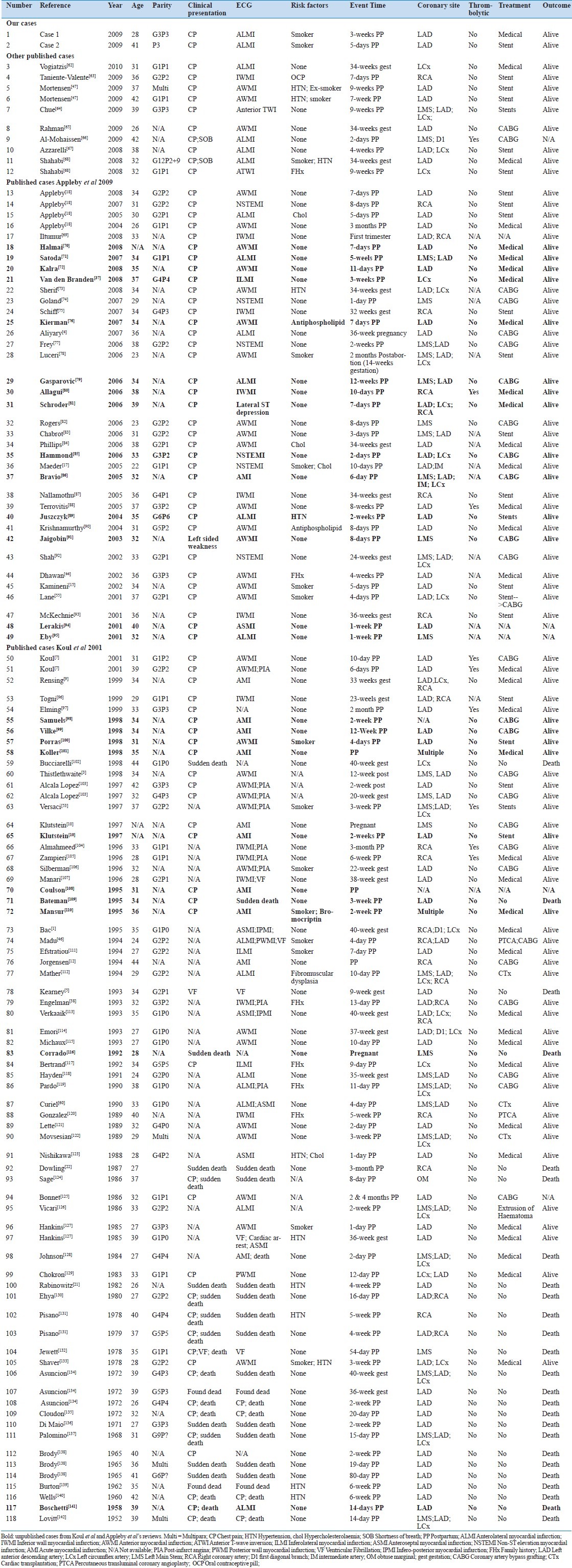
Our search revealed another 10 cases (case number 55, 56, 57, 58, 65, 70, 71, 72, 83, 117) between 1952 and 1999, which were not included by Koul et al.,[7] in their literature review [Table 1]. Between 1999 and 2008, there were additional 14 cases (case number 18, 19, 20, 21, 25, 29, 30, 31, 35, 37, 40, 42, 48, 49), which were not included by Appleby et al., in their review of the literature [Table 1]. Between 2008 and 2010, there were 10 case reports published.
The mean age at presentation was 32.62 years (youngest 22 years; oldest 44 years). The mean parity was 1.08. The earliest reported case was at first trimester and the latest was at 3 months postpartum. There were 92 (77%) postpartum reported cases (earliest 2 days postpartum; latest 3 month postpartum) and 27 (23%) cases during gestation (earliest 20 weeks pregnancy; latest 40 weeks gestation).
Pathogenesis
The pathogenesis of SCAD is unknown. The body undergoes different hormonal and hemodynamic changes during pregnancy and in the post-partum period; it may take upto six months after delivery for the body to achieve the pre-pregnancy status. Several theories have been postulated with regards to p-SCAD. It is suggested that the morphological changes in arterial wall associated with hemodynamic changes may be a contributory factor. Excess progesterone during pregnancy induces the loss of normal corrugation of elastic fibres and degeneration of medial wall collagen and all this may result in weakening of the arterial wall leading to arterial dissection. Heafner et al.,[19] suggested a two-step process leading to SCAD: an initial intimal rupture followed by delayed bleeding in tunica media likely caused by the clotting changes that occur in pregnancy. Bleeding from vasa vasorum into tunica media has been proposed as a possible cause of arterial dissection.[12,20] Robinowitz et al., postulated an association with vasculitis and peri-adventitial infiltrates composed of eosinophilic lymphocytes or histiocytes.[21] Dowling et al.,[22] proposed that peri-adventitial inflammation were a consequence of SCAD and not the actual cause.
Cocaine abuse and the strenuous physical exercise have been suggested as possible causes.[23–26] Koul et al.,[7] postulated that the hemodynamic changes that occur during pregnancy may initiate the intimal tear and subsequent hemorrhage into the media of coronary artery.
Other factors such as use of oral contraceptives, immunosuppressant drugs, drug reactions, blunt trauma to chest,[27] type IV Ehlers Danlos syndrome[28] Marfan's syndrome,[29] and α1-antitrypsin deficiency[30] have also been described as possible mechanisms leading to arterial dissection.[31–34] Crystal medial necrosis has also been implicated in SCAD.[35]
How do patients present?
