

Abstract
Aim:
Though many studies have examined cysts of the jaws, most of them focused on a group of cysts and only few have examined cysts based on a particular classification. The aim of this study is to review cysts of the oro-facial region seen at a tertiary health centre in Ibadan and to categorize these cases based on Lucas, Killey and Kay and WHO classifications.
Materials and Methods:
All histologically diagnosed oro-facial cysts were retrieved from the oral pathology archives. Information concerning cyst type, topography, age at time of diagnosis and gender of patients was gathered. Data obtained was analyzed with the SPSS 18.0.1 version software.
Results:
A total of 92 histologically diagnosed oro-facial cysts comprising 60 (65.2%) males and 32 (34.8%) females were seen. The age range was 4 to 73 years with a mean age of 27.99 ± 15.26 years. The peak incidence was in the third decade. The mandible/ maxilla ratio was 1.5:1. Apical periodontal was the most common type of cyst accounting for 50% (n = 46) of total cysts observed. Using the WHO classification, cysts of the soft tissues of head, face and neck were overwhelmingly more common in males than females with a ratio of 14:3, while non-epithelial cysts occurred at a 3:1 male/female ratio.
Conclusion:
This study showed similar findings in regard to type, site and age incidence of oro-facial cysts compared to previous studies and also showed that the WHO classification protocol was the most comprehensive classification method for oro-facial cysts.
Keywords: Classification, Ibadan, oro-facial cysts
INTRODUCTION
A cyst is defined as a pathological cavity which may contain fluid or semi-fluid contents and which is not created by the accumulation of pus.[1] It was initially defined by Killey and Kay as a pathologic epithelium-lined cavity usually containing fluid or semisolid material.[2]
Cysts of the oral and maxillofacial region that are lined by epithelium are known as true cysts, for example, dentigerous cyst; while those not lined by epithelium are generally referred to as pseudo-cysts, for example, the mucous extravasation cyst of the salivary glands, the aneurysmal bone cyst and the solitary bone cyst.[1] Cysts, especially epithelial cysts, are more commonly seen in jaw bones than other parts of the body because of numerous epithelial rests that develop in intimate relationship with developing bone.[3] Various classifications of cysts of the oral and maxillofacial region have been published [Table 1].[2]
Table 1.
Various Classifications of jaw cysts
Though many studies have examined cysts of the jaws, most of them focused on a group of cysts[4–6] and only few have examined cysts based on a particular classification.
The aim of this study was to review cysts of the Oro-facial region seen at a tertiary health centre in Ibadan and attempt to group the cases using the Lucas (1966), the Killey and Kay (1968) and WHO (1992) classification protocols.
MATERIALS AND METHODS
This was a retrospective study of oro-facial cysts seen at the oral pathology department of the University College Hospital Ibadan. All histologically diagnosed oro-facial cysts seen in the department over a 10-year period (1999-2009) were retrieved from the oral pathology archives. Cysts diagnosed as odontogenic keratocysts (OKC) were excluded from the study. Information concerning cyst type, topography, age at time of diagnosis and gender of patients were retrieved.
Data obtained were analyzed with the SPSS 18.0.1 version software. Frequency tables were generated and data was analyzed for gender, age and site. The cases were also analyzed based on the Lucas (1966) the Killey and Kay (1964) and WHO (1992) classifications protocols.
RESULTS
A total of 92 histologically diagnosed oro-facial cysts comprising 60 (65.2%) males and 32 (34.8%) females (1.9:1 male to female ratio) were seen over the study period. The ages of patients ranged between 4 to 73 years with a mean age of 27.99 ± 15.26 years.
Apical periodontal was the most common type of cyst seen in this study accounting for 50% (n = 46) of the total number of cysts seen. Dentigerous cyst was the second most common type of cyst seen (n = 11), representing 12% of total number of cysts; while mucous extravasation cyst, lateral periodontal cyst and calcifying odontogenic cyst, epidermoid cyst and aneurysmal bone cysts accounted for 7.6%, 5.4%, 4.3%, 4.3% and 4.3% of total number of cases seen respectively. Other types of cysts were relatively few in number and all together accounted for 16.4% of the cases seen [Figure 1].
Figure 1.
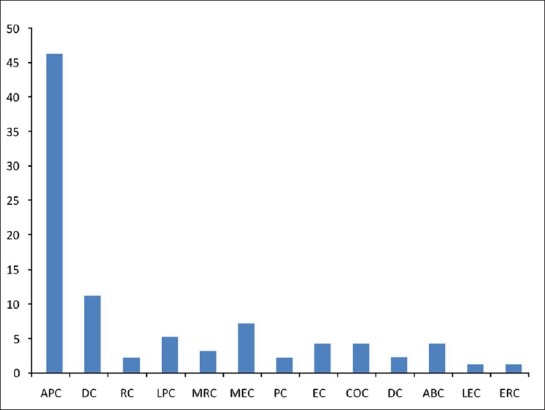
Frequency of Oro-facial cysts. APC – Apical periodontal cyst, DC-Dentigerous cyst, RC-Residual cyst, LPC-Lateral periodontal cyst, MRC-Mucous retention cyst, MEC-Mucous extravastion cyst, PC-paradental cyst, EC-Epidermoid cyst,COC-calcifying odontogenic cyst, DC-Dermoid cyst, ABC- Aneurysmal bone cyst, LEC-Lymphoepithelial cyst, ERC- Eruption cyst.
The peak incidence with 28 (30.4%) occurred in the third decade of life. Majority (78.2%) of the cases occurred in the first four decades while only 21.8% occurred in the fifth decade upwards. Oro-facial cysts were however rare in the seventh and eight decades of life both having a combined occurrence of just 3.3% [Figure 2]. The mandible was the most common site of occurrence with 43 (46.7%) of the cases while 31.5% of the cases occurred in the maxilla giving a mandible/maxilla ratio of 1.5:1. The lower lip, floor of mouth and palate accounted for 9.8%, 3.3%, and 2.2%, respectively.
Figure 2.
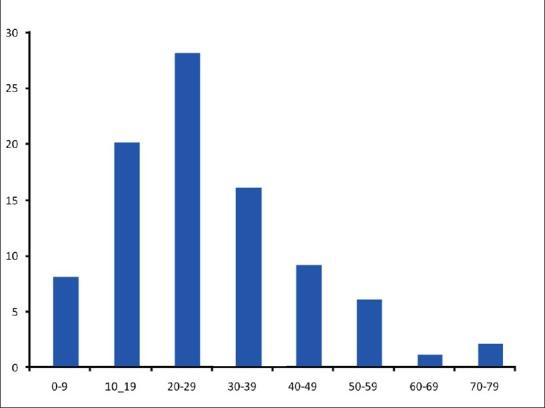
Age group distribution of Oro-facial cysts
Tables 2–4 show oro-facial cysts distribution based on the Killey and Kay, Lucas and WHO classifications, respectively. According to the Killey and Kay classification, cysts arising from epithelial rests were the most common accounting for more than half (59.8%) of cases while cysts derived from reduced enamel epithelium represented only 13% of cases seen. Pseudo cysts accounted for 4.3% of cases and 18.5% were not classifiable by the Killey and Kay classification. Most of the cysts under this classification were more common in men but pseudo cysts occurrence was significantly higher in females than males with a ratio of 3:1 [Table 1].
Table 2.
Oro-facial cysts distribution according to Killey and Kay classification
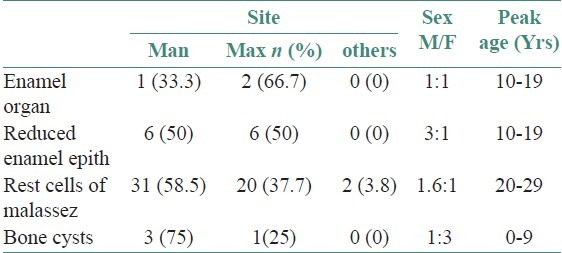
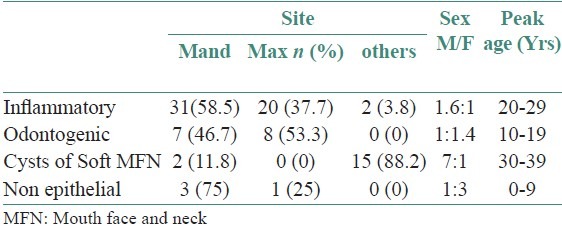
Table 4.
Oro-facial cysts distribution according to WHO classification
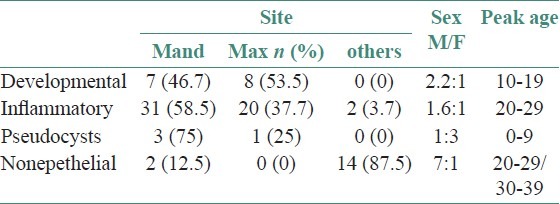
According to the Lucas classification, inflammatory cysts were the most common accounting for 59.8% while 17.4% were classified as developmental, 17.4% were non-epithelial and 1.1% was not classifiable by this method. Non-epithelial cysts occurred almost exclusively in men with a 7:1 male/female ratio.
The WHO classification showed that inflammatory cysts were the most common accounting for 59.8% (similar to Lucas), cysts of soft tissue of MFN were 18.5% odontogenic cysts were 17.4%, while no cyst was left unclassified by this protocol. Under the WHO classification, cysts of the soft tissues of head, face and neck (dermoid, epidermoid and lymphoepithelial cysts and salivary gland cysts) were overwhelmingly more common in males than females with a ratio of 14:3 but non-epithelial cysts were more common in females than males with a ratio of 3:1 [Table 3].
Table 3.
Oro-facial cysts distribution according to Lucas classification
DISCUSSION
The number of cases reported in this study is lower than other similar studies partly because OKC were excluded from this study since it is currently regarded as a benign tumor. The World Health Organization (WHO) in 2005 reclassified OKC as an odontogenic tumor (OT) derived from odontogenic epithelium with mature, fibrous stroma without odontogenic ectomesenchyme and renamed it keratocystic OT.[7] The relatively small number of cases seen may also be due to the fact that apical periodontal cyst may have been underreported because many cases especially smaller ones are now routinely treated by root canal therapy without histological examination.
Inflammatory cysts were the most common cyst in this study accounting for 59.8% of all cysts seen while development cysts represented mainly by dentigerous cyst were 17.4% of all cysts seen. This is mainly due to the preponderance of apical periodontal cyst which alone accounted for 50% of all the cysts seen. This is in agreement with other studies,[6,8,9] which have shown that inflammatory cysts represented mainly by apical periodontal cyst were the most common type of cyst. El Gehani[10] in Libya, Koseolu[11] in Turkey and Arotiba[6] in Ibadan reported that inflammatory cysts accounted for 68.1%, 59%, and 61.9% of all the odontogenic cysts seen respectively. However, in a study in Lagos, Ogunlewe[3] reported that inflammatory cyst represented only 27% of epithelial jaw cysts while developmental cysts accounted for 73% of epithelial cysts. The mean age occurrence of cysts in this study was 27.99 years and mode was in the third decade of life. Other studies have reported peak age incidence in 21-30,[3] 21-50[10] and 33 years[5] but Arotiba[6] reported peak age incidence in second decade of life.
Oro-facial cysts were more prevalent in the mandible than maxilla (1.5:1). This is similar to the findings of ogunlewe[3] in Lagos although they reported 1.1:1 mandible/maxilla ratio but it is at variance with libyan[10] and lithuanian[5] studies that reported mandible/maxilla ratios of 1:1.3 and 1:1.5 respectively.
Although the Killey and Kay classification showed the cells of origin of the different types of cysts, a total of 18.5% were unclassified as salivary gland cysts were not considered by this protocol. The Lucas and WHO classifications both focused on the etiologic process of the individual cysts and only 1.1% (Lymphoepithelial cyst) of the cysts in this study were not classified by the Lucas classification protocol. The WHO classification appears to be the most inclusive of the three classification protocols as all cysts seen in this study were classified by this protocol.
The results from this study showed similar findings in regard to type, site and age incidence of oro-facial cysts compared to previous studies and also showed that the WHO classification protocol the most comprehensive classification method for oro-facial cysts.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Shear M, Speight P. Classification and frequency of Cysts of the Oral and Maxillofacial tissues. In: Shear M, Speight PM, editors. Cysts of the Oral and Maxillofacial regions. Singapore: Blackwell; 2007. pp. 11–2. [Google Scholar]
- 2.Malik AH, Ajaz AS, Suhail L, Manzoor AM, Rubeena T, Shazia Q, et al. Cysts of the maxillofacial region. [Last accessed on 2010 Sept 11]. Available from: http://www.articlesbase.com/medicine-articles/cystsof-maxillofacial-region-1556366.html#ixzz0wyCjqT4u .
- 3.Ogunlewe MO, Odukoya O, Akinwande JA. Epithelial jaw cysts: Analysis of 126 Nigerian cases. Afr Dent J. 1996;10:1–8. [PubMed] [Google Scholar]
- 4.Yazdani J, Kahnamouii S. Developmental Odontogenic Cysts of Jaws: A Clinical Study of 245 Cases. J Dent Res Dent Clin Dent Prospect. 2009;3:64–6. doi: 10.5681/joddd.2009.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lawal AO, Adisa AO, Sigbeku OF. Cysts of Oro-facial region : A Nigerian experience. J Oral Maxilofac Pathol. 2012;16:167–71. doi: 10.4103/0973-029X.98448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Arotiba JT, Lawoyin JO, Obiechina AE. Pattern of occurrence of odontogenic cysts in Nigerians. East Afr Med J. 1998;75:664–6. [PubMed] [Google Scholar]
- 7.Gaitan-Cepeda LA, Quezada-Rivera D, Tenorio-Rocha F, Leyva-Huerta ER. Reclassification of odontogenic keratocyst as tumor Impact on the odontogenic tumors prevalence. Oral Dis. 2010;16:185–7. doi: 10.1111/j.1601-0825.2009.01625.x. [DOI] [PubMed] [Google Scholar]
- 8.Kreidler JF, Raubenheimer EJ, Vanheerden WF. A retrospective analysis of 367 cystic lesions of the jaw- the Ulm experience. J Craniomaxillofac Surg. 1993;21:339–41. doi: 10.1016/s1010-5182(05)80494-9. [DOI] [PubMed] [Google Scholar]
- 9.Wakoli RA, Bhaji AF. A retrospective study of jaw cysts in a Kenyan Hospital. Afr Dent J. 1987;1:19–22. [Google Scholar]
- 10.El Gehani R, Krishnan B, Orafi H. The prevalence of inflammatory and developmental odontogenic cysts in a libyan population. Libyan J Med. 2008;3:75–7. doi: 10.4176/071216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Koseoglu BG, Atalay B, Erdem MA. Odontogenic cysts: A clinical study of 90 cases. J Oral Sci. 2004;46:253–7. doi: 10.2334/josnusd.46.253. [DOI] [PubMed] [Google Scholar]