

Abstract
Aim:
The aim of this study was to determine the prevalence of dens invaginatus in a sample of Turkish dental patients.
Materials and Methods:
The sample included 6, 912 panoramic radiographs from different Turkish dental patients. The ages of the patients ranged from 18 to 50 years. A tooth was considered having dens invaginatus if an infolding of a radiopaque ribbon-like structure equal in density to enamel was seen extending from the cingulum into the root canal. Maxillary and mandibular teeth were evaluated on panoramic radiographs to determine the type of dens invaginatus using Oehlers’ classification.
Results:
The overall incidence of patients with dens invaginatus was 0.17%. Dens invaginatus were detected in 15 teeth of a total of 192 150 teeth to give a tooth prevalence of 0.008%. Maxillary lateral incisors were most commonly affected teeth in the mouth (80% of cases), followed by maxillary canine teeth (20% of cases). The bilateral incidence of a symmetrical distribution was 25%.
Conclusion:
The occurrence of dens invaginatus among this Turkish population was rare. Attention should be paid to the presence of dens invaginatus and the treatment problems associated with it.
Keywords: Dens invaginatus, prevalence, Turkish
INTRODUCTION
Dens invaginatus is a developmental malformation resulting from an invagination of enamel organ into the dental papilla, beginning at the crown and sometimes extending into the root before calcification occurs.[1–3] There are number of terms to describe dens invaginatus like Dens in Dente,[4] dilated composite odontoma,[5] dents telescope, and gestant anomaly.[6] According to A. Alanic and K. Bishop, the term “Dens invaginatus” is more appropriate as it reflects the infolding of the outer portion enamel into the inner dentine portion with the formation of a pocket or dead space.[7]
Several theories have illustrated the etiology of dens invaginatus; however, at the present time, they remain unclear. Kronfeld suggested that the invagination results from a focal failure of growth of the internal enamel epithelium while the surrounding normal epithelium continues to proliferate and engulfs the static area.[8] According to Pindborg, the etiology of this malformation is unknown; yet, the following explanations have been proposed: (i) delayed focal growth, (ii) stimulation in the area of the tooth bud, and (iii) abnormal pressure on tissues surrounding the dental organ.[9,10]
Clinically, dens invaginatus appears in the tooth crown at the site of an anatomical lingual pit susceptible to caries.[11] Radiographically, it shows a radiopaque invagination, equal in density to enamel, extending from the cingulum into the root canal.[2] The invagination allows entry of irritants into an area which is separated from pulp tissue by only a thin layer of enamel and dentine. It may predispose to the development of dental caries and ingress of irritants resulting in pulp inflammation. The affected pulp tissue then frequently undergoes necrosis.[12]
According to Oehlers,[13] dens invaginatus can be classified into three categories depending on enamel invagination depth inside the tooth. In Type I, the invagination ends as a blind sac and is limited to the coronary portion of the tooth. In Type II, the invagination extends beyond the cementoenamel junction and is retained inside the main canal. Type III occurs when the invagination extends throughout the root canal interior and reaches the apical tooth area, giving rise to two or more foramina.[14]
The dens invaginatus may be associated with other tooth abnormalities, such as microdontia,[15] macrodontia,[16] taurodontism,[17–19] gemination and fusion,[20,21] and amelogenesis imperfecta.[3]
Studies that have addressed the prevalence of dens invaginatus in populations are very few and most of them are case reports. The reported incidence of dens invaginatus ranges from 0.04% to 10%.[3] Teeth in both maxillary and mandibular arches may be affected, but the permanent maxillary lateral incisors are the most commonly involved teeth.[22–25]
The purpose of this study was to investigate the prevalence of dens invaginatus in a sample of Turkish dental patients and their distribution among different types of teeth.
MATERIALS AND METHODS
Panoramic radiographs from 8,568 patients (4,324 women and 4,243 men, age range from 15 to 50 years) attending Kırıkkale University Dental Faculty Hospital during the period from July 2009 to August 2011 were reviewed for the presence of dens invaginatus. Radiographic interpretation was undertaken by two experienced examiners.
A patient was excluded if he/she was below 15 years of age and if the orthopantomograms were not of high quality and/or failed to show crowns of the teeth. In addition, carious, restored, and fractured teeth, incomplete apical foramen formation, undetectable furcation, and fused roots were not included. The final sample included 6,912 patients (3,860 women and 3,052 men, mean patient age: 29.04 years and the range between 15 to 50 years).
A tooth was considered as having dens invaginatus if an infolding of a radiopaque ribbon-like structure equal in density to enamel was seen extending from the cingulum into the root canal. Each radiograph which exhibits this criterion was re-examined carefully by both examiners twice and a combined decision was made to either consider the tooth has having dens invaginatus or not. For each patient with dens invaginatus, we recorded the demographic variables (including age, sex), number, and location (maxilla or mandible). Maxillary and mandibular teeth were evaluated on panoramic radiographs to determine the type of dens invaginatus using Oehlers’ classification.[13]
The examiners read 100 radiographs separately, containing 10 diff erent cases of dens invaginatus as part of the training before the start of the investigation. The examiners re-read together a sample of 12 panoramic radiographs containing dens invaginatus 2 weeks after the initial training and a 100% agreement was obtained. The overall incidence of dens invaginatus in the patients and their correlations between female and male patients and between the right-side and left-side occurrences were analyzed by using the χ2 test. The bilateral incidences of dens invaginatus were also evaluated.
RESULTS
Panoramic radiographs of 6,912 patients, 3,860 females and 3,052 males, with ages between 15 - 45 years and average age of 29.04 ± 8.68 years were studied.
Almost equal numbers of maxillary (95,994) and mandibular teeth (96,156) were examined. The number of individual tooth type was comparable, so the per tooth prevalence of dens invaginatus was meaningful. Dens invaginatus were detected in 15 teeth of a total of 192,150 teeth to give a tooth prevalence of 0.008%. The prevalence of dens invaginatus among different tooth types is presented in Table 1. All 15 teeth exhibiting dens invaginatus were in the maxillary arch, so the maxillary teeth prevalence was 0.016%. Maxillary lateral incisors were most commonly affected teeth in the mouth (80% of cases), followed by maxillary canines (20% of cases). No dens invaginatus were detected in any other tooth types.
Table 1.
Frequency of the prevalence of dens invaginatus amongst different tooth types in the sample set of dental patients
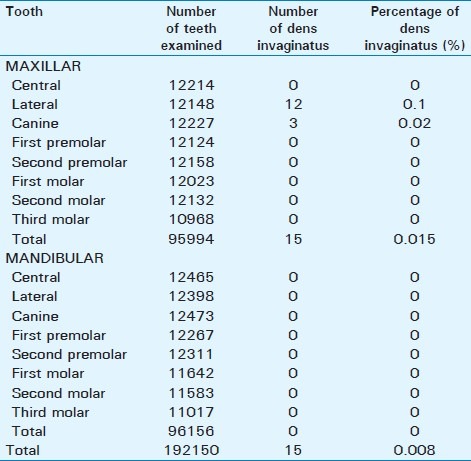
Table 2 presents the distribution and prevalence of dens invaginatus according to the gender of patients. Males had more teeth with dens invaginatus (12 teeth) than females (3 teeth). The prevalence of dens invaginatus for males and females was 0.29% and 0.008%, respectively. The difference calculated using chi square test was statically significant (P = 0.00).
Table 2.
The distribution of the subjects with dens invaginatus
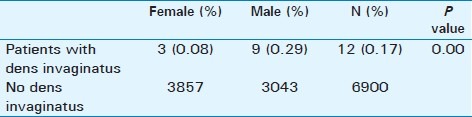
The distribution of patients with dens invaginatus is presented in Table 3. Teeth with dens invaginatus were found in 12 subjects (9 males, 3 females) of 6 912 subjects examined; thus, the person prevalence was 0.17%. Bilateral dens invaginatus were seen in three patients (25%), whereas nine patients (75%) of those with dens invaginatus exhibited unilateral dens invaginatus.
Table 3.
Number of teeth with dens invaginatus according to gender

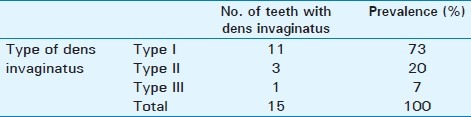
The most commonly seen type of dens invaginatus was Type I (73%) followed by Type II (20%) while 7% of patients had Type III dens invaginatus [Table 4].
Table 4.
Number of dens invaginatus according to type
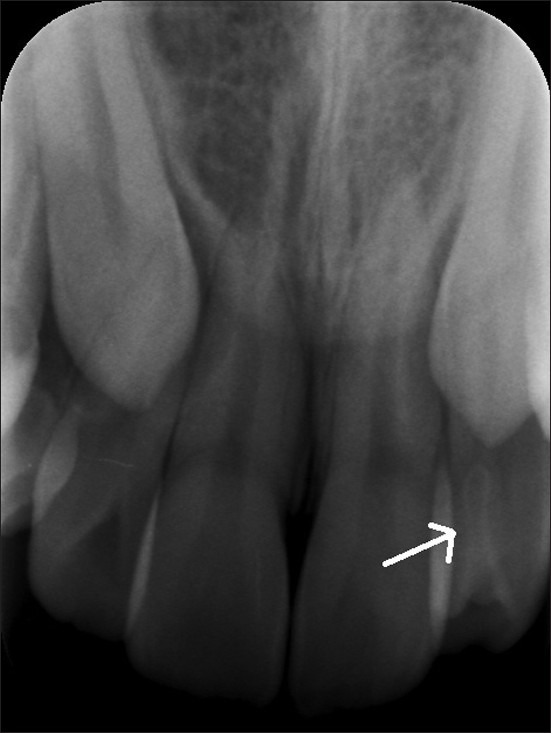
Figures 1 to 4 show examples of dens invaginatus belonging in different types of teeth as seen in periapical and panoramic radiographic images.
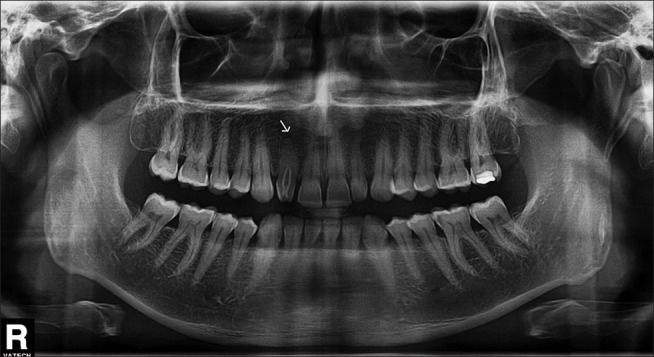
Figure 1.

Panoramic radiograph shows dens invaginatus in maxillary right lateral incisor without any signs of pathosis (white arrow).
Figure 4.
Periapical radiograph shows Type I dens invaginatus in the maxillary left lateral incisors (white arrow).
Figure 2.
Panoramic radiograph of the right lateral incisor reveals an invagination extending from the crown to the middle of the root (Type II). Note the periapical radiolucency (white arrow).
Figure 3.

Panoramic radiograph shows Type III dens invaginatus in the maxillary right lateral incisors. The invagination extends all the way from the crown to the apex of the root.
DISCUSSION
Dens invaginatus is a developmental anomaly, which arises as a result of an invagination of enamel organ through dental papilla, in the early phase of odontogenesis, before calcification occurs.[3]
Review of the literature reveals a wide discrepancy in the prevalence of dens invaginatus in different populations. The results of the present study on a group of Turkish dental patients have shown an overall prevalence of 2.95% for individuals and 0.65% for all teeth examined. Hamasha and Alomari[15] found a prevalence of 0.65% for individuals and 43.2% for all teeth in Jordanian dental patients. On the basis of person prevalence, the results of Cakici et al.[26] and Kirzioğlu and Ceylan[27] were 1.3% and 12%, respectively, in Turkish dental patients.
When considering only anterior teeth, the prevalence of dens invaginatus was 0.02%. This figure is considerably lower than the result of the study by Cakıcı et al.[26] (0.8%) and by Kirzioğlu and Ceylan[27] (0.8%) among the Turkish population, and the result of the study by Ezoddini et al., (5.8%) among Iranian population, and the study by Poyton and Morgan.[28] These variations in prevalence between different populations may be due to ethnic variations, but may also be influenced by differences in criteria used for interpretation of dens invaginatus and also the specific teeth examined.
In the present study, males presented a higher prevalence of dens invaginatus than females and these differences were statistically significant (P = 0.00). This finding is consistent with another study previously reported for patients of Jordanian origin.[15] However, according to other studies performed in Turkish population, dens invaginatus occurred equally frequent in males and females.[26,27]
In the present study, the maxillary lateral incisors were the most commonly affected teeth with the condition, followed by the canines. Additionally, no dens invaginatus were observed in the mandibular anterior teeth, and maxillary central incisors examined. These findings were consistent with studies of Cakıcı et al.[26] Hamasha and Alomari,[15] Kirzioğlu and Ceyhan.[27]
The appearance of the symmetric dens invaginatus was considered to be a common finding by some authors. In the present study, the bilateral occurrence of dens invaginatus was 25% (3 of 15), which was very close to the recent study[26] among the Turkish population (23.1%) and the studies on the Jordanian population[15] (24.49%). These contradictory variations might be explained by marked differences in the sample size, case selection, and the methods used. Thus, further investigations are necessary to clarify the issue.
The most popular classification of invagination has been proposed by Oehlers.[13] Type I is an enamel-lined minor invagination occurring within the confines of the crown and not extending beyond the amelocemental junction. Type II consists of an enamel-lined form which invades the root but ends as a blind sac with or without communication with the pulp. Type III describes an invagination penetrating the root to the apical area and forming a second foramen in the apical or periodontal area. In the present study, the most commonly seen type of dens invaginatus was type I (73%) followed by type II (20%) while 7% of patients had type III dens invaginatus. These findings were consistent with previously published studies.[15,26,27] Oehlers’ system is based on a two-dimensional radiographic image and there are limitations associated with the use of conventional radiography in the classification, true extent, and complexity of the invagination.[27] With respect to the above data, it was considered that a tooth which appeared to be Type II dens invaginatus radiographically might have been Type III dens invaginatus histologically.
The limitations in this study included the method of radiographic assessment which included only panoramic radiographs, did not give a clear picture of the posterior teeth with dens invaginatus. Moreover, compared to panoramic radiographs, periapical radiographs are normally accurate images of the object without major distortion or magnification especially in the anterior region. However, panoramic radiographs show the entire mouth area - all teeth on both upper and lower jaws - on a single X-ray.
The treatment options for invaginated teeth include preventive sealing or filling of the invagination, root canal treatment, endodontic apical surgery, intentional replantation, and extraction.[29,30] Because of the complex anatomy of dens invaginatus, conservative endodontic treatment is difficult and usually complicated, especially when large apical lesions exist. Regardless of the size of the periradicular lesion, surgical treatment should be performed only when nonsurgical endodontic treatment has failed, and the size of the periradicular lesion should not dictate the treatment procedure.[31,32]
Endodontic treatment of invaginated teeth requires careful analysis of the configuration of the root canal system. The root canal morphology of these teeth can be very complex and in many cases, it is difficult to detect and differentiate between the main and the invaginated canals.[3,33]
Finally, due to the relatively small size sample, the prevalence figures for dens invaginatus in the present study should be considered with caution as they may not be a representative for the overall Turkish population. Further large-scale multicenter studies are therefore needed to assess its prevalence in the general population.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
Available FREE in open access from: http://www.clinicalimagingscience.org/text.asp?2012/2/1/34/97755
REFERENCES
- 1.Alani A, Bishop K. Dens invaginatus. Part 1: classification, prevalence and aetiology. Int Endod J. 2008;41:1123–36. doi: 10.1111/j.1365-2591.2008.01468.x. [DOI] [PubMed] [Google Scholar]
- 2.Zengin AZ, Sumer AP, Celenk P. Double dens invaginatus: report of three cases. Eur J Dent. 2009;3:67–70. [PMC free article] [PubMed] [Google Scholar]
- 3.Hulsmann M. Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J. 1997;30:79–90. doi: 10.1046/j.1365-2591.1997.00065.x. [DOI] [PubMed] [Google Scholar]
- 4.Busch F. tber Verschmelzung und Verwachsung der ZAhne des Milchgebisses und des bleibenden Gebisses. Deut Monot f Zhk. 1897;15:469. [Google Scholar]
- 5.Hunter HA. Dilated composite odontome; reports of two cases, one bilateral and one radicular. Oral Surg Oral Med Oral Pathol. 1951;4:668–73. doi: 10.1016/0030-4220(51)90060-6. [DOI] [PubMed] [Google Scholar]
- 6.Colby RA. Philadelphia, Montreal: J. B. Lippincott Co; 1956. Color Atlas of Oral Pathology. [Google Scholar]
- 7.Dixit PB. Dens Invaginatus : Diagnosis and its treatment options. Journal of Nepal Dental Association. 2010;11:82–4. [Google Scholar]
- 8.Kronfeld R. Dens in dente. J Dent Res. 1934;14:49–66. [Google Scholar]
- 9.Pindborg JJ. 4 ed. Philadelphia: Saunders; 1970. Pathology of the dental hard tissues. [Google Scholar]
- 10.Moradi S, Donyavi Z, Esmaealzade M. Non-surgical root canal treatment of dens invaginatus 3 in a maxillary lateral incisor. Iranian Endodontic Journal. 2008;3:38–41. [PMC free article] [PubMed] [Google Scholar]
- 11.Vajrabhaya L. Nonsurgical endodontic treatment of a tooth with double dens in dente. J Endod. 1989;15:323–5. doi: 10.1016/s0099-2399(89)80056-1. [DOI] [PubMed] [Google Scholar]
- 12.Goncalves A, Goncalves M, Oliveira DP, Goncalves N. Dens invaginatus type III: report of a case and 10-year radiographic follow-up. Int Endod J. 2002;35:873–9. doi: 10.1046/j.1365-2591.2002.00575.x. [DOI] [PubMed] [Google Scholar]
- 13.Oehlers FA. Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957;10:1204–18. doi: 10.1016/0030-4220(57)90077-4. contd. [DOI] [PubMed] [Google Scholar]
- 14.Borges AH, Semenoff Segundo A, Nadalin MR, Pedro FL, da Cruz Filho AM, Sousa-Neto MD. Conventional Treatment of Maxillary Incisor Type III Dens Invaginatus with Periapical Lesion: A Case Report. ISRN Dent. 2011;2011:257609. doi: 10.5402/2011/257609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Hamasha AA, Alomari QD. Prevalence of dens invaginatus in Jordanian adults. Int Endod J. 2004;37:307–10. doi: 10.1111/j.0143-2885.2004.00797.x. [DOI] [PubMed] [Google Scholar]
- 16.Ekman-Westborg B, Julin P. Multiple anomalies in dental morphology: macrodontia, multituberculism, central cusps, and pulp invaginations.Report of a case. Oral Surg Oral Med Oral Pathol. 1974;38:217–22. doi: 10.1016/0030-4220(74)90059-0. [DOI] [PubMed] [Google Scholar]
- 17.Ruprecht A, Sastry KA, Batniji S, Lambourne A. The clinical significance of dental invagination. J Pedod. 1987;11:176–81. [PubMed] [Google Scholar]
- 18.Ireland EJ, Black JP, Scures CC. Short roots, taurodontia and multiple dens invaginatus. J Pedod. 1987;11:164–75. [PubMed] [Google Scholar]
- 19.Chen RJ, Yang JF, Chao TC. Invaginated tooth associated with periodontal abscess. Oral Surg Oral Med Oral Pathol. 1990;69:659. doi: 10.1016/0030-4220(90)90256-r. [DOI] [PubMed] [Google Scholar]
- 20.Mader CL, Zielke DR. Incomplete dens in dente in a fused tooth. Oral Surg Oral Med Oral Pathol. 1982;53:439. doi: 10.1016/0030-4220(82)90451-0. [DOI] [PubMed] [Google Scholar]
- 21.Ruprecht A, Batniji S, Sastry KA, el-Neweihi E. The incidence of dental invagination. J Pedod. 1986;10:265–72. [PubMed] [Google Scholar]
- 22.de Sousa SM, Bramante CM. Dens invaginatus: treatment choices. Endod Dent Traumatol. 1998;14:152–8. doi: 10.1111/j.1600-9657.1998.tb00830.x. [DOI] [PubMed] [Google Scholar]
- 23.Ikeda H, Yoshioka T, Suda H. Importance of clinical examination and diagnosis.A case of dens invaginatus. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995;79:88–91. doi: 10.1016/s1079-2104(05)80080-0. [DOI] [PubMed] [Google Scholar]
- 24.Jimenez-Rubio A, Segura JJ, Jimenez-Planas A, Llamas R. Multiple dens invaginatus affecting maxillary lateral incisors and a supernumerary tooth. Endod Dent Traumatol. 1997;13:196–8. doi: 10.1111/j.1600-9657.1997.tb00039.x. [DOI] [PubMed] [Google Scholar]
- 25.Uysal S, Nazikoğlu A, Avcu N, Müftüoğlu S. Dens in Dente and Fusion Occuring in Two Supernumerary Teeth: Report of An Unusual Case. Hacettepe Dişhekimliği Fakültesi Dergisi. 2006;30:54–9. [Google Scholar]
- 26.Cakici F, Celikoglu M, Arslan H, Topcuoglu HS, Erdogan AS. Assessment of the prevalence and characteristics of dens invaginatus in a sample of Turkish Anatolian population. Med Oral Patol Oral Cir Bucal. 2010;15:e855–8. doi: 10.4317/medoral.15.e855. [DOI] [PubMed] [Google Scholar]
- 27.Kirzioglu Z, Ceyhan D. The prevalence of anterior teeth with dens invaginatus in the western Mediterranean region of Turkey. Int Endod J. 2009;42:727–34. doi: 10.1111/j.1365-2591.2009.01579.x. [DOI] [PubMed] [Google Scholar]
- 28.Poyton HG, Morgan GA. Dens in dente. Dent Radiogr Photogr. 1966;39:27–33. [PubMed] [Google Scholar]
- 29.Subay RK, Kayatas M. Dens invaginatus in an immature maxillary lateral incisor: a case report of complex endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:e37–41. doi: 10.1016/j.tripleo.2005.10.056. [DOI] [PubMed] [Google Scholar]
- 30.Lindner C, Messer HH, Tyas MJ. A complex treatment of dens invaginatus. Endod Dent Traumatol. 1995;11:153–5. doi: 10.1111/j.1600-9657.1995.tb00478.x. [DOI] [PubMed] [Google Scholar]
- 31.Pai SF, Yang SF, Lin LM. Nonsurgical endodontic treatment of dens invaginatus with large periradicular lesion: a case report. J Endod. 2004;30:597–600. doi: 10.1097/00004770-200408000-00009. [DOI] [PubMed] [Google Scholar]
- 32.Lichota D, Lipski M, Wozniak K, Buczkowska-Radlinska J. Endodontic treatment of a maxillary canine with type 3 dens invaginatus and large periradicular lesion: a case report. J Endod. 2008;34:756–8. doi: 10.1016/j.joen.2008.01.013. [DOI] [PubMed] [Google Scholar]
- 33.Rodekirchen H, Jung M, Ansari F. Dens invaginatus type II: case report with 2-year radiographic follow-up. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006;102:e121–5. doi: 10.1016/j.tripleo.2005.10.064. [DOI] [PubMed] [Google Scholar]