The most common presentation is acute coronary syndrome but the severity may range from unstable angina to acute myocardial infarction and cardiogenic shock. The disease is associated with high mortality about 50% at presentation.[12] Sudden death without evidence of myocardial infarction is much more frequent.[36] The mortality exceeds 70% for patients who present with myocardial infarction.[37] The survival rate is fairly good, about 85%, for patients who survive the acute phase.[38] Survival is possible in patients if luminal obstruction is incomplete or with myocardial infarction without serious complications.[39–42]
Risk factors
A review of the literature revealed that 76 (64%) did not have any risk factors; 7 (6%) had multiple risk factors, while risk factors in others included antiphospholipid 2 (1.68%), fibromuscular dysplasia 1 (0.84%), positive family history of ischemic heart disease 6 (5%), hypercholesterolemia 2 (1.68%), hypertension 7 (5.88%), smoking 11 (9%), oral contraceptives 1 (0.84%); risk factors were unknown in 6 (5%) cases. There is an increased risk of SCAD in patients with advancing age and multiparity.[43]
Diagnosis
There should be a high degree of suspicion of SCAD in any young peripartum or postpartum lady presenting with chest pain. If the index of suspicion of a cardiac ischemic event is high, despite any perceived lack of cardiac risk factors, urgent coronary angiography should be considered.[2,3,44–46]
Angiographic Diagnosis
SCAD occurs in normal coronary vessels. The dissection can involve both right and left coronary arteries. Kemineni et al., reviewed 154 cases and reported that left anterior descending (LAD) artery was frequently involved in women (66% vs 41%) and right coronary artery (RCA) is commonly involved in men (50% vs 28%).[15]
A review of the published literature revealed that LAD was involved in 49 (41%) of cases and RCA in 13 (11%); 42 (35%) had multivessel dissection. Other vessels were less frequently involved: LMS 7 (6%), LCx 5 (4.2%), OM 1 (0.84), and no information was available in 2 (1.68%) cases.
Management
The guidelines for the optimal management of SCAD have yet to be established. The published data describes different management strategies including conservative treatment, percutaneous coronary intervention, coronary artery bypass grafting (CABG),[1–7,38] and heart transplantation.[1]
The factors that may influence the decision regarding the best treatment option include
Hemodynamic stability of the patient
Site of dissection
Number of vessels involved
Availability of coronary intervention services
Mortensen et al., in Western Denmark Heart Registry Study, mentioned that the location and the extent of the dissection guided their treatment strategy:
Lesions that involved LMS were treated with CABG
Proximal lesions of LAD, LCx and RCA were treated with PCI, and
Distal lesions were managed conservatively.[47]
Conservative Management
The conservative management may include use of heparin, beta blockers, calcium channel blockers, nitrates, diuretics, antiplatelet therapy including aspirin, clopidogrel, and glyprotein IIb/IIIa inhibitors.[48,49]
The information regarding the safety of some of these drugs in pregnancy is limited. The drugs, which may be administered safely during pregnancy include unfractionated heparin or LMW heparin, aspirin, beta blockers, nitrates, morphine, and frusemide. Angiotensin-converting enzyme inhibitors and angiotensin receptor blockers are contra-indicated due to the risks to the fetus.[47,50] Clopidogrel is not recommended during breast feeding; its safety in pregnancy is however unknown. The safety of glycoprotein IIb/IIIa inhibitors in pregnancy is not known.
Atay et al., suggested that patients who have completed an acute event or those with no evidence of ongoing ischemia and no significant stenosis on cardiac catheterisation may do well with conservative treatment in short term but most of these patients have had recurrent angina, subsequent myocardial infarction or sudden death due to extension of dissection.[51]
Thrombolysis
The use of thromboytics in pregnancy remains controversial. They may resolve the thrombus in the false lumen leading to improvement of the flow in the true lumen.[52] They may lead to further extension of the existing dissection by lysing a false lumen thrombus.[2,53] Pregnancy therefore remains a relative contraindication to thrombolytic therapy[48] and is best avoided in these circumstances. The literature review revealed that the thrombolytics were used in 9 (7.56%); 96 (86%) did not have any thrombolytics. No information was available in 14 (12%) cases.
Percutaneous coronary intervention
Percutaneous coronary intervention is the treatment of choice in SCAD with involvement of a single vessel with ongoing ischemia.[16] Whether Drug-Eluting Stents(DES) have any benefit over BMS in the setting of SCAD is not known and there have been no trials due to the rare occurrence of the condition.
Coronary Artery Bypass Grafting (CABG)
Paez et al., reported a case treated with revascularisation surgery, ventricular assistance and heart transplant.[54] CABG is the preferred mode of treatment in patients with Left Main Stem (LMS) dissection, multivessel dissection or complex lesions[3,17,23,44,55–57] or in patients with failed coronary intervention.[16]
Surgical myocardial revascularisation has been shown to achieve good results[56,58,59] and is considered to be the first line treatment when multiple vessels are involved.[60] One of the major problems with CABG is that it is difficult to clearly identify the true lumen, which may result in grafting of the false lumen leading to irreversible myocardial damage or death.[16] Heart transplantation has been tried with success in cases of severe heart failure following a coronary artery dissection.[61]
Prognosis
The prognosis of patients with SCAD is poor. Benham et al., in their review of 123 cases reported death in 67% of patients, whilst 33% survived treated either conservatively or by surgery.[62] Jorgensen et al., reported 100% survival in a series of 10 consecutive patients who underwent surgical treatment.[12]
A review of the literature showed that 36 (30.25%) were treated medically; 25 (21%) had CABG, 25 (21%) had PCI, 3 (2.52%) had heart transplant, 1 (0.84%) had extrusion of hematoma, 2 (1.68%) had PCI and CABG, 24 (20.16%) did not have any treatment. Information was not available in 3 (2.52%) cases. Eighty-nine (75%) cases survived, whilst 25 (21%) died; no information was available in 5 (4.2%) cases.
The prognosis of SCAD has improved in the recent years. An overall mortality of 66% was reported by Engleman et al., in a retrospective study in 1993.[63] More recently, Koul et al., in 2001 reported a much lower mortality of 38%.[7] Last reported death because of SCAD was in 1998, according to the literature review.[7] First reported alive case was in 1978.[7] Between 1952 and 1999, out of 64 cases, 37 (58%) cases survived; 25 (39%) cases died. No information available in 2 (3%) cases. Between 1999 and 2010, out of 55 cases, there was no reported death. No information was available in 3 (5.4%) cases.
CONCLUSIONS
SCAD is a relatively common cause of acute myocardial infarction in young women who are pregnant or in the puerperium. A high index of suspicion is critically important when dealing with any young woman presenting with chest pain associated with pregnancy. A timely diagnosis of this fatal condition helps in deciding about the appropriate treatment and a successful outcome.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Bac DJ, Lotgering FK, Verkaaik AP, Deckers JW. Spontaneous coronary artery dissection during pregnancy and postpartum. Eur Heart J. 1995;16:136–8. doi: 10.1093/eurheartj/16.1.136. [DOI] [PubMed] [Google Scholar]
- 2.Badmanaban B, McCarty D, Mole DJ, McKeown PP, Sarsam MA. Sponataneous coronary artery dissection presenting as cardiac tamponade. Ann Thorac Surg. 2002;73:1324–6. doi: 10.1016/s0003-4975(01)03240-4. [DOI] [PubMed] [Google Scholar]
- 3.Thistlethwaite PA, Trazi RY, Giordano FJ, Jamieson SW. Surgical management of spontaneous left main coronary artery dissection. Ann Thorac Surg. 1998;66:258–60. doi: 10.1016/s0003-4975(98)00382-8. [DOI] [PubMed] [Google Scholar]
- 4.Aliyary S, Mariani MA, Verhorst PM, Hartmann M, Stoel MG, von Birgelen C. Staged therapeutic approach in spontaneous coronary dissection. Ann Thorac Surg. 2007;83:1879–81. doi: 10.1016/j.athoracsur.2006.11.085. [DOI] [PubMed] [Google Scholar]
- 5.Kearney P, Singh H, Hutter J, Khan S, Lee G, Lucey J. Spontaneous coronary artery dissection: A report of three cases and review of the literature. Postgrad Med J. 1993;69:940–5. doi: 10.1136/pgmj.69.818.940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Alvarez J, Deal CW. Spontaneous dissection of the left main coronary artery: Case report and review of the literature. Aust N Z J Med. 1991;21:891–2. doi: 10.1111/j.1445-5994.1991.tb01417.x. [DOI] [PubMed] [Google Scholar]
- 7.Koul AK, Hollander G, Moskovits N, Frankel R, Herrera L, Shani J. Coronary artery dissection during pregnancy and the postpartum period: Two case reports and review of literature. Catheter Cardiovasc Interv. 2001;52:88–94. doi: 10.1002/1522-726x(200101)52:1<88::aid-ccd1022>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 8.Almeda F, Barkatullah S, Kavinsky CJ. Spontaneous coronary artery dissection. Clin Cardiol. 2004;27:377–80. doi: 10.1002/clc.4960270702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Rensing BJ, Kofflard M, Van den Brand MJ, Foley D. Spontaneous dissection of all three coronary arteries in a 33-week pregnant woman. Catheter Cardiovasc Interv. 1999;48:207–10. doi: 10.1002/(sici)1522-726x(199910)48:2<207::aid-ccd19>3.0.co;2-2. [DOI] [PubMed] [Google Scholar]
- 10.Klutstein MW, Tzivoni D, Bitran D, Mendzelevski B, Ilan M, Almagor Y. Treatment of spontaneous coronary artery dissection: Report of three cases. Catheter Cardiovasc Diagn. 1997;40:372–6. doi: 10.1002/(sici)1097-0304(199704)40:4<372::aid-ccd11>3.0.co;2-p. [DOI] [PubMed] [Google Scholar]
- 11.Pretty HC. Dissecting anneurysm of coronary artery in a woman aged 42; rupture. BMJ. 1931;1:667. [Google Scholar]
- 12.Jorgensen MB, Aharonian V, Mansukhani P, Mahrer PR. Spontaneous coronary artery dissection: A cluster of cases with this rare finding. Am Heart J. 1994;127:1382–7. doi: 10.1016/0002-8703(94)90060-4. [DOI] [PubMed] [Google Scholar]
- 13.Mohamed HA, Eshawesh A, Habib N. Spontaneous coronary dissection. A case and review of the literature. Angiology. 2002;53:205–11. doi: 10.1177/000331970205300212. [DOI] [PubMed] [Google Scholar]
- 14.Capuano C, Sesana M, Predolini S, Leonzi O, Cuccia C. Case report: A very large dissection in the left anterior descending coronary artery of a 56-year-old man. Cardiovasc Revasc Med. 2006;7:240–2. doi: 10.1016/j.carrev.2006.07.003. [DOI] [PubMed] [Google Scholar]
- 15.Kaminemi R, Sadhu A, Alpert J. Spontaneous coronary artery dissection: Report of two cases and a 50-year review of the literature. Cardiol Rev. 2002;10:279–84. doi: 10.1097/00045415-200209000-00004. [DOI] [PubMed] [Google Scholar]
- 16.Arnold JR, West NE, van Gaal WJ, Karamitsos TD, Banning AP. The role of intravascular ultrasound in the management of spontaneous coronary artery dissection. Cardiovasc Ultrasound. 2008;6:24. doi: 10.1186/1476-7120-6-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Maeder M, Ammann P, Angehrn W, Rickli H. Idiopathic spontaneous coronary artery dissection: Incidence, diagnosis and treatment. Int J Cardiol. 2005;101:363–9. doi: 10.1016/j.ijcard.2004.03.045. [DOI] [PubMed] [Google Scholar]
- 18.Appleby CE, Barolet A, Ing D, Ross J, Schwartz L, Seidelin P, et al. Contemporary management of pregnancy-related coronary artery dissection: A single-centre experience and literature review. Exp Clin Cardiol. 2009;14:e8–16. [PMC free article] [PubMed] [Google Scholar]
- 19.Heefner WA. Dissection haematoma of the coronary artery. JAMA. 1973;223:550–1. [PubMed] [Google Scholar]
- 20.Bager AC, Beeuwkes R, Ainey L, Silverman K. Hypothesis: Vasa vasorum and neovascularisation of human coronary arteries. A possible role in the pathophysiology of atherosclerosis. N Engl J Med. 1984;310:175–7. doi: 10.1056/NEJM198401193100307. [DOI] [PubMed] [Google Scholar]
- 21.Robinowitz M, Virmani R, McAllister H. Spontaneous coronary artery dissection and eosinophilic inflammation: A cause and effect relationship. Am J Med. 1982;72:923–8. doi: 10.1016/0002-9343(82)90853-1. [DOI] [PubMed] [Google Scholar]
- 22.Dowling GP, Buja LM. Spontaneous coronary artery dissection occurs with and without peri-adventitial inflammation. Arch Pathol Lab Med. 1987;111:470–2. [PubMed] [Google Scholar]
- 23.Steinhauer JR, Caulfield JB. Spontaneous coronary artery dissection associated with cocaine use: A case report and brief review. Cardiovasc Pathol. 2001;10:141–5. doi: 10.1016/s1054-8807(01)00074-6. [DOI] [PubMed] [Google Scholar]
- 24.Jaffe BD, Broderick TM, Leier CV. Cocaine-induced coronary artery dissection. N Engl J Med. 1994;330:510–1. doi: 10.1056/NEJM199402173300719. [DOI] [PubMed] [Google Scholar]
- 25.Sherrid MV, Mieres J, Mogtader A. Onset during exercise of spontaneous coronary artery dissection and sudden death. Occurrence in a trained athlete: Case report and review of prior cases. Chest. 1995;108:284–7. doi: 10.1378/chest.108.1.284. [DOI] [PubMed] [Google Scholar]
- 26.Ellis CJ, Haywood GA, Monro JL. Spontaneous coronary artery dissection in a young woman resulting from intense gymnasium “work-out”. Int J Cardiol. 1994;47:193–4. doi: 10.1016/0167-5273(94)90191-0. [DOI] [PubMed] [Google Scholar]
- 27.Masuda T, Akiyama H, Kurosawa T, Ohwada T. Long-term follow-up of coronary artery dissection due to blunt chest trauma with spontaneous healing in a young woman. Intensive Care Med. 1996;22:450–2. doi: 10.1007/BF01712164. [DOI] [PubMed] [Google Scholar]
- 28.Borczuk AC, van Hoeven KH, Factor SM. Review and hypothesis: The eosinophil and peripartum heart disease (myocarditis and coronary artery dissection)--coincidence or pathogenetic significance? Cardiovasc Res. 1997;33:527–32. doi: 10.1016/s0008-6363(96)00257-x. [DOI] [PubMed] [Google Scholar]
- 29.Bonacchi M, Prifti E, Giunti G, Frati G, Leacche M, Brancaccio G, et al. Emergency management of spontaneous coronary artery dissection. J Cardiovasc Surg (Torino) 2002;43:189–93. [PubMed] [Google Scholar]
- 30.Martín Dávila F, Delgado Portela M, García Rojo M, González García J, Puig Rullán AM, López Pérez R, et al. Coronary artery dissection in alpha-1-antitrypsin deficiency. Histopathology. 1999;34:376–8. doi: 10.1046/j.1365-2559.1999.0669d.x. [DOI] [PubMed] [Google Scholar]
- 31.Azam MN, Roberts DH, Logan WF. Spontaneous coronary artery dissection associated with oral contraceptive use. Int J Cardiol. 1995;48:195–8. doi: 10.1016/0167-5273(94)02238-e. [DOI] [PubMed] [Google Scholar]
- 32.Tsimikas S, Giordano FJ, Tarazi RY, Beyer RW. Spontaneous coronary artery dissection in patients with renal transplantation. J Invasive Cardiol. 1999;11:316–21. [PubMed] [Google Scholar]
- 33.Marik PE, Marik E. Coronary artery dissection after a rugby injury: A case report. S Afr Med J. 1990;77:586–7. [PubMed] [Google Scholar]
- 34.Saunders SL. Spontaneous coronary artery dissection possibly related to drug hypersensitivity in a male. Gen Physiol Biophys. 1990;9:291–9. [Google Scholar]
- 35.Kaufman G, Engelbrecht JW. Hemorrhagic intramedial dissection of coronary artery with cystic medial necrosis. Am J Med. 1969;24:409–13. doi: 10.1016/0002-9149(69)90437-8. [DOI] [PubMed] [Google Scholar]
- 36.Cocco P, Thiene G, Corrado D, Lodovichetti G, Pennelli N. Ematoma (aneurisma) dissecante spontaneo delle coronarie e morte improvvisa. G Ital Cardiol. 1990;20:795–800. [PubMed] [Google Scholar]
- 37.Van den Branden BJ, Bruggeling WA, Corbeij HM, Dunselman PH. Sponataneous coronary artery dissection in the postpartum period. Neth Heart J. 2008;16:412–4. doi: 10.1007/BF03086188. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Engelman DT, Thayer J, Derossi J, Scheinerman J, Brown L. Pregnancy related coronary artery dissection: A case report and collective review. Conn Med. 1993;57:135–9. [PubMed] [Google Scholar]
- 39.Bulkley BH, Roberts WC. Dissecting aneurysm (hematoma) limited to coronary artery: A clinic-pathologic study of six patients. Am J Med. 1973;55:747–56. doi: 10.1016/0002-9343(73)90255-6. [DOI] [PubMed] [Google Scholar]
- 40.Mark D, Kong Y, whalen R. Variant angina and spontaneous coronary artery dissection. Am J Cardiol. 1985;56:485–6. doi: 10.1016/0002-9149(85)90894-x. [DOI] [PubMed] [Google Scholar]
- 41.Van Der Bel-Khan J. Recurrent primary coronary artery dissecting aneurysm (hematoma) Am J Clin Pathol. 1982;78:394–8. doi: 10.1093/ajcp/78.3.394. [DOI] [PubMed] [Google Scholar]
- 42.Palank E, Dawson J, Cowen G, Tysinger J. Primary dissecting aneurysm of the right coronary artery. Chest. 1977;72:774–6. doi: 10.1378/chest.72.6.774. [DOI] [PubMed] [Google Scholar]
- 43.Barrett JM, Van Hooydonk JE, Boehm FH. Pregnancy-related rupture of arterial aneurysms. Obstet Gynecol Surv. 1982;37:557–66. doi: 10.1097/00006254-198209000-00001. [DOI] [PubMed] [Google Scholar]
- 44.Dhawan R, Singh G, Fesniak H. Spontaneous coronary artery dissection: The clinical spectrum. Angiology. 2002;53:89–92. doi: 10.1177/000331970205300112. [DOI] [PubMed] [Google Scholar]
- 45.Roth A, Elkayam U. Acute myocardial infarction associated with pregnancy. Ann Intern Med. 1996;125:751–62. doi: 10.7326/0003-4819-125-9-199611010-00009. [DOI] [PubMed] [Google Scholar]
- 46.Madu EC, Kosinski DJ, Wilson WR, Burket MW, Fraker TD, Ansel GM. Two vessel coronary artery dissection in the peripartum period. Angiology. 1994;45:809–16. doi: 10.1177/000331979404500909. [DOI] [PubMed] [Google Scholar]
- 47.Mortensen KH, Thuesen L, Kristensen IB, Christiansen EH. Spontaneous coronary artery dissection: A Western Denmark Heart Registry Study. Catheter Cardiovasc Interv. 2009;74:710–7. doi: 10.1002/ccd.22115. [DOI] [PubMed] [Google Scholar]
- 48.Antman EM, Anbe DT, Armstrong PW, Bates ER, Green LA, Hand M, et al. ACC/AHA Guidelines for the management of patients with ST-elevation myocardial infarction: Executive summary. J Am Coll Cardiol. 2004;44:671–719. doi: 10.1016/j.jacc.2004.07.002. [DOI] [PubMed] [Google Scholar]
- 49.Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE, Jr, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-elevation myocardial infarction—Executive summary: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) J Am Coll Cardiol. 2007;50:652–726. [Google Scholar]
- 50.Wilson AM, Boyle AJ, Fox P. Management of ischemic heart disease in women of child-bearing age. Intern Med J. 2004;34:694–7. doi: 10.1111/j.1445-5994.2004.00698.x. [DOI] [PubMed] [Google Scholar]
- 51.Atay Y, Yagdi T, Turkoglu C, Altintig A, Buket S. Sponatneous dissection of the left main coronary artery: A case report and review of the literature. J Card Surg. 1996;11:371–5. doi: 10.1111/j.1540-8191.1996.tb00066.x. [DOI] [PubMed] [Google Scholar]
- 52.Celik SK, Sagcan A, Altintig A, Yuksel M, Akin M, Kultursay H. Primary spontaneous coronary artery dissections in atherosclerotic patients. Eur J Cardiothorac Surg. 2001;20:573–6. doi: 10.1016/s1010-7940(01)00864-8. [DOI] [PubMed] [Google Scholar]
- 53.Versaci F, Tomai F, Gaspardone A, Proietti F, Chiariello L, Gioffrè PA. Stent implantation for spontaneous coronary dissection. Cardiologia. 1997;42:971–4. [PubMed] [Google Scholar]
- 54.Paez M, Buisan F, Herrero E. Spontaneous dissection of the left coronary artery trunk during the postpartum period treated with revascularization surgery, ventricular assistance and a successful heart transplant. Acta Anaesthesiol Scand. 2007;51:960–1. doi: 10.1111/j.1399-6576.2007.01359.x. [DOI] [PubMed] [Google Scholar]
- 55.Lane JE, Cartledge RG, Johnson JH. Successful surgical treatment of spontaneous coronary artery dissection. Curr Surg. 2001;58:316–8. doi: 10.1016/s0149-7944(00)00456-6. [DOI] [PubMed] [Google Scholar]
- 56.Ardehali R, Brinton TJ, Wilson AM, Gradman M, Vagelos RH, Lee DP. Recurrent spontaneous coronary artery dissection with transient left ventricular systolic dysfunction. Int J Cardiol. 2007;116:e48–50. doi: 10.1016/j.ijcard.2006.06.024. [DOI] [PubMed] [Google Scholar]
- 57.Sarmento-Leite R, Machado PR, Garcia SL. Spontaneous coronary artery dissection: Stent it or wait for healing? Heart. 2003;89:164. doi: 10.1136/heart.89.2.164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Shirakawa Y, Matsumiya G, Ohtake S, Sawa Y, Kagisaki K, Matsuda H. Emergency operation for sponataneous coronary artery dissection in young female. Asian Cardiovasc Thorac Ann. 2002;10:58–60. doi: 10.1177/021849230201000115. [DOI] [PubMed] [Google Scholar]
- 59.Cini R, Iezzi F, Sordini P, Pasceri V. Sponataneous left coronary artery dissection. Interact Cardiovasc Thorac Surg. 2008;7:943–4. doi: 10.1510/icvts.2008.182345. [DOI] [PubMed] [Google Scholar]
- 60.Curiel P, Spinelli G, Petrella A, Gori A, De Maria R, Bonacina E, et al. Postpartum coronary artery dissection followed by heart transplantation. Am J Obstet Gynaecol. 1990;163:538–9. doi: 10.1016/0002-9378(90)91192-f. [DOI] [PubMed] [Google Scholar]
- 61.Benham R, Tillinghast S. Thrombolytic therapy in spontaneous coronary artery dissection. Clin cardiol. 1991;14:611–4. doi: 10.1002/clc.4960140714. [DOI] [PubMed] [Google Scholar]
- 62.Vogiatzis I, Hadjimiltiades S, Sachpekidis V, Parcharidis G. Spontaneous coronary artery dissection and acute myocardial infarction during pregnancy. Hellenic J Cardiol. 2010;51:74–80. [PubMed] [Google Scholar]
- 63.Teniente-Valente R, Delgado-Sánchez A, Sánchez M, Mendoza-Gómez R, Vargas L, Medina-Torres O, et al. Inferior acute myocardial infarction associated to coronary artery dissection in the postpartum. Int J Cardiol. 2009;7:2. [Google Scholar]
- 64.Chue CD, Routledge HC, Townend JN. Spontaneous coronary artery dissection and the role of percutaneous coronary intervention: To treat or not to treat? J Invasive Cardiol. 2009;21:E44–7. [PubMed] [Google Scholar]
- 65.Rahman S, Abdul-Waheed M, Helmy T, Huffman LC, Koshal V, Guitron J, et al. Spontaneous left main coronary artery dissection complicated by pseudoaneurysm formation in pregnancy: Role of CT coronary angiography. J Cardiothorac Surg. 2009;4:15. doi: 10.1186/1749-8090-4-15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Al-Mohaissen MA. Spontaneous left main coronary artery dissection. A rare cause of acute coronary syndrome. Saudi Med J. 2009;30:1476–9. [PubMed] [Google Scholar]
- 67.Azzarelli S, Fiscella D, Amico F, Giacoppo M, Argentino V, Fiscella A. Multivessel spontaneous coronary artery dissection in a postpartum woman treated with multiple drug-eluting stents. J Cardiovasc Med (Hagerstown) 2009;10:340–3. doi: 10.2459/JCM.0b013e3283276dee. [DOI] [PubMed] [Google Scholar]
- 68.Shahabi S, Smith NA, Chanana C, Abbott JD, Copel J, Setaro JF. Pregnancy-associated myocardial infarction: A report of two cases and review of the literature. Ups J Med Sci. 2008;113:325–30. doi: 10.3109/2000-1967-239. [DOI] [PubMed] [Google Scholar]
- 69.Iltumur K, Karahan Z, Ozmen S, Danis R, Toprak N. Spontaneous coronary artery dissection during hemodialysis in the post-abortion period. Int J Cardiol. 2008;127:e45–7. doi: 10.1016/j.ijcard.2007.01.105. [DOI] [PubMed] [Google Scholar]
- 70.Halmai L, Sepp R, Thury A, Gavallér H, Ungi I, Rudas L. Coronary artery dissection in the postpartum period--A case study. Orv Hetil. 2008;149:457–63. doi: 10.1556/OH.2008.28012. [DOI] [PubMed] [Google Scholar]
- 71.Satoda M, Takagi K, Uesugi M, Morishima I, Mukawa H, Tsuboi H, et al. Acute myocardial infarction caused by spontaneous postpartum coronary artery dissection. Nat Clin Pract Cardiovasc Med. 2007;4:688–92. doi: 10.1038/ncpcardio1055. [DOI] [PubMed] [Google Scholar]
- 72.Kalra N, Greenblatt J, Ahmed S. Postpartum spontaneous coronary artery dissection (SCAD) managed conservatively. Int J Cardiol. 2008;129:e53–5. doi: 10.1016/j.ijcard.2007.06.118. [DOI] [PubMed] [Google Scholar]
- 73.Sherif HM, Nguyen HC, Sarter BH, West JT, Lucente E, Fink DM, et al. Spontaneous coronary dissection in late pregnancy: A multidisciplinary approach to management. Ann Thorac Surg. 2008;85:1793–4. doi: 10.1016/j.athoracsur.2007.11.018. [DOI] [PubMed] [Google Scholar]
- 74.Goland S, Schwarz ER, Siegel RJ, Czer LS. Pregnancy-associated spontaneous coronary artery dissection. Am J Obstet Gynecol. 2007;197:e11–3. doi: 10.1016/j.ajog.2007.08.054. [DOI] [PubMed] [Google Scholar]
- 75.Schiff JH, Gries A, Ehehalt R, Elsaesser M, Katus HA, Meyer FJ. A pregnant woman with acute myocardial infarction due to coronary artery dissection: Pre-hospital and in-hospital management. Resuscitation. 2007;73:467–74. doi: 10.1016/j.resuscitation.2006.10.020. [DOI] [PubMed] [Google Scholar]
- 76.Kiernan TJ, Rochford M. Postpartum spontaneous coronary artery dissection: An important clinical link with anticardiolipin antibody. Int J Cardiol. 2007;114:E75–6. doi: 10.1016/j.ijcard.2006.07.113. [DOI] [PubMed] [Google Scholar]
- 77.Frey BW, Grant RJ. Pregnancy-associated coronary artery dissection: A case report. J Emerg Med. 2006;30:307–10. doi: 10.1016/j.jemermed.2005.05.027. [DOI] [PubMed] [Google Scholar]
- 78.Luceri S, Paolillo V, De Benedictis M, Scrocca I. Spontaneous dissection of the left coronary tree after an interruption of pregnancy treated with extensive stenting. J Invasive Cardiol. 2006;18:e117–20. [PubMed] [Google Scholar]
- 79.Gasparovic H, Ugljen R, Coric V, Gosev I, Gasparovic V, Jelic I. Surgical treatment of a postpartal spontaneous left main coronary artery dissection. Thorac Cardiovasc Surg. 2006;54:70–1. doi: 10.1055/s-2005-865830. [DOI] [PubMed] [Google Scholar]
- 80.Allagui E, Delmotte P, Joly E, Vachiery JL, Preumont N, Renard M. Spontaneous coronary artery dissection on the 10th post-partum day: A case report. Arch Mal Coeur Vaiss. 2006;99:255–8. [PubMed] [Google Scholar]
- 81.Schroder C, Stoler RC, Branning GB, Choi JW. Postpartum multivessel spontaneous coronary artery dissection confirmed by coronary CT angiography. Proc (Bayl Univ Med Cent) 2006;19:338–41. doi: 10.1080/08998280.2006.11928196. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 82.Rogers IS, Rinaldi MJ, Humphrey CB, Boden WE, Dougherty JE. Postpartum dissection of the left main coronary artery. Clin Cardiol. 2006;29:175–8. doi: 10.1002/clc.4960290410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Chabrot P, Motreff P, Boyer L. Postpartum spontaneous coronary artery dissection: A case of pseudoaneurysm evolution detected on MDCT. AJR Am J Roentgenol. 2006;187:W660. doi: 10.2214/AJR.06.0783. [DOI] [PubMed] [Google Scholar]
- 84.Phillips LM, Makaryus AN, Beldner S, Spatz A, Smith-Levitin M, Marchant D. Coronary artery dissection during pregnancy treated with medical therapy. Cardiol Rev. 2006;14:155–7. doi: 10.1097/01.crd.0000173944.99498.84. [DOI] [PubMed] [Google Scholar]
- 85.Hammond AS, Bailey PL. Acute spontaneous coronary artery dissection in the peripartum period. J Cardiothorac Vasc Anesth. 2006;20:837–41. doi: 10.1053/j.jvca.2005.07.021. [DOI] [PubMed] [Google Scholar]
- 86.Bravio I, Castelão N, Duarte R, Telles R, Roquette J. Post-partum spontaneous coronary artery dissection. Clinical report. Rev Port Cir Cardiotorac Vasc. 2005;12:153–6. [PubMed] [Google Scholar]
- 87.Nallamothu BK, Saint M, Saint S, Mukherjee D. Double jeopardy. N Engl J Med. 2005;353:75–80. doi: 10.1056/NEJMcps050117. [DOI] [PubMed] [Google Scholar]
- 88.Terrovitis JV, Kanakakis J, Nanas JN. Spontaneous coronary artery dissection as a cause of acute myocardial infarction in the postpartum period. Cardiol Rev. 2005;13:211–3. doi: 10.1097/01.crd.0000134862.82534.b3. [DOI] [PubMed] [Google Scholar]
- 89.Juszczyk M, Marnejon T, Hoffman DA. Spontaneous coronary artery dissection postpartum. J Invasive Cardiol. 2004;16:524–6. [PubMed] [Google Scholar]
- 90.Krishnamurthy M, Desai R, Patel H. Spontaneous coronary artery dissection in the postpartum period: Association with antiphospholipid antibody. Heart. 2004;90:e53. doi: 10.1136/hrt.2004.038869. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Jaigobin C, Silver FL. Stroke secondary to post-partum coronary artery dissection. Can J Neurol Sci. 2003;30:168–70. [PubMed] [Google Scholar]
- 92.Shah P, Dzavik V, Cusimano RJ, Sermer M, Okun N, Ross J. Spontaneous dissection of the left main coronary artery. Can J Cardiol. 2004;20:815–8. [PubMed] [Google Scholar]
- 93.McKechnie RS, Patel D, Eitzman DT, Rajagopalan S, Murthy TH. Spontaneous coronary artery dissection in a pregnant woman. Obstet Gynecol. 2001;98:899–902. doi: 10.1016/s0029-7844(01)01563-0. [DOI] [PubMed] [Google Scholar]
- 94.Lerakis S, Manoukian S, Martin RP. Transesophageal echo detection of postpartum coronary artery dissection. J Am Soc Echocardiogr. 2001;14:1132–3. doi: 10.1067/mje.2001.115654. [DOI] [PubMed] [Google Scholar]
- 95.Eby CS, McBride LR. Postpartum coronary artery dissection complicated by heparin-induced thrombocytopenia and thrombosis. Ann Thorac Surg. 2001;71:1025–7. doi: 10.1016/s0003-4975(00)02438-3. [DOI] [PubMed] [Google Scholar]
- 96.Togni M, Amann FW, Follath F. Spontaneous multivessel coronary artery dissection in a pregnant woman treated successfully with stent implantation. Am J Med. 1999;107:407–8. doi: 10.1016/s0002-9343(99)00177-1. [DOI] [PubMed] [Google Scholar]
- 97.Elming H, Køber L. Spontaneous coronary artery dissection. Case report and literature review. Scand Cardiovasc J. 1999;33:175–9. doi: 10.1080/14017439950141821. [DOI] [PubMed] [Google Scholar]
- 98.Samuels LE, Kaufman MS, Morris RJ, Brockman SK. Postpartum coronary artery dissection: Emergency coronary artery bypass with ventricular assist device support. Coron Artery Dis. 1998;9:457–60. [PubMed] [Google Scholar]
- 99.Vilke GM, Mahoney G, Chan TC. Postpartum coronary artery dissection. Ann Emerg Med. 1998;32:260–2. doi: 10.1016/s0196-0644(98)70147-7. [DOI] [PubMed] [Google Scholar]
- 100.Porras MC, Ares MA, Gill JZ. Intracoronary stenting for postpartum coronary artery dissection. Ann Intern Med. 1998;128:873. doi: 10.7326/0003-4819-128-10-199805150-00020. [DOI] [PubMed] [Google Scholar]
- 101.Koller PT, Cliffe CM, Ridley DJ. Immunosuppressive therapy for peripartum-type spontaneous coronary artery dissection: Case report and review. Clin Cardiol. 1998;21:40–6. doi: 10.1002/clc.4960210108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Bucciarelli E, Fratini D, Gilardi G, Affronti G. Spontaneous dissecting aneurysm of coronary artery in a pregnant woman at term. Pathol Res Pract. 1998;194:137–9. doi: 10.1016/S0344-0338(98)80081-2. [DOI] [PubMed] [Google Scholar]
- 103.Alcalá López J, Romero Hinojosa JA, González-Gay JM, Díaz Fernández JF, Melgares Moreno R, Ramírez Hernández JA, et al. Spontaneous postpartum coronary dissection. Rev Esp Cardiol. 1998;51:844–6. doi: 10.1016/s0300-8932(98)74829-8. [DOI] [PubMed] [Google Scholar]
- 104.Almahmeed WA, Haykowski M, Boone J, Ling H, Allard M, Webb J, et al. Spontaneous coronary artery dissection in young women. Catheter Cardiovasc Diagn. 1996;37:201–5. doi: 10.1002/(SICI)1097-0304(199602)37:2<201::AID-CCD21>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- 105.Zampieri P, Aggio S, Roncon L, Rinuncini M, Canova C, Zanazzi G, et al. Follow up after spontaneous coronary artery dissection: A report of five cases. Heart. 1996;75:206–9. doi: 10.1136/hrt.75.2.206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Silberman S, Fink D, Berko RS, Mendzelevski B, Bitran D. Coronary artery bypass surgery during pregnancy. Eur J Cardiothorac Surg. 1996;10:925–6. doi: 10.1016/s1010-7940(96)80325-3. [DOI] [PubMed] [Google Scholar]
- 107.Manari A, Giacometti P, Vergoni W, Mastrangeli S, Guiducci U. Acute myocardial infarction in pregnancy in a patient with pseudoaneurysm of the left main coronary artery. G Ital Cardiol. 1996;26:1437–43. [PubMed] [Google Scholar]
- 108.Coulson CC, Kuller JA, Bowes WA., Jr Myocardial infarction and coronary artery dissection in pregnancy. Am J Perinatol. 1995;12:328–30. doi: 10.1055/s-2007-994487. [DOI] [PubMed] [Google Scholar]
- 109.Bateman AC, Gallagher PJ, Vincenti AC. Sudden death from coronary artery dissection. J Clin Pathol. 1995;48:781–4. doi: 10.1136/jcp.48.8.781. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Mansur LI, Minns GO, Steckley RA. Postpartum myocardial infarction: Association with primary coronary artery dissection. Cleve Clin J Med. 1995;62:261–8. doi: 10.3949/ccjm.62.4.261. [DOI] [PubMed] [Google Scholar]
- 111.Efstratiou A, Singh B. Combined spontaneous postpartum coronary artery dissection and pulmonary embolism with survival. Catheter Cardiovasc Diagn. 1994;31:29–33. doi: 10.1002/ccd.1810310107. [DOI] [PubMed] [Google Scholar]
- 112.Mather PJ, Hansen CL, Goldman B, Inniss S, Piña I, Norris R, et al. Postpartum multivessel coronary dissection. J Heart Lung Transplant. 1994;13:533–7. [PubMed] [Google Scholar]
- 113.Verkaaik AP, Viser W, Deckers JW, Lotgering FK. Multiple coronary artery dissections in a woman. Br J Anaesth. 1993;71:301–2. doi: 10.1093/bja/71.2.301. [DOI] [PubMed] [Google Scholar]
- 114.Emori T, Goto Y, Maeda T, Chiba Y, Haze K. Multiple coronary artery dissections diagnosed in vivo in a pregnant woman. Chest. 1993;104:289–90. doi: 10.1378/chest.104.1.289. [DOI] [PubMed] [Google Scholar]
- 115.Michaux L, Lefebvre C, Lebaupin C, Lo Presti L, Coche E. Spontaneous dissection of the anterior interventricular coronary artery in the postpartum period. Rev Med Interne. 1993;14:49–50. doi: 10.1016/s0248-8663(05)82524-x. [DOI] [PubMed] [Google Scholar]
- 116.Corrado D, Thiene G, Cocco P, Frescura C. Non-atherosclerotic coronary artery disease and sudden death in the young. Br Heart J. 1992;68:601–7. doi: 10.1136/hrt.68.12.601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Bertrand E, Seka R, Adoh M, Dori RN, Odi-Assamoi M, Cailleau G, et al. Spontaneous coronary artery dissection: Apropos of a case with associated spasm and regression of the dissection. Arch Mal Coeur Vaiss. 1993;86:249–53. [PubMed] [Google Scholar]
- 118.Hayden J, Mort T, Rintel T. Acute coronary artery dissection during pregnancy. Int J Obstet Anesth. 1991;1:43–5. doi: 10.1016/0959-289x(91)90031-k. [DOI] [PubMed] [Google Scholar]
- 119.Pardo J, González B, Novoa O, Pumarino R, Oppliger E, Godoy D. Acute post-partum infarct of the myocardium secondary to a spontaneous dissection of the coronary artery. Rev Med Chil. 1990;118:300–5. [PubMed] [Google Scholar]
- 120.Gonzalez JI, Hill JA, Conti CR. Spontaneous coronary artery dissection treated with percutaneous transluminal angioplasty. Am J Cardiol. 1989;63:885–6. doi: 10.1016/0002-9149(89)90068-4. [DOI] [PubMed] [Google Scholar]
- 121.Lette J, Gagnon A, Cerino M, Prénovault J. Apical hypertrophic cardiomyopathy with spontaneous postpartum coronary artery dissection. Can J Cardiol. 1989;5:311–4. [PubMed] [Google Scholar]
- 122.Movsesian MA, Wray RB. Postpartum myocardial infarction. Br Heart J. 1989;62:154–6. doi: 10.1136/hrt.62.2.154. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Nishikawa H, Nakanishi S, Nishiyama S, Nishimura S, Kato K, Yanagishita Y, et al. Primary coronary artery dissection: Its incidence, mode of the onset and prognostic evaluation. J Cardiol. 1988;18:307–17. [PubMed] [Google Scholar]
- 124.Sage MD, Koelmeyer TD, Smeeton WM. Fatal postpartum coronary artery dissection. A light- and electron-microscope study. Am J Forensic Med Pathol. 1986;7:107–11. doi: 10.1097/00000433-198607020-00005. [DOI] [PubMed] [Google Scholar]
- 125.Bonnet J, Aumailley M, Thomas D, Grosgogeat Y, Broustet JP, Bricaud H. Spontaneous coronary artery dissection: Case report and evidence for a defect in collagen metabolism. Eur Heart J. 1986;7:904–9. doi: 10.1093/oxfordjournals.eurheartj.a061979. [DOI] [PubMed] [Google Scholar]
- 126.Vicari R, Eybel C, Monson D. Survival following spontaneous coronary artery dissection: Surgical repair by extrusion of intramural hematoma. Am Heart J. 1986;111:593–4. doi: 10.1016/0002-8703(86)90069-4. [DOI] [PubMed] [Google Scholar]
- 127.Hankins GD, Wendel GD, Leveno KJ, Stoneham J. Myocardial infarction during pregnancy. Obstet Gynecol. 1985;65:139–46. [PubMed] [Google Scholar]
- 128.Johnson KM, Carpenter Pl, Geakle T, Barlow JF. Twenty seven year old postpartum Gravid 4 Para 4 with hypertension and chest pain. S D J Med. 1984;37:17–22. [PubMed] [Google Scholar]
- 129.Chokron R, Thomas D, Leprince JL, Szwarc G, Gandjbakhch I, Grosgogeat Y. Isolated primary dissection of coronary arteries. Apropos of 3 cases with a favorable development. Arch Mal Coeur Vaiss. 1983;76:886–92. [PubMed] [Google Scholar]
- 130.Ehya H, Jackson M, Weitzner S. Postpartum dissecting aneurysm of coronary arteries in a patient with sarcoidosis. South Med J. 1980;73:87–8. doi: 10.1097/00007611-198001000-00032. [DOI] [PubMed] [Google Scholar]
- 131.Pisano RV, Taylor MB, Sopher IM. Dissecting coronary artery aneurysm: A report of two cases. J Forensic Sci. 1979;24:18–25. [PubMed] [Google Scholar]
- 132.Jewett JF. Two dissecting coronary artery aneurysms postpartum. N Engl J Med. 1978;298:1255–7. doi: 10.1056/NEJM197806012982211. [DOI] [PubMed] [Google Scholar]
- 133.Shaver PJ, Carrig TF, Baker WP. Postpartum coronary artery dissection. Br Heart J. 1978;40:83–6. doi: 10.1136/hrt.40.1.83. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 134.Asuncion CM, Hyun J. Dissecting intramural hematoma of the coronary artery in pregnancy and the puerperium. Obstet Gynecol. 1972;40:202–10. [PubMed] [Google Scholar]
- 135.Cloudon DG, Cloudon DB, Edwards JE. Primary dissecting aneurysm of coronary artery: A cause of acute myocardial ischemia. Circulation. 1972;45:256–9. doi: 10.1161/01.cir.45.2.259. [DOI] [PubMed] [Google Scholar]
- 136.Di Maio VJ, Di Maio DJ. Postpartum dissecting coronary aneurysm. N Y State J Med. 1971;71:767–9. [PubMed] [Google Scholar]
- 137.Palomino SJ. Dissecting intramural hematoma of the left coronary artery in the puerperium: A case report and survey of literature. Am J Clin Pathol. 1968;51:119–25. doi: 10.1093/ajcp/51.1.119. [DOI] [PubMed] [Google Scholar]
- 138.Brody GL, Burton JF, Zawadzki ES, French JA. Dissecting aneurysms of the coronary artery. N Engl J Med. 1965;273:1–6. doi: 10.1056/NEJM196507012730101. [DOI] [PubMed] [Google Scholar]
- 139.Burton JF, Zawadzki ES. The coronary aneurysm. J Forensic Sci. 1962;7:486–92. [Google Scholar]
- 140.Wells AL. Dissecting aneurysm of coronary artery in the puerperium. J Pathol Bact. 1960;79:404–5. doi: 10.1002/path.1700790222. [DOI] [PubMed] [Google Scholar]
- 141.Boschetti AE, Levine A. Cystic medionecrosis with dissecting aneurysm of coronary arteries. Arch Intern Med. 1958;102:562–70. doi: 10.1001/archinte.1958.00260210048008. [DOI] [PubMed] [Google Scholar]
- 142.Lovitt WV, Corzine WJ. Dissecting intramural hemorrhage of anterior descending branch of left coronary artery. Am Arch Pathol. 1952;54:458–62. [PubMed] [Google Scholar